
Abstract
Abstract
Objective:
To evaluate the efficacy of cyclosporine 0.05% (CsA) eye drops in patients with Stevens Johnson syndrome (SJS) who had chronic dry eye.
Design:
Prospective noncomparative interventional case series.
Methods:
Thirty cases of SJS patients who developed dry eye defined by symptoms and signs, including the Schirmer I test, the fluorescein clearance test (FCT), and corneal staining (fluorescein and Rose Bengal staining) were treated with CsA 0.05% eye drops twice daily for 6 months. Dry eye symptoms, eye injection, tear break up time (TBUT), and corneal staining were evaluated before and after the treatment at 0, 2, 4, and 6 months. The Shirmer I test and FCT were evaluated at 0 and 6 months.
Results:
Seventeen patients (56.67%) completed the study. Eight patients (26.67%) withdrew from the study as a result of intolerable side effects of CsA, which included pain, redness, and eyelid swelling. Five cases were lost in follow up. All 17 cases demonstrated significant improvement in dry eye symptoms, conjunctival injection, corneal staining, Schirmer I test, and FCT (P<0.05).
Conclusions:
CsA 0.05% eye drops might be beneficial in the treatment of chronic dry eye associated with SJS.
Introduction
The management of dry eye in SJS is very challenging. Several managements have been reported to alleviate the dry eye associated with SJS, including topical lubricants, autologous serum eye drops, 11 topical corticosteroids, punctal occlusion, tarsorrhaphy, amniotic membrane transplantation,12,13 as well as systemic immunosuppressive agents. Unfortunately, in severe cases, the efficacy of the treatment is still limited and long-term prognosis is often guarded. 14
Cyclosporine A (CsA) is a cyclic polypeptide produced by the fungus Tolypocladium inflatum. It works as an immunomodulatory agent mainly by inhibiting the activated T cells and downregulating inflammatory cytokines.Topical CsA has been reported to reduce the underlying inflammatory process in dry eye and increase goblet cell density. The efficacy and safety of topical CsA for the treatment of dry eye patients with and without Sjogren's syndrome or other autoimmune diseases, such as Graft versus host disease, were previously described.15–26 However, no study regarding topical CsA and dry eye in SJS has been reported.
The purpose of this study is to evaluate the efficacy of CsA 0.05% eye drops in the treatment of chronic dry eye in patients with SJS.
Methods
Study design
This study is conducted as a prospective noncomparative interventional case series to evaluate the efficacy of CsA eye drops in SJS patients who had chronic dry eye. The study was conducted in accordance with the principles of the Declaration of Helsinki, and was approved by the Committee for the Protection of Human Participants in Research at the Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand [SiEC number 336/2549]. After completing the informed consent, patients with SJS who met the inclusion criteria were enrolled for the study at the Department of Ophthalmology, Faculty of Medicine, Siriraj Hospital.The trial was registered with ClinicalTrials.gov, identification number NCT 01488396.
Patients
Patients were enrolled in the study after they satisfied all the following 4 criteriat:1) patients age of at least 18 years, 2) diagnosed with SJS for more than 3 months, 3) dry eye as confirmed by at least one of the following symptoms; dry sensation, foreign body sensation, photophobia, eye pain, and burning, which required chronic usage of ocular lubricants before the study, and 4) abnormal score for one of the aqueous tear tests (Schirmer I without anesthesia ≤5 mm/5 min or fluorescein clearance test (FCT) <3 mm/1 min) combined with abnormal corneal or conjunctival dye staining. Exclusion criteria included: use of oral or topical CsA or anticholinergic drugs, immunocompromised status, pregnancy, evidences of herpetic keratitis or other corneal infection and known allergic reaction to CsA or any components of CsA emulsion (glycerin, castor oil, polysorbate 80, and carbomer 1342).
Study procedures
At the first visit, the following parameters were assessed: history of dry eye symptoms (dry sensation, foreign body sensation, photophobia, pain, burning), examination of eyelids (ectropion, entropion), meibomian glands, eye lashes, lacrimal punctum, conjunctiva (injection, keratinization, and symblepharon), cornea, fluorescien tear break-up time (FBUT), fluorescein and Rose Bengal staining, the Schirmer I test (without anesthesia) and FCT. In addition, daily artificial tear usage was also recorded.
The patients were instructed to use commercially available preparation of cyclosporine 0.05% eye drops (Restasis®; Allergan) twice daily for 6 months and were allowed to continue their preservative-free artificial tear as needed. All parameters were re-evaluated at the 2-, 4-, and 6-month visit, except Schirmer I and FCT, which were repeated at the 6-month visit only.
Outcome measures
The severity of dry eye symptoms was graded using the visual analogue scale scoring from 0 to 10. Objective signs monitored were biomicroscopic examination of eyelids, meibomian glands, conjunctiva, cornea, FBUT, corneal dye staining, and tear volume tests (Schirmer I, FCT). Eyelid abnormalities, such as entropion, ectropion, and trichiasis were recorded. All lacrimal punctum configurations were indicated as opened, slit, or closed.
In each eye, the presence of symblepharon was recorded. Conjunctival keratinization was monitored in 4 quadrants area of the conjunctiva. Injection was graded as follows: 0=none; 1=mild hyperemia; 2=moderate hyperemia; or 3=severe hyperemia.
FBUT was assessed by the first disruption of dye on the cornea and the average value of 3 measurements was calculated. Corneal fluorescein staining was graded using the National Eye Institute system. 27 In brief, each of the 5 areas of the cornea and conjunctiva were scored from 0 to 3. The sum of the staining score then ranged from 0 to 15. For Rose Bengal staining, the Von Bijsterveld grading system was used for the conjunctiva and cornea. The staining was graded from 0 to 3 in each zone with the maximal score of 9.
The Schirmer I test without anesthesia (at 5 min) and the first strip of FCT (at 1 min) were used to measure tear volume once per each data point. Delayed tear clearance was assessed by the presence or absence of dye in the second strip of FCT (at 20 min).
Statistical Methods
To evaluate the significance of difference from baseline at 2-, 4-, and 6-month visits, the Wilcoxon signed rank test was used for continuous outcome measurements, including dry eye symptoms, visual acuity, conjunctiva (injection, staining, symblepharon, and keratinization), cornea (keratinization and dye staining), and tear volume by Schirmer I and the first strip of FCT. The McNemar test (or marginal homogeneity test) was used for categorical outcome measurements, including punctal status, lid abnormalities, and the tear clearance test. To compare differences at baseline between the group who completed the study and the group who withdrew from the study due to the adverse effects, the Mann–Whitney U test was used for continuous outcome measurements, and the chi-square test (or Fisher's exact test) was used for categorical outcome measurements. In all analyses, SPSS for Windows version 11.0 (SPSS Inc., Cary, NC) was used for statistical calculations, and a P-value of less than 0.05 was considered statistically significant.
Results
Patients' demographic data
Thirty patients (59 eyes) were enrolled into the study. Twenty of them (66.7%) were females and 10 (33.3%) were males. The mean age was 48 ranging from 23 to 81 years old. Seventeen patients (33 eyes) completed the study. Ten of them (58.8%) were females and 7 of them (41.2%) were males. Seven (23.3%) discontinued due to side effects of the medication. Five patients (16.7%) lost follow-up before 6 months, while one (3.3%) withdrew from the study after ocular surgeries.
Treatment response
In patients who completed the study, dry eye symptoms significantly improved as shown in Fig. 1. The mean scores of subjective symptoms, including foreign body sensation, photophobia, pain, and dry sensation at each follow-up visit were significantly decreased when compared with baseline measurements (P<0.05). The frequency of artificial tear requirement significantly decreased from 21.8 to 14.6 times per day (P=0.003) at 4 months and 14.8 times per day (P=0.011) at the 6-month visit (Fig. 2).

Comparison of dry eye symptoms, including dryness, foreign body sensation, photophobia, eye pain, and burning from baseline to month 6. Statistically significant improvements from baseline were noted at 2, 4, and 6 months [*P<0.005].
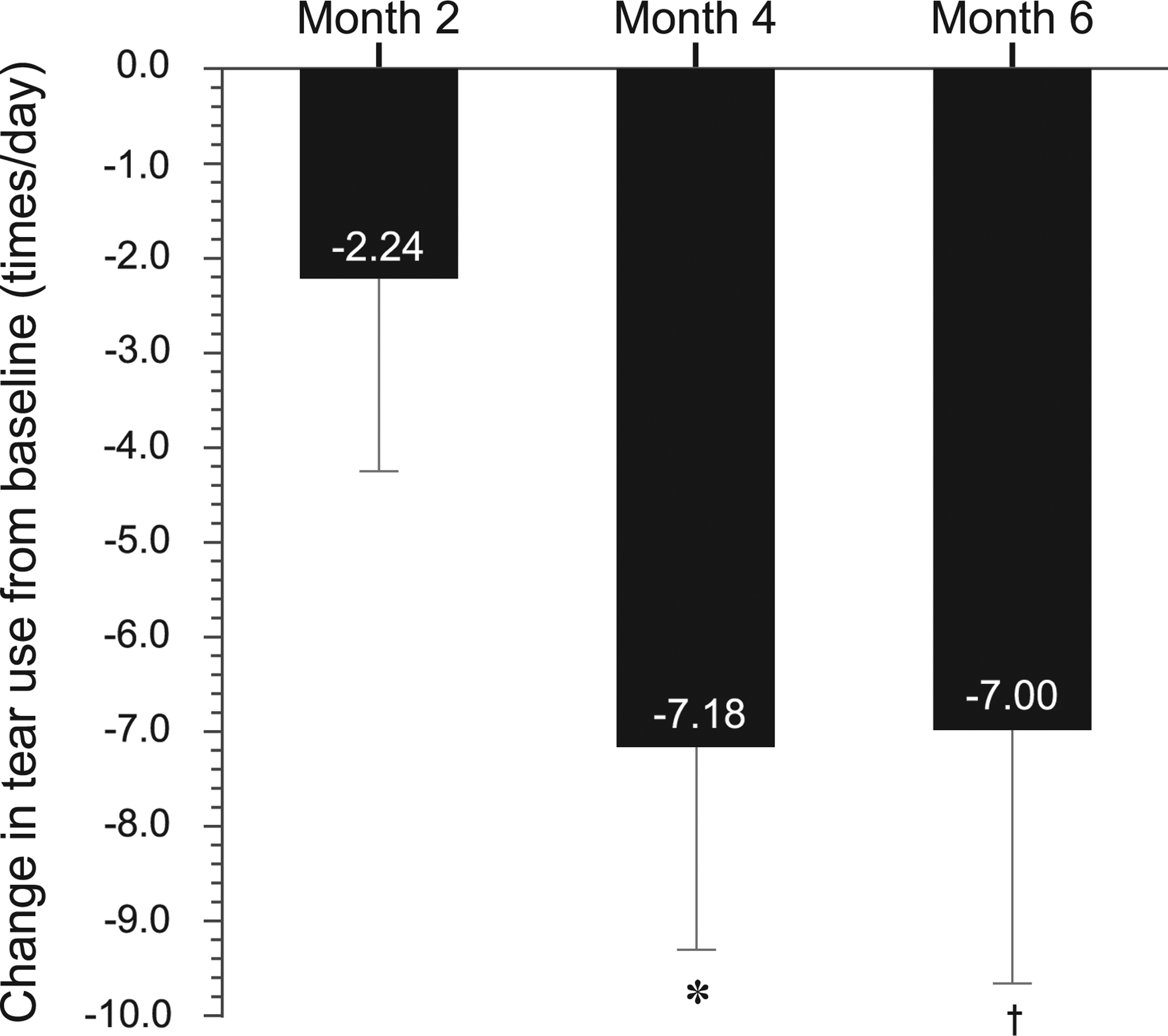
Comparison of artificial tear use (times per day) between baseline and month 6. Statistically significant reduction of artificial tear use was noted at 4 and 6 months [*P=0.003; †P=0.011].
Signs, such as conjunctival injection, also decreased significantly at each follow-up visit (P=0.006, 0.001, and <0.001 at 2, 4, and 6 months, respectively) (Fig. 3). Symblepharon and conjunctival keratinization did not change along the study.

Comparison of fluorescein staining, rose Bengal staining, conjunctival injection, and fluorescein tear break-up time (FBUT) from baseline to month 6. Statistically significant improvements from baseline were noted at 2, 4, and 6 months [*P<0.0.5] in all parameters except FBUT.
The mean fluorescein staining score was 13.0 at baseline. The mean score decreased to 10.4 (P=0.001), 8.9 (P<0.001), and 7.9 (P<0.001) at 2, 4, and 6 months, respectively. The same result was observed for Rose Bengal staining with the mean score of 7.9 at baseline and 6.2 (P<0.001), 5.5 (P<0.001), and 5.1(P<0.001) at 2, 4, and 6 months, respectively (Fig. 3). The FBUT values showed improvement at the 4- and 6-month visit with no statistical significance (P=0.344 and 0.152, respectively).
Tear volume assessed by Schirmer I and FCT significantly increased at 6 months (P<0.001) (Fig. 4). Clinical inflammation subsided after topical CsA as shown in Figure 5.
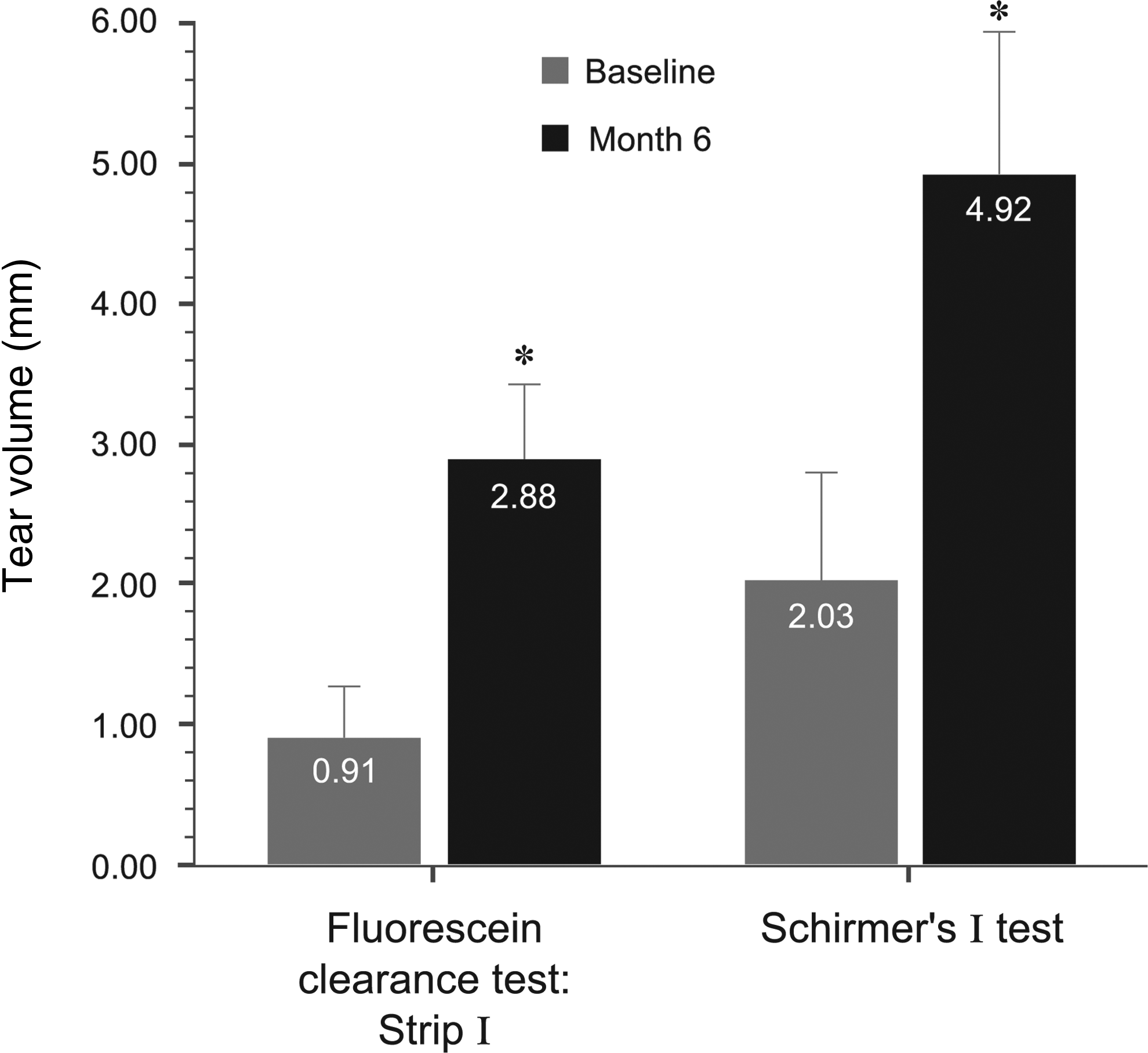
Statistically significant improvements in fluorescein clearance test and Schirmer I comparing baseline and 6 months [*P<0.05].

Pretreatment slit-lamp photograph
Adverse events
During the first 3 months, treatment-related adverse events occurred in 23.3% of total patients (7/30) leading to discontinuation of CsA. All 7 cases complained of eye pain, 13.3% (4/30) had eye injection, 6.7% (2/30) had lid swelling, and 3.3% (1/30) reported increase of dryness. Comparison between patients who completed the study and those who withdrew from the study due to the side effect using univariate analysis, revealed that, the withdrawal group exhibited more eyelid abnormalities (including entropion, trichiasis, total punctal occlusion) and lower tear volume (Schirmer I) as shown in Table 1.
Compares mean value between group by Mann–Whitney U test.
Compares mean value between group by chi-square test.
Compares mean value between group by Fisher's exact test.
FCT, fluorescein clearance test.
Discussion
This study demonstrates the efficacy of topical CsA 0.05% in the treatment of chronic dry eye in SJS. The results reveal that adjunctive treatment with CsA eye drop for 6 months can significantly improve dry eye symptoms (foreign body sensation, photophobia, eye pain, and dry sensation), decrease conjunctival injection and corneal dye staining, and increase tear volume in patients with SJS.
Topical CsA has been previously reported in several studies as a safe and effective treatment of dry eye in Sjogren syndrome18,19 and other autoimmune diseases.24,26 It inhibits T-cell activation28,29 and downregulates inflammatory cytokines, such as IL-6 and MMP-9, 24 in the ocular surface. The improvement of dry eye symptoms, corneal staining, and tear volume are probably based on the immunomodulatory properties of the drug that reduce the inflammation of the conjunctiva and lacrimal glands and increase goblet cell density.24,29,30
The Stevens Johnson syndrome is an autoimmune disease with chronic inflammatory reaction affecting several parts of the body, including the eye. Several patients suffer from the consequences of chronic ocular surface inflammation, loss of goblet cells, and decrease tear secretion,10,31 even after the acute stage of the disease. Chronic dry eye in SJS results from several factors, including lacrimal obstructive mechanism, goblet cell destruction, meibomian gland changes, and chronic inflammation. Reports also demonstrate chronic recurrent or persistent inflammation in the chronic stage of this disease.8,9 The improvement of dry eye in patients with SJS after topical CsA treatment in this study may emphasize the role of chronic inflammation as the main pathogenesis of dry eye in SJS. To the best of our knowledge, this study is the first to demonstrate the efficacy of topical CsA 0.05% in the treatment of chronic dry eye in the patients with SJS.
Although dry eye symptoms, conjunctival injection, dye staining, and tear volume significantly improved after CsA treatment, TBUT increased without statistical significance. This may be explained by the multiple factors influencing the stability of the tear film and the TBUT result, such as surface keratinization, goblet cell density, and mechanical irritation from eyelid abnormalities (trichiasis and entropion).
Photophobia showed less improvement than other symptoms. This might explain that photophobia is of ciliary spasm induced by several factors affected the ocular surface, cornea and anterior chamber. As a result, these symptoms might not be improved by topical CsA only.
Despite the improvement in symptoms, signs and tear tests as mentioned, 23% of the patients treated with topical CsA were unable to tolerate the side effects especially eye pain, leading to discontinuation of the treatment within the first 3 months. Similar finding has been reported by Barber and colleagues 32 with 20% treatment failure due to the side effect of topical CsA. Multivariate analysis indicated that this group of patients exhibited a higher occurrence of eyelid abnormalities, including trichiasis, entropion, and total punctal occlusion than those who completed the study. The eyelid abnormalities might cause chronic mechanical irritation and more inflammation of the ocular surface in these patients.
The authors are aware of the study limitations, including the noncomparative study design and the small sample size, and that the study results should be interpreted with care. Since SJS is a relatively rare disease, a prospective randomized controlled study is very difficult to conduct. Another limitation of the study is the inconsistency of the treatment results. The possible explanation might be the multiple pathogenesis of ocular involvement in chronic SJS, such as eyelid abnormalities, chronic inflammation, tear duct obliteration, and loss of goblet cells. These factors may vary with each case and, thus, determine the treatment modality, responses, and the outcome of each patient.
In conclusion, the present study suggests that CsA 0.05% eye drops could be considered an effective adjunctive treatment of chronic dry eye in patients with SJS. However, a prospective randomized controlled study on a larger population would be more conclusive.
Footnotes
Author Disclosure Statement
No financial interest exists.