
Abstract
Abstract
Purpose:
To evaluate the efficacy and complications of bevacizumab versus 5-fluorouracil (5-FU)-augmented bleb needling of failed filtration blebs following trabeculectomy.
Methods:
Twenty-seven eyes of 27 patients with bleb failure were included. Patients were randomly assigned to receive either 5-FU or bevacizumab. Needling was performed in the operating room under sterile conditions. After the needling procedure, a viscoelastic material was injected subconjunctivally around the bleb area to avoid the entrance of 5-FU or bevacizumab into the anterior chamber. Bevacizumab (1.25 mg/0.1 mL) was injected into 12 eyes and 5-FU injected into 15 eyes subconjunctivally. All of the patients were controlled weekly until a filtration bleb was maintained. Intraocular pressure (IOP), bleb appearance, and complications were noted in each group. Success was defined as absolute if the IOP 21 mmHg or less without any medication or surgical intervention at last visit, and qualified if the IOP 21 mmHg or less with topical antiglaucomatous medications. The patients were followed from 11 to 26 (median, 17) months.
Results:
The IOP decreased, from 31.2±3.2 mmHg to 16.1±2.1 mmHg, in the bevacizumab group on the first postoperative day. The IOP was within normal limits in 1 (8.3%) patient without medication and controlled with topical antiglaucomatous drops in 2 (16.7%) patients. The total success rate was 25% at the time of the last visit. Success was not achieved in 9 (75%) eyes. The IOP was 32.0±4.6 mmHg preoperatively and 12.2±2.6 mmHg on the first postoperative day in the 5-FU injected patients. The total success rate was 80%; 8 (53.3%) eyes showed absolute success, whereas 4 (26.7%) eyes showed a qualified success. A statistically significant difference between groups in terms of success rates was observed (P=0.04).
Conclusions:
Subconjunctival 5-FU application is a more effective therapy than bevacizumab application for needling procedures in failed trabeculectomy blebs.
Introduction
Needle revision with or without antifibrotic agents is an effective and simple method of restoring bleb function. 5-fluorouracil (5-FU) inhibits fibroblast proliferation, modulates the wound-healing process, and increases the success rate of glaucoma filtration surgery.4,5 Subconjunctival 5-FU application has been used in the early postoperative period alone, or with needle revision in bleb failure following trabeculectomy.5,8 Adjuvant subconjunctival mitomycin-C (MMC) application during bleb needle revision has also been reported.7,9 Although MMC and 5-FU help to prevent scar formation in the bleb area, they may cause widespread nonselective cell death and apoptosis. 10 Therefore, the use of these agents is associated with sight-threatening complications such as hypotony, blebitis, endophthalmitis, and wound leakage.
Bevacizumab is a full-length humanized monoclonal antibody directed against all isoforms of vascular endotelial growth factor-A. It is extensively used for metastatic colorectal cancer. Wound dehiscence at the colorectal anastomosis has been reported several months to years after original surgery in patients with metastatic colorectal cancer treated with intravenous bevacizumab.11,12 Based on this situation, it has been proposed that bevacizumab may inhibit the wound-healing process in a long-term period. Recent studies showed that subconjunctival injections of bevacizamub could reduce scarring in animal models of glaucoma. 13
The key players in generating scar tissue after trabeculectomy are the fibroblasts in the Tenon's capsule. It has been demonstrated that bevacizumab affects both vascular and fibroblast proliferation directly in glaucoma filtration surgery. In addition, it modulates the inflow of proinflammatory cytokines into the bleb from surrounding vessels. 14 For this reason, anti-VEGF agents may also exhibit beneficial effects during glaucoma surgery. The use of subconjunctival injections of bevacizumab to salvage failing blebs has been described in a small number of case reports.15,16 To our knowledge, no reported study has compared 5-FU and bevacizumab for the needle revision of failed filtration blebs. The purpose of this study was to compare the efficacy and complications of needle revision and subconjunctival 5-FU-versus-bevacizumab application in bleb failure after trabeculectomy.
Methods
This is a prospective and comparative case series of patients who underwent needle revision augmented with bevacizumab or 5-FU for failed trabeculectomy blebs between November 2008 and February 2011. Twenty-seven eyes of 27 patients with bleb failure were included. All of the eyes had failing filtering procedures with or without the use of antifibrotic agents, and an intraocular pressure (IOP) >21 mmHg. Signs of a failed bleb included an unacceptably high IOP, an open corneoscleral window at gonioscopy, vascularization, thickening and flattening of the bleb, and loss of the conjunctival microcysts. Patients were randomly assigned to receive either 5-FU or bevacizumab.
Demographic properties of the patients, previous surgeries, the type of glaucoma, antimetabolite use in last trabeculectomy, the time interval between the last trabeculectomy, and the needling procedure were noted. Visual acuity testing, IOP measurements, anterior segment, and fundus examinations were then performed.
A single surgeon (T.S.) performed all of the bleb revisions using a standard protocol. The procedure was performed in the operating room under sterile conditions. A sterile cotton swab soaked with proparacaine was placed over the superotemporal quadrant for approximately 5 min. Brimonidine eye drops were used preoperatively to prevent bleeding from the conjunctival vessel during the procedure. With the eye infraducted, the subconjunctival space was entered at least 5 mm from the site of the filtration bleb using a 29-gauge needle. Multiple passes and back and forth sweeping movements were performed to disrupt any episcleral fibrosis. Careful attention was given to avoid inadvertent perforation of the overlying conjunctiva and subconjunctival blood vessels. Then, the needle was moved into the bleb cavity, underneath the scleral flap, until the fistula between the anterior chamber and subconjunctival space was reformed. A viscoelastic material was injected subconjunctivally around the bleb area to avoid the entrance of 5-FU or bevacizumab into the anterior chamber before exiting the wound. The entry site was closed with a single 8-0 Vicryl suture when necessary. At the end of the procedure, a single subconjunctival injection of 5-FU at a dose of 5 mg/0.2 mL or bevacizumab at a dose of 1.25 mg/0.1 mL were administered outside the viscoelastic material. Patients were examined daily for the first week, and weekly for the first month or as necessary, depending on the IOP and the appearance of the filtration bleb. Topical prednisolone acetate (1%) was administered every 2 h while awake for the first month. The dose was then tapered according to the clinical signs of conjunctival inflammation and bleb function. Topical ofloxacin (2%) eye drops were administered 5 times per day for 1 week. The patients were followed for 11–26 (median, 17) months. In control examinations, the IOP, bleb appearance, and complications were noted. Absolute success was defined as an IOP 21 mmHg or less without antiglaucomatous medications measured at the last visit. A qualified success was defined as an IOP 21 mmHg or less with topical antiglaucomatous medications.
The study followed the tenets of the declaration of Helsinki. Written informed consent was provided by each patient after an explanation of the nature and possible consequences of the study. The protocol was approved by the Institutional Ethics Committee.
Statistical analyses were performed using the SPSS software (ver. 15.0). The normality of data was evaluated using a Shapiro–Wilk test. Descriptive statistics were used to evaluate the demographic characteristics of the patients. Differences in success rates among the groups were compared using the chi-squared test. A statistically significant difference was defined as one with a P value < 0.05.
Results
Patients with failed filtration blebs were included (n=27). Table 1 shows the demographic and clinical characteristics of the patients. No statistically significant difference between demographic characteristics was observed (P>0.05). No diagnostic difference between the groups was evident. The baseline IOP was between 27 and 42 (mean, 32.0±4.6) mmHg in the 5-FU group and 26–35 (mean, 31.2±3.2) mmHg in the bevacizumab group. No statistical difference was observed between the groups (P=0.638). Needling and subconjunctival 5-FU or bevacizumab were applied between 4 and 12 (median, 5) weeks following trabeculectomy.
5-FU, 5-fluorouracil; F, female; M, male; IOP, intraocular pressure; min, minimum; max, maximum; PEX, pseudoexfoliative; POAG, primary open angle glaucoma.
The IOP was found to be 12–19 (mean, 15.8±1.9) mmHg following the procedure in the bevacizumab group. The mean IOP after the procedure was 12.4±2.3 (range, 8–18) mmHg in the 5-FU group. Through an analysis with an independent sample t-test, the difference between the preprocedure and after-procedure IOP was statistically significant in both groups (P=0.001). There was also a significant difference in terms of after-procedure IOP between groups (P=0.00). In 8 (53.3%) eyes, the IOP remained below 21 mmHg with no medication (complete success), while in 4 (26.7%) eyes, it was controlled with topical antiglaucomatous agents (qualified success) in the 5-FU group. Thus, the total success rate was 80%. In the remaining 3 (20%) eyes, the IOP was above 21 mmHg despite topical antiglaucomatous agents. In the bevacizumab group, the IOP was within normal limits in 1 (8.3%) eye with no medication, and controlled with topical antiglaucomatous drops in 2 (16.7%) eyes. The total success rate was 25% at the time of the last visit. Success was not achieved in 9 (75%) eyes. Figure 1 shows distribution of the success rate among groups. A statistically significant difference in terms of the success rates between the 2 groups was observed (P=0.007).
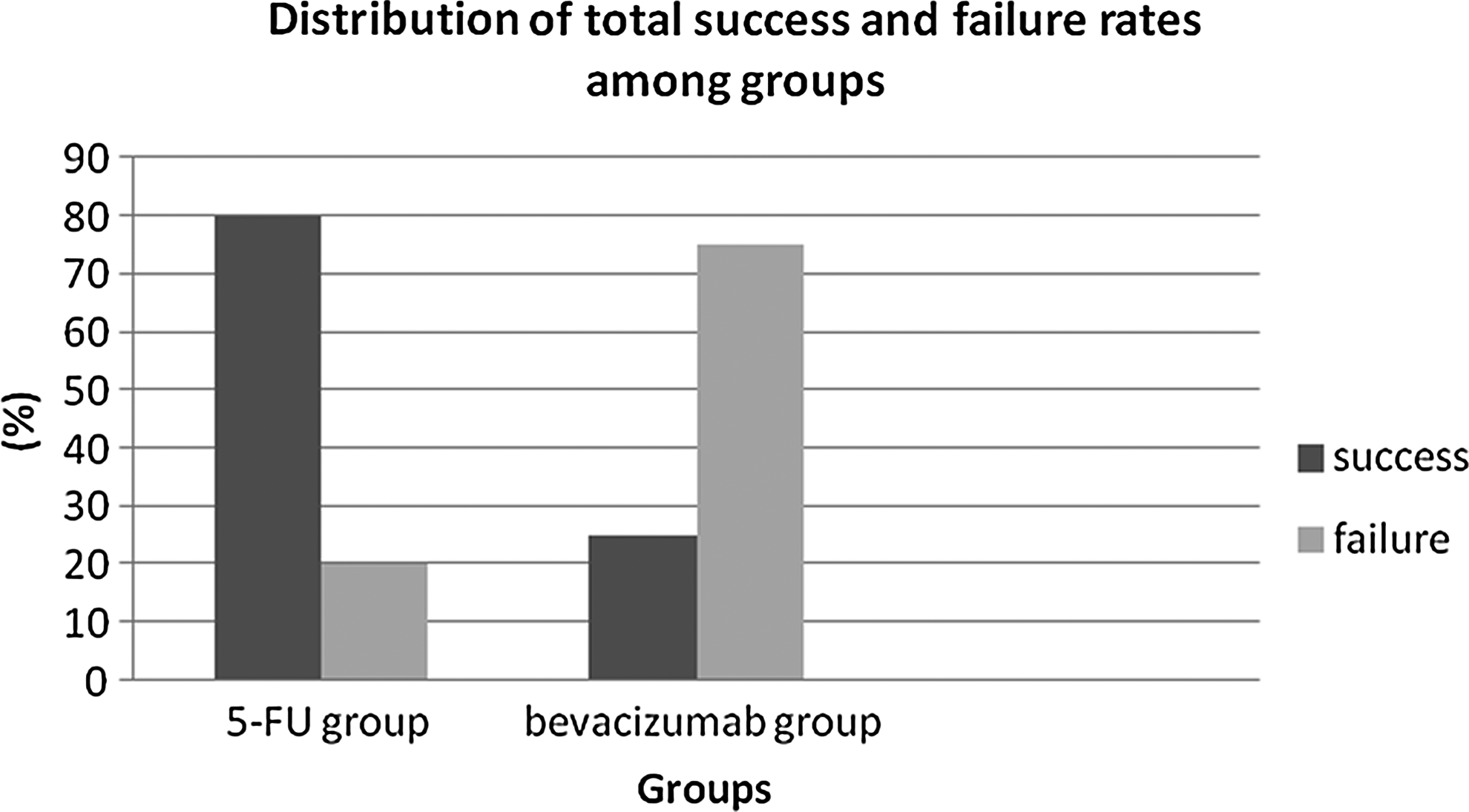
Distribution of success and failure rates among groups.
Transient complications were encountered in 14/27 (51.8%) eyes. The distribution of complications according to the groups is shown in Table 2. No statistically significant difference between the groups in terms of the occurrence of complications was observed (P>0.05). The anterior chamber reaction was thought to be due to the injection of bevacizumab, and corneal punctate epitheliopathy was thought to be due to the injection of 5-FU. Healon GV was injected into the eye with hypotony. The other complications were resolved without surgical intervention.
Discussion
The success rate of filtration surgery has been reported as 67%–94% in different studies, and bleb failure remains a common problem. 1 A functional bleb is characterized by a filtering fistula between the anterior chamber and the subconjunctival space. A steady flow of aqueous humor is required to maintain a passageway at the outer edge of the scleral fistula and to distend the interstitial space within the bleb.2,6 Bleb failure in the early postoperative period may be due to the obstruction of the internal filtering ostium by blood clots, uveal tissue, or the vitreous, or sutures in the scleral flap being too tight. 6 In the management of immediate bleb failure following trabeculectomy, numerous techniques have been described, including digital ocular compression, argon laser suture-lysis, releasable sutures, tissue plasminogen activator application to the anterior chamber, subconjunctival 5-FU application, and Nd-YAG laser fistula revision.2,6
Bleb failure in the late postoperative period may be due to the proliferation of the connective tissue cells in the episclera, which fill the interstitial space within the bleb, or bridging of the Tenon's capsule over the bleb. These conditions are predominantly observed due to an inadequate aqueous humor flow through the bleb. 6 The adjuvant intraoperative use of antifibrotic agents has been shown to increase the success of filtration surgery.3,5,17
Subconjuctival 5-FU application in the early and late postoperative period has been shown to increase the success rate of trabeculectomy.5,17–19 Despite the use of adjuvant intraoperative or postoperative antimetabolites, bleb failure is still common in high-risk glaucoma patients.1,2 Needle revision is an alternative technique in postoperative bleb failure cases. Needle revision has been reported to be effective in improving bleb function in bleb failure cases due to fibrosis at the episcleral level and within the bleb or encapsulation by the Tenon's capsule.4,7,8 In these studies, adjuvant subconjunctival 5-FU application increases the success of the needle revision technique. The success rate of needle revision in bleb failure has been reported as 17%–91.6% in different studies.7–9,20,21
Adjuvant subconjunctival 5-FU or MMC application during bleb needle revision has been used in several studies.7–9,20,21 MMC has advantages over 5-FU, including higher potency, a lower risk of bleb encapsulation, and improved control of IOP after trabeculectomy. 7 However, MMC displays several dangerous complications, including thin avascular leaking blebs, hypotony, and blebitis. 9 Application of MMC at a lower concentration may reduce the occurrence of hypotony and other complications.
It has been shown that hydrocortisone-21-phosphate and AGM-1470 are angiogenesis inhibitors that display significant effects on Tenon's fibroblast proliferation and migration. Researchers have thus suggested that angiogenesis inhibitors may be used for wound modulation in glaucoma filtration surgery.22,23 The use of subconjunctival bevacizumab for bleb failure following trabeculectomy has been reported. 16 The wound-healing process is carried out with both fibroblastic activity and angiogenesis. 22 For this reason, anti-VEGF agents would be expected to decrease the new vascular growth and inhibit the fibroblastic activity. However, the antifibrotic effects of bevacizumab have not been experimentally demonstrated. Yoeruek et al. found that bevacizumab did not display toxic effects on human corneal fibroblast cells even at high concentrations. 24 Unpublished data have shown that the inhibition of the neovascular cascade by anti-VEGF agents decreases fibroblast proliferation through cytokines, including fibroblast growth factors.
We found that 5-FU was more effective than bevacizumab for this procedure. The total success rates were 25% in the bevacizumab group and 80% in the 5-FU group. The differences in the success rates may be due to the different antifibroblastic activity of the adjuvant agents. Grewal et al., in a pilot study with a small number of subjects and 6 months follow-up, suggested that subconjunctival bevacizumab is a potential adjunctive treatment for reducing the incidence of bleb failure after trabeculectomy. 15 The limited sample size, short-term follow-up, and the lack of a control group were the limitations of this study. These prevent us from making firm conclusions regarding the efficacy of bevacizumab injections in reducing bleb failure.
Memarzadeh et al. studied the usefulness of the subconjunctival injection of bevacizumab on bleb morphology in rabbits. 13 They found that bevacizumab created a more favorable bleb morphology compared with 5-FU and control groups. However, unlike our study, bevacizumab was injected after trabeculectomy in this study. Therefore, the early injection of bevacizumab after trabeculectomy would be more effective for bleb survival than postneedling injection. Kahook et al. reported a case in which a significant decrease in IOP was observed after needling and subconjunctival injection of bevacizumab. In this case, the IOP decrease was transient. 16 For this reason, it may be that the IOP reduction resulted from bevacizumab injection or solely from the effects of the needling procedure. It is obviously difficult to answer this question with 1 case report; further controlled clinical and experimental studies are required to understand the effectiveness of anti-VEGF agents in glaucoma surgery and needling procedures. In the present study, bevacizumab injection was performed at different stages of the wound-healing response in each patient. This may be a reason of the failure of needling and bevacizumab injection. If needling and bevacizumab injection were performed on the new vessel formation stage of the wound-healing response, the success rate would be expected to increase. In addition, repeat injection of the bevacizumab would be more effective than a single injection in reducing angiogenesis and fibrosis. Li et al. demonstrated that 1 injection of a high dosage of bevacizumab (25 mg/mL) during the surgery reduced the angiogenesis and fibrosis in a rabbit model of glaucoma filtration surgery. They stated that bevacizumab was only effective in increasing the bleb area and did not affect the IOP. 25
The wound-healing response is a complex process; consequently, more than 1 agent may be needed to inhibit scar formation in the bleb area. Recently, How et al. found that bevacizumab in combination with 5-FU offers greater antifibrotic effect over monotherapy in a rabbit model of glaucoma filtration surgery. 26 They concluded that bevacizumab and 5-FU have synergistic effect in reducing the fibroblastic activity of the wound-healing process. Combined treatment with 5-FU and bevacizumab may also be effective in the treatment of failed filtration blebs. This treatment modality might be advantageous to lessen corneal complications of 5-FU. Kahook reported that the combination of intravitreal ranibizumab and MMC at the time of trabeculectomy resulted in more diffuse blebs with less vascularity compared to the use of MMC alone. 27
Several complications such as wound leak, choroidal effusion, a shallow anterior chamber, bleb-related endophthalmitis, hypotony maculopathy, suprachoroidal hemorrhage, corneal epitheliopathy, and subconjunctival hemorrhage have been reported to be associated with needle revision and subconjunctival 5-FU application.2,6,28,29 In this study, no significant difference was observed between the groups in terms of complications. However, the anterior chamber reaction was thought to be due to the injection of bevacizumab, and the corneal punctuate epitheliopathy due to 5-FU injection. The intravitreal injection of bevacizumab may cause IOP spikes, particularly in suspected or confirmed cases of glaucoma. Kahook and coworkers 30 found that bevacizumab displayed a toxic effect on trabecular meshwork cells. Other reports have stated that bevacizumab may physically accumulate in the trabecular meshwork and block aqueous outflow, leading to an increased IOP. It is not yet known whether IOP elevation occurs after the subconjunctival injection of bevacizumab.
In conclusion, needle revision and subconjunctival 5-FU application was a more effective procedure than needling and subconjunctival bevacizumab injection for bleb failure following trabeculectomy. Further controlled clinical studies are required to determine the time and route of administration of bevacizumab in the glaucoma surgical procedure.
Footnotes
Author Disclosure Statement
None of the authors have a conflict of interest with the submission.