
Abstract
Abstract
Purpose:
To evaluate the natural course of the eyes with macular edema secondary to branch retinal vein occlusion (BRVO) and to compare the visual outcome and macular thickness with eyes treated with intravitreal injection of triamcinolone acetonide (IVTA) and intravitreal injection of bevacizumab (IVB).
Methods:
We reviewed the medical records of the patients with macular edema secondary to BRVO who were followed over 12 months. We evaluated the best corrected visual acuity (BCVA) and central macular thickness (CMT) of the patients who have had no treatment for macular edema (natural course group) and compared the BCVA and CMT of the patients who had been treated with IVTA or IVB.
Results:
BCVA and CMT of the natural course group improved in a slow, but steady manner. The IVTA and the IVB group showed temporary improvement after injection, but macular edema recurred and there was no significant difference in the visual outcome and macular thickness after 6 months.
Conclusions:
Although IVTA and IVB were effective to decrease the macular edema at 1 month after the injection in BRVO. BCVA and CMT of the natural course group were not inferior to both the IVTA and the IVB groups at 12 months.
Introduction
Generally, natural course and visual prognosis of BRVO is known to be favorable.5–8 However, retinal hemorrhage, vitreous hemorrhage, tractional retinal detachment, and macular ischemia due to BRVO lead to decreased visual acuity. 9 Of these, macular edema is the most common cause of decreased visual acuity. 10
Several modalities have been explored in the treatment of macular edema. Until now, the only evidence-based therapy for BRVO is argon laser photocoagulation. 10 Currently, several studies have demonstrated the usefulness of intravitreal injection of triamcinolone acetonide (IVTA)11–13 and of anti-vascular endothelial growth factor (anti-VEGF) agents, such as intravitreal injection of bevacizumab (IVB)14,15 and ranibizumab16,17, in dealing with macular edema due to BRVO. However, some studies have shown that effectiveness of IVTA was not maintained after 1 year despite repeat injections. 18 Another study reported that IVTA and IVB injections were similarly effective for BRVO-related macular edema, but the IVTA group showed a longer mean improvement duration than the IVB group. 19
While IVTA and IVB injections, as mentioned above, have been widely studied, there was no study of natural course of BRVO except the Branch vein occlusion study (BVOS), which was published more than 25 years ago.
Therefore, it was the purpose of the present investigation to assess the natural course of the visual acuity and central macular thickness (CMT) in patients with macular edema due to BRVO and to compare the visual outcomes with the patients receiving either triamcinolone or bevacizumab.
Subjects and Methods
The medical records of 76 patients with macular edema secondary to BRVO who visited the Hallym University Sacred Heart hospital were analyzed retrospectively. Only patients with CMT of ≥250 μm, a follow-up period ≥12 months were included in this study. The patients who already had other treatments, such as vitrectomy, macular laser treatments, or other intravitreal injections were excluded. Eyes with other diseases affecting the best corrected visual acuity (BCVA) or the presence of neovascularization were also excluded in this study. However, the patients who received the peripheral scatter laser photocoagulation were included.
We did not perform the macular grid laser for macular edema because of the poor visual outcome associated with side effects, such as paracentral scotoma. All patients with macular edema were recommended to be treated with either intravitreal triamcinolone or bevacizumab after informed consent was obtained and received the injection within 1 week, but some of the patients refused the intravitreal injection because of the risk of complications, financial difficulty, certain personal reasons, and so on.
Intravitreal injections were performed under sterile conditions. Topical anesthetic drops were instilled, cleaning of the injection site with 5% povidone iodide, and a 30-gauge needle was inserted through the pars plana 4 mm posterior to limbus. The dose was 4.0 mg of triamcinolone or 1.25 mg of bevacuzimab. Following the injection, an antibiotic ointment was administered and the eye was patched overnight. After intravitreal injection, patients were prescribed to administer a topical antibiotic eye drop for 3 days routinely and monitored for potential injection-related complication at 1, 3, and 7 days after injection.
For all patients, the follow-up visits were scheduled every month. Baseline and follow-up examinations for comparison of each group were performed 1, 3, 6, 12 months after the day of recommendation of treatment, which is a reference date for the comparison of the natural course group with the IVTA and the IVB group. Follow-up examinations included ophthalmologic examination, BCVA, and an optical coherence tomography (OCT, Stratus OCT; Carl Zeiss Meditec, Dublin, CA) examination. Macular thickness more than 300 μm, or macular thickness that increased by 100 μm since the last examination, were criteria for reinjection.
The minimum time intervals between injections were 6 weeks for bevacizumab and 8 weeks for triamcinolone. We evaluated the BCVA and CMT of the patients who have had no treatment for macular edema (natural course group) and compared them with the patients who had been treated under the parameters of the IVTA group and IVB group. Since Fluorescein angiography (FA) is not very informative during the early period of BRVO because of the presence of blocked fluorescence due to retinal hemorrhage, FA was taken at about 6 months after BRVO when the retinal hemorrhage had cleared up. The patients who did not show visual improvement despite the improvement of retinal thickening were candidates for FA.
For statistical analysis, the BCVA were converted to the logarithm of the minimum angle of resolution (log MAR). Baseline demographics were compared using the Kruskal–Wallis test and the χ2 test.
A comparison of differences between follow-up and baseline data within each group was performed using the Wilcoxon Matched-Paired signed rank test, and further comparison among each group was performed for any follow-up visits by repeat measurement analysis after adjusting age, sex, reinjection, and so on. Statistical analysis was performed with SPSS for windows, version 13 (SPSS, Inc., Chicago, IL) and the level of statistical significance was set at P<0.05.
This study was done in adherence to the tenets of the Declaration of Helsinki and informed consent was obtained. Approval for this study was obtained from the Institutional Review Board.
Results
Among the total of 76 patients, 27 patients underwent IVTA (IVTA group), 18 patients IVB injections (IVB group), and 29 patients were followed regularly without any treatment except peripheral scatter laser (natural course group). None of the patients developed immediate injection-related complications, such as uveitis, endopthalmitis, or a thromboembolic event.
At baseline, 3 groups did not differ in age (P=0.245), BCVA (P=0.380), and CMT (P=0.353) (Table 1). Mean duration of symptoms before reference date were 78.33±70.67, 126.47±94.58, and 62.45±57.30 days in IVTA, IVB, and natural course group, respectively. The mean number of injections per eye within 1 year was 1.63 in the IVTA group, and 1.39 in the IVB group.
Kruskal–Wallis test (P<0.05).
χ2 test (P<0.05).
IVTA, intravitreal injection of triamcinolone acetonide; IVB, intravitreal injection of bevacizumab; BCVA, best corrected visual acuity; CMT, central macular thickness.
At 1 month after injection, both IVTA and IVB groups showed a significant reduction of CMT (P<0.001). After 3 months, all groups showed a significant reduction of CMT (P<0.001) and maintained until final follow-up. In the among-group comparison, both IVTA and IVB groups showed a significantly lower thickness than the natural course group at 1 month (Kruskal–Wallis test, P=0.001), but no significant difference was revealed at the 12-month follow-up visit (repeated measurement analysis, P=0.139) (Fig. 1A). Mean macular thickness reduction rates were 60.5%, 55.5%, and 55.9% in the IVTA, IVB, and natural course group, respectively (Table 2). When it comes to visual acuity, only the natural course group showed improvement after 6 months compared to baseline (P<0.001), while other groups did not. In the among-group, a comparison revealed that the natural course group showed significant improvement at 12 months (repeated measurement analysis, P=0.024) (Fig. 1B). Twelve months after the reference date, 16 of 29 eyes (55.2%) in the natural course group had an improvement of visual acuity ≥0.3 log MAR units, while 8 of 27 eyes (29.6%) and 6 of 18 eyes (33.3%) showed improvement in the IVTA and IVB group, respectively. We also found that 23 eyes (79.3%) showed visual acuity of 20/40 or better in natural course, while 7 eyes (25.9%) and 5 eyes (27.8%) in the IVTA and IVB group, respectively, at final follow-up. Two (6.9%), 6 (20.7%), and 4 eyes (22.2%) showed visual acuity of 20/200 or worse in the natural course, IVTA, and IVB group at final follow-up, respectively (Table 2). The FA showed that 7 eyes (58.3%) among 12 eyes with visual acuity of 20/200 or worse in all groups showed the increased or irregular margin of foveal avascular zone, which is compatible with ischemic maculopathy.
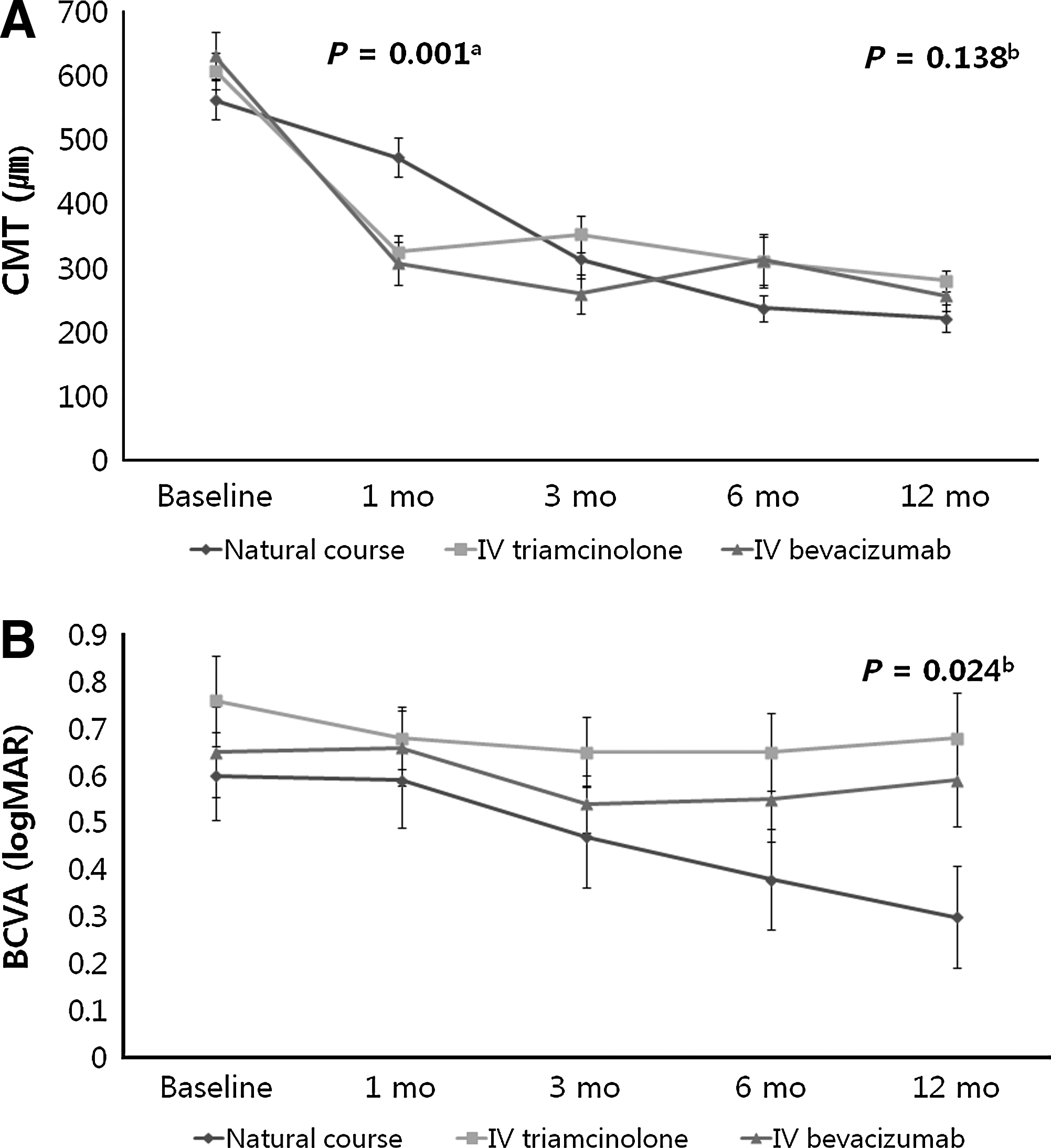
Changes of central macular thickness (CMT)
χ2 test (P<0.05).
After exclusion of these 7 eyes with ischemic maculopathy, we re-evaluated the BCVA and CMT of each group. The results were similar to those without exclusion. Both IVTA and IVB groups showed a significantly lower thickness than the natural course group at 1 month (Kruskal–Wallis test, P=0.003), but no significant difference was revealed at any other follow-up visit (repeated measurement analysis, P=0.148) and there was no significant difference in BCVA among all groups at any follow-up visit (repeated measurement analysis, P=0.141) (Fig. 2).
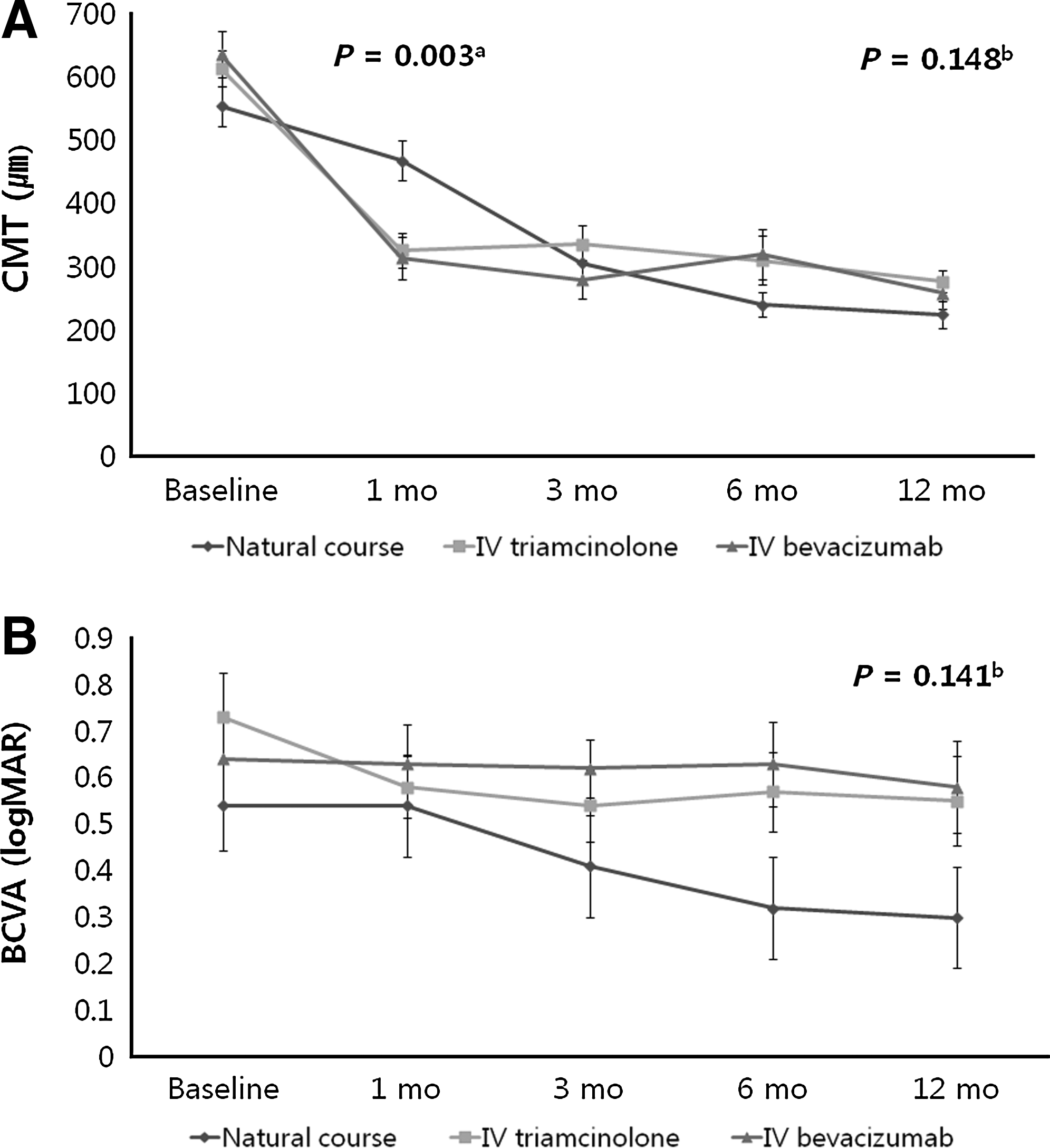
Changes of CMT (central macular thickness,
The macular edema recurred in 11 eyes with the IVTA group and 7 eyes with the IVB group during the follow-up period. The mean recurrence time from previous injection was 20.83 weeks in the IVTA group and 24.14 weeks in the IVB group. Kaplan-Meier survival analysis of macular edema recurrence in the IVTA and IVB group showed no difference in time and number of recurrence (P=0.613) (Fig. 3).

Kaplan-Meier survival analysis of macular recurrence in IVTA and IVB group. IVTA, intravitreal injection of triamcinolone acetonide; IVB, intravitreal injection of bevacizumab.
Until the end of follow-up, an elevated intraocular pressure was seen in 2 eyes of the IVTA group and controlled by topical therapy. A quick progression of cataract was noted in 4 eyes of the IVTA group, but was not serious to receive cataract surgery. There was no remarkable complication in the IVB group.
Discussion
The natural course of BRVO is reported to be favorable. 50%–60% of patients with untreated BRVO had a final visual acuity of 20/40 or better without any treatment.5–8 However, the visual outcome of untreated eyes was less favorable in BVOS, 37% of untreated eyes followed for 3 years gained ≥2 lines of vision from baseline maintained for at least 2 consecutive study visits and 65% had gained ≥2 lines of vision with the macular grid laser treatment group 10 . In laser-treated eyes, the average improvement of visual acuity was 1.3 lines from baseline, 40% of eyes ended up with visual acuity of 20/40 or better, and 12% remained with visual acuity of 20/200 or worse. After BVOS, macular grid photocoagulation became the only evidence-based effective treatment modality for macular edema in BRVO. However, paracentral scotoma is one of the unfavorable side effects and laser is not suitable if there is retinal hemorrhage.
To overcome these limitations, a number of treatment modalities have been described.
IVTA or IVB have been widely used and reported for their efficacies. It has been claimed that IVTA reduces the permeability effect of VEGF, and thereby reduces the leakage of osmotically active molecules from the vessel into the tissue. 20 IVB directly inhibits VEGF, reduces vascular leakage, eliminates retinal and subretinal fluid, and improves the hypoxic condition. However, the efficacy of IVTA or IVB is still controversial. In the Standard of Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study, there was no difference in the visual outcome between the standard care group and the IVTA group for macular edema secondary to BRVO at 12 months. 21 Moreover, adverse events, such as elevated intraocular pressure and cataract, were reported in the IVTA group. In addition, frequent repeated injections are required for recurrent macular edema after IVTA or IVB, which increase the risk of complication associated with intravitreal injection, such as endopthalmitis. That means, there is no satisfactory modality for macular edema secondary to BRVO until now.
When it comes to BVOS again, BVOS involved only 35 untreated eyes and different BRVO durations from 3 to 18 months were included together, and determined the natural course of BRVO. Because the BVOS reported grid laser photocoagulation to be the standard care for BRVO eyes with macular edema, no natural history information for such eyes can be ascertained from the SCORE study or OZURDEX GEVEVA (Global Evaluation of implaNtable DexamEthasone in retinal Vein occlusion with macular edema) because all eyes in the standard of care group received grid laser before or after study entry.21,22 Therefore, more than 25 years after BVOS, there have been no reliable studies about the natural history of BRVO.
In our study, we evaluated the natural course of BRVO with patients who were treatment-naïve and followed for more than 12 months, and compared the visual outcome of the eye treated with other modalities (IVTA, IVB). We found 2 distinguishable facts compared with previous studies. First, in BVOS, 13 eyes (37%) gained 2 or more lines of vision and 6 eyes (17%) lost 2 or more lines of vision among untreated 35 eyes, while 16 eyes (55.2%) gained 3 or more lines of vision and no one lost 3 or more lines of vision in our study. We assumed that a better visual outcome in our study could be due to the difference of inclusion criteria. Because we included the subjects according to the macular thickness using OCT, the patients with visual acuity better than 20/40 were included. Another reason we thought that the better visual outcome of natural course in the current study than in BVOS is thanks to the improvement of medical and social environment. Compared with 25 years earlier, there have been many improvements in pharmacology, which made it possible to control underlying disease, such as hypertension or diabetes, more easily. Accompanying medical advances, social environment also improved so that the compliance of patients became better, which, as a result, could make a better clinical course for BRVO.
Secondly, it looked like there was a beneficial effect of IVTA or IVB right after the injection, but macular edema recurred several months after the injections. Consequently, there were no significant differences in macular thickness after 6 months.
Definitely, there could be the possibility of selection bias, such as macular perfusion status because we did not perform FA in all patients. Shroff et al. 23 reported that the anatomical and functional outcome could be different according to macular perfusion status. In natural course of BRVO, BCVA increases from 0.09 to 0.17 in the nonischemic type and remains stable in the ischemic type at 6 months. In our study, 7 eyes (58.3%) with visual acuity of 20/200 or worse showed ischemic maculopathy in FA and only 1 eye in the natural course group, while 4 eyes in the IVTA group. Therefore, there was a possibility of selection bias that more patients with nonischemic type of BRVO were included in the natural course group than other groups. After exclusion of the eyes with ischemic maculopathy, it showed a similar result in macular thickness, but BCVA became no statistically different among 3 groups at 12 months (Fig. 2).
Even though the possibility of selection bias and small number of subjects are the main limitations of this study, it is still a meaningful report and this is the first report of natural history of macular edema due to BRVO after BVOS to the best of our knowledge. Therefore, this report may help to understand the clinical course of BRVO according to the treatment modality. Surely, in the future, studies with a larger sample size and longer follow-ups are necessary to decide the optimal treatment modality for macular edema in BRVO.
In conclusion, even though IVTA and IVB were effective to decrease the macular edema at 1 month after the injection in BRVO, there was no significant difference in the visual outcome and macular thickness with natural course after 6 months until the end of follow-up visits in nonischemic maculopathy patients. That means that natural course of BRVO was not inferior to both IVTA and IVB treatments until 12 months. Therefore, close observation without any treatment could be another option for the patients who are contraindicated for intravitreal injection or macular grid laser treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.