
Abstract
Abstract
Purpose:
The aim of this study was to evaluate by serial measurements, pupil mydriasis produced by topical application of tropicamide 1% using a spray in a closed eye or instillation in an open eye in adult and elderly populations.
Methods:
The research was done from February to April of 2011 in the Policlinica Ronaldo Gazolla, located in the Arcos da Lapa Campus of Estacio de Sá University, RJ- Brazil. It was a clinical trial, controlled and randomized, made in a series of 50 patients that were being prepared for ophthalmoscopy examination. They were submitted to eye drop administration of 1% tropicamide in an open eye and to eyelid margin vaporization in a closed eye. The eyes were chosen for the administration of drops or spray according to a pseudo-random numbers table from Excel (2007) before application. The pupil diameter was measured before instillation and after 10, 20, and 30 min in both eyes, with a millimeter ruler. Biostat 5.0 software was used for statistical calculations.
Results:
Tropicamide 1% was vaporized in a group that presented the following average pupil diameters: 3 mm before the application; 4.16 mm in 10 min; 5 mm in 20 min; and 5.35 mm in 30 min. The group in which tropicamide 1% was instilled presented 2.96 mm of average pupil diameter before the application; 4.22 mm at 10 min; 5.02 mm at 20 min; and 5.44 at 30 min. The two way analysis of variance showed P<0.0001, and the Tukey test performed for comparisons among the groups showed statistical significant differences among all groups except when the measurements were done at the same time.
Conclusion:
The vaporized tropicamide 1% mydriatic effect in closed eyes was clinically equivalent to the instillation effect of eye drop in open eyes. Other mydriatic drugs sprayed in closed eyes may not have the same effect.
Introduction
Patients may instill tropicamide in their eyes for therapeutic purposes, but this drug can also be instilled by a family member in patients who are outside the medical environment and have diseases that impair fine motor coordination, cognition or vision (blindness). 3 The use of the drug applied at distance by spray with the eye previously closed can be useful as an alternative to traditional instillation when it is difficult to accomplish it due to pre-existing diseases. 4 Patients with lid inflammations, like the ones that have blepharohematomas or facial cellulitis may feel pain during topical application, when a finger touches their eyelids. Instillation may also be affected by the reduction of eyelid opening that occurs in these diseases or facial dystonias. It is likely that persons who will benefit most from this method of application will be the adult or elderly patients who possess normal vision and feel very anxious or nervous when they sense the eye drop contact with open eyes. They often move the head or eye and blink excessively when someone comes and presses the eye drop bottle near their face. This behavior prevents the eye drop to fall into the proper position in the tear film and may also lead to bottle tip touch on the eye.
Several authors have demonstrated that the incorrect use of eye drops may cause increased systemic absorption of the active ingredient, resulting in higher toxicity.5,6 Misuse of eye drops can also occur when, for technical error, the tip of the bottle has direct contact with the ocular surface, this contact can cause bottle contamination. The procedure is also incorrect when a caregiver of a patient uses excessive number of drops per application or excessive number of applications. 7
The instillation of eye drops often produces symptoms such as burning, stinging, and tearing. According to Stillitano et al. (2005), this procedure becomes even more complicated to be done in children because they have greater difficulty keeping eyes open and unpleasant feelings are exacerbated. 8
An important factor that leads patients not to adhere adequately to treatment is incorrect drop instillation that raises the cost of therapy. An example is the chronic treatment of glaucoma. In 2005, Stillitano et al. found a wide variation in the average daily cost of glaucoma treatment. There was daily variation of R$ 0.077 for generic timolol maleate (cheaper) to R$ 1.910 for Xalacom® (more expensive). If we focus on the possibility of constant loss by multiple incorrect applications, that figure could double by the need to buy a second bottle. 8
There are few studies demonstrating the tropicamide efficacy when it is sprayed topically onto the eye. When the spray is applied with the patients' eyes closed, the ophthalmic solution droplets are placed under pressure between the lashes so that when the patient opens his/her eyes, they mingle in the tear film. In Brazil, only one study was published in 2006, which used a spray with open eyes. 9 After an extensive search in PubMed, SciELO, and LILACS, the authors didn't find articles that evaluated the tropicamide mydriatic effect on adults or elderly closed eyes. However, we found articles about tropicamide vaporization on children closed eyes. 10 Therefore, the method tested should also be validated in adult and elderly patients.
The aim of this study was to evaluate by serial measurements, pupil mydriasis produced by topical application of tropicamide 1% using spray in a closed eye or instillation in an open eye in adult and elderly patients. Other medications sprayed in closed eyes may not have the same effect. Additional studies are needed to assess this issue.
Methods
The research was done from February to April of 2011 in the Policlinica Ronaldo Gazolla, located in the Arcos da Lapa Campus of Estacio de Sá University, RJ- Brazil. It was a clinical trial, controlled and randomized, made in a series of 50 patients that were being prepared for ophthalmoscopy examination in the ophthalmological department. They were submitted to eye drop administration of 1% tropicamide in an open eye and to eyelid margin vaporization in a closed eye.
The research was done in accordance to the tenets of The Declaration of Helsinki. Informed consent was obtained for all patients studied, and the research was approved by the Institutional Review Board.
The eyes were chosen for the administration of drops or spray according to a pseudo-random numbers table from Excel (2007) before application. The pupil diameter was measured before instillation and in 10-, 20-, and 30-minute increments in both eyes, with a millimeter ruler.
We used a bottle of eye drops solution tropicamide 1% (Mydriacyl®) and a bottle of the same solution coupled to a vaporizer. The vaporizer had a plastic mist spray pump (screw version).
Exclusion criteria:
(1) Anisocoria and/or any change in pupil diameter.
(2) Presence of any systemic disease that affects the autonomic nervous system.
(3) Presence of posterior synechiae.
(4) Presence of inflammatory eye diseases.
(5) Presence of eye disease that prevents the pupil diameter measurement.
The eye drop was applied by one of the authors into one of the patient's eyes, always in the same way: the patient was instructed to direct the head back, making a neck extension, and looking up. His lower eyelid was slightly pulled, exposing the lower conjunctival fornix, where a drop was instilled.
The vaporization was made on the other eye, as follow: The patient was instructed to remain seated and look ahead. Then, the bottle was placed by one of the authors directly toward the nasal part of the eyelids while closed, about 3 cm away from the patient eye, and the drug was sprayed just once. The whole process was made quickly and dexterously. The bottle used was made of plastic with 7-cm height and 2-cm large, with a total volume of 7 mL. This flask was adapted for eye drop instillation, so it was sterilized with ethylene oxide before the study, and tropicamide 1% was introduced in it in a sterile way. One single-spray vaporization volume was equivalent to 2 eye drops. The tropicamide 1% spray dispersion area was 3 cm in horizontal diameter and 2.5 cm in vertical diameter at 3-cm distance.
Tropicamide application and pupil diameter measurements were done by students in the last year of medical school and supervised by Prof. Dr. Arlindo Portes. On Tuesdays, a student measured the pupil diameter and then applied tropicamide in patients. At 10, 20, and 30 minutes, another student measured the pupil diameter blindly. The process was repeated on Thursday by another pair of students. Ophthalmoscopic examinations were scheduled in Policlinica Ronaldo Gazola always and only on Tuesday and Thursdays.
At the end of 30 minutes, after the last pupil diameter measurement, all patients who complained of ocular discomfort underwent biomicroscopical examination to discard any corneal or eyelid modification. No study patient complained of nasal symptoms after tropicamide application.
Results
The average age of patients was 61.5 years and standard deviation was 11.7. Twenty patients (40%) were men and 30 (60%) were women.
In Table 1, the average pupil diameter of each group was observed at the same times. There were no clinically significant pupil diameter differences between the groups measured at the same times.
Mydriasis evolution is demonstrated in Figure. 1. Except for one outlier measurement in the group of eyes vaporized, observed at 30 min, the average pupil diameter and standard pattern deviation is very similar for each group.
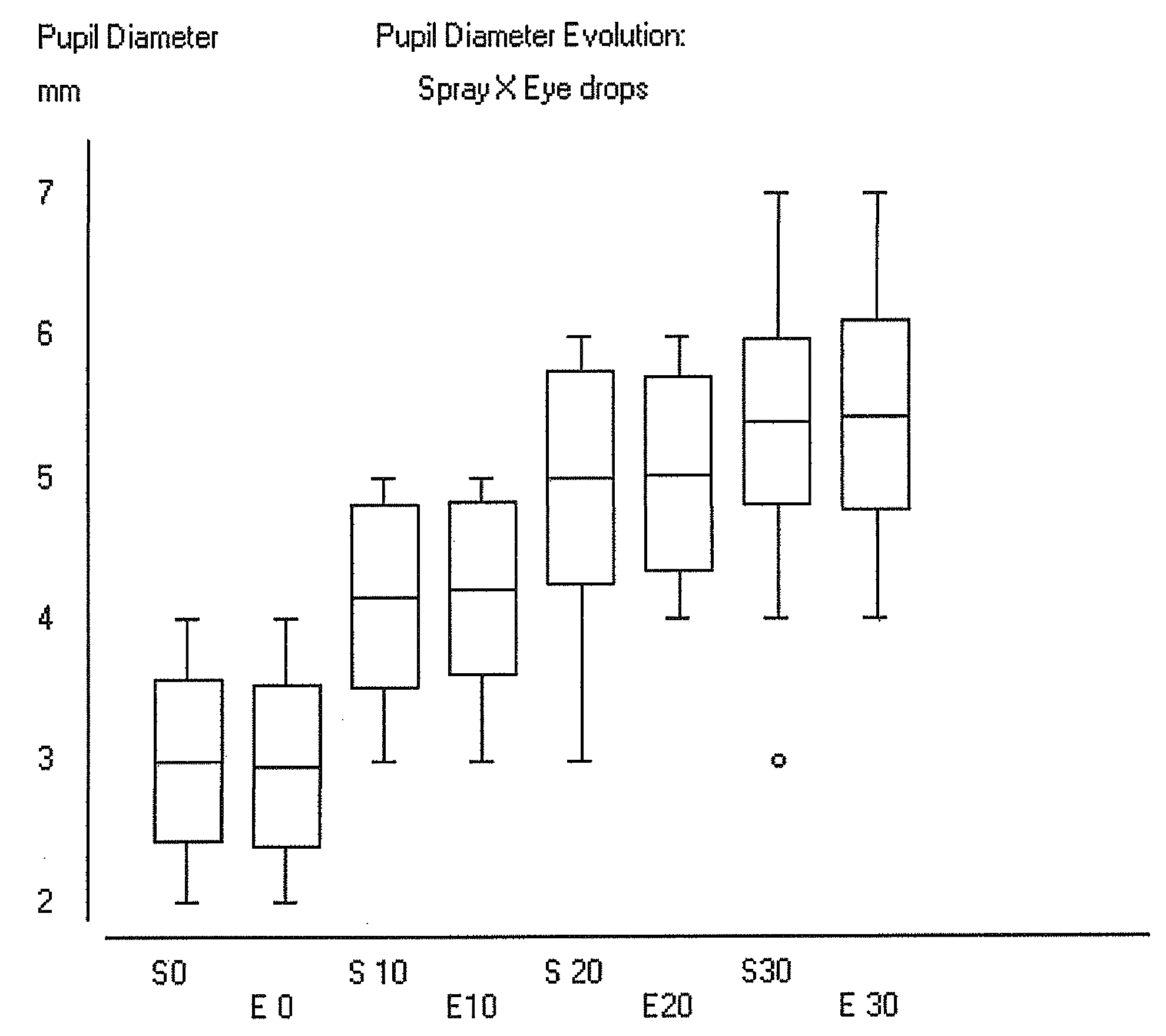
Pupil diameter evolution in a box plot graphic of eyes that were submitted to spray (S) and eye drop application (E) at 0, 10, 20, and 30 min. The box was plotted with data average and one standard deviation. The whiskers indicate maximum and minimum values. An outlier is observed in the group S30.
The two-way analysis of variance showed P<0.0001 for all groups. The F value (treatment)=244.1573 and the F value (blocks)=9.9155.
The Tukey test was performed on data for comparisons among all groups studied. Average mydriasis comparisons among measurements at different times showed statistically significant difference for all comparisons. Average mydriasis comparisons between measurements made at same times showed no statistical significance for all comparisons.
Discussion
The study conducted by Wong in China in 2003, compared the efficacy and tolerance of mydriatic and cycloplegic application as spray in closed eyes versus instillation of eye drops in Chinese childrens' open eyes. The study showed that the vaporization of the drug has an effect on pupillary dilation and cycloplegia similar to instillation of drops. However, more acceptance and tolerability were noted as vaporization with eyes closed. 10 In our study, although we have not evaluated tolerability, we found similar results on the mydriatic effect on adults and the elderly. The chronic use of drugs in adults or the elderly occur in a greater way than in children.
Tavares and Portes (2006) showed no difference in clinically and statistically significant mydriatic effect of tropicamide 1% applied as instillation, compared with the form of vaporization with open eyes. 9 In our study, we observed similar results on the effect of mydriasis produced by tropicamide, but with the eyes closed in vaporization. This effect can be produced due to the release of active pressure causing accumulation of vaporized droplets on the eyelid margin, which mix with the tear film when the eyes open. Excessive tearing, cleaning of the eyelashes, or the edge of the eyelid may impair the absorption of the medication and explain outliers. It is important to notice that each spray application in this study delivered a volume equivalent to two eye drops; therefore, the method described would be probably more expensive than eye drop instillation alone.
A study conducted in 2008 and 2009 by Portes et al., evaluated the perception of topical drugs sprayed in the eye compared with the instillation of drops. The patients noted that the instillation of drops was easier as compared to the vaporization of the open eye. However, the perceived ease was due to technical failure to support the tip of the bottle in the eye tissues. Vaporization was the safest method to avoid contamination of the bottle. 11 Perhaps, the level of comfort and ease of vaporization with eyes closed is greater than eye drop instillation with the eye open. However, this should be a theme for future study.
In 2009, Khaireddin and Schmidt compared the efficacy of the treatment of dry eye using sodium hyaluronate instillation of drops versus spray of phospholipid liposome on closed eye in 216 patients. They concluded that both forms of administration were effective, and therapy with a vaporizer obtained more significant results, especially when there was inflammation of the eyelid margins. 12 In our study, we obtained similar mydriasis, either with vaporization onto closed eyes or eye drop instillation in open eyes. Therefore, medications topically sprayed in closed eyes can affect intraocular sites, in addition to what was observed with the ocular surface tear film.
In 2010, Craig et al. studied the effect of a liposomal spray in an eye closed versus saline spray in the contra lateral eye for the treatment of evaporative dry eye. Improvement was clinically and statistically significant in the height of the meniscus tear, in the thickness of the lipid layer, and in the stability of the tear film in the eyes sprayed with liposomes. 13 In our study, we have evaluated the effectiveness of mydriatics in an aqueous vehicle, but using the application technique with the eye closed. Our results show that the effect of spray in eyes closed may also be effective in the aqueous vehicle without the use of liposome.
Footnotes
Author Disclosure Statement
The authors state that no competing financial interest exists.