
Abstract
Abstract
Purpose:
Dexamethasone palmitate (DXP) is a lipophilic prodrug of dexamethasone (DXM), a potent corticosteroid used to treat a variety of ophthalmic diseases. The aim of the study was to characterize the sustained release capacity (in rabbit), efficacy (in rat and rabbit), and safety (in rabbit, cat, and minipig) of intravitreal (IVT) DXP emulsions in preclinical models.
Methods:
Oil-in-water emulsions of DXP were administered by IVT injections in rats, rabbits, cats, or minipigs. Efficacy was assessed in rabbits by the inhibition of VEGF-induced vascular leakage and in rats by inhibition of laser-induced choroidal neovascularization. Concentrations of DXP and DXM in aqueous humor, vitreous, retina, choroid, and blood were determined to characterize the ocular and systemic pharmacokinetic (PK) profile. Complete ophthalmic examinations (indirect ophthalmoscopy, slit-lamp biomacroscopy, electroretinography, tonometry) were performed to assess the ocular safety of IVT DXP doses up to 2,600 μg in minipig, followed by histopathologic examinations. A validated feline model of DXM-induced elevated intraocular pressure (IOP) was used to assess the ocular hypertensive impact (i.e., the safety) of an IVT injection of DXP emulsion.
Results:
Rat and rabbit efficacy data demonstrated that IVT injections of DXP emulsions were effective. Rabbit PK data demonstrated that following a single 1,280 μg IVT injection resulted in sustained DXM levels in the retina and choroid (1,179.6 and 577.7 ng/g with a half-life of 189 and 103 days, respectively) sufficient to inhibit VEGF-induced vascular hyper-permeability for up to 9 months. No adverse ocular findings were observed in the rabbit at the 1,280 μg DXP dose. Plasma levels of DXP and DXM were close to the lower limit of quantification (0.5 ng/mL). In minipigs, no systemic effects were observed at a dose up to 2,600 μg DXP. In steroid responsive cats, IVT DXP emulsions increased IOP to a lesser extent than triamcinolone acetonide with a more rapid return to basal levels and no evidence of cataract formation.
Conclusions:
IVT injections of DXP emulsions were well tolerated and shown to be efficacious for the sustained release of the drug, with the potential to control vascular leakage up to 9 months following a single IVT injection. These data suggest that IVT injections of DXP emulsions could be a safe and effective alternative IVT drug delivery vehicle for corticosteroid to treat back of the eye diseases complicated by macular edema.
Introduction
Although anti-VEGF therapies are effective for the treatment of macular edema, the burden of repeated intravitreal (IVT) injections on ophthalmologist and patients is a major disadvantage to this class of agents. Prior to the recent advances in the development of anti-VEGF therapies there has been an interest in the IVT use of corticosteroids such as dexamethasone (DXM), triamcinolone acetonide (TA), and fluocinolone acetonide (FA) for the treatment of retinal and choroidal diseases complicated by macular edema. While corticosteroids administered either by periocular or IVT injections or by the implantation of surgical devices have shown efficacy in improving visual acuity and anatomically reducing macular edema, the beneficial effect of corticosteroids is invariably offset by an increase in intraocular pressure (IOP) and/or cataract development, well-established corticosteroid side effects.2–6
In an attempt to improve the efficacy and safety of intravitreally administered corticosteroids for the treatment of macular edema, a new strategy was conceived in which dexamethasone palmitate (DXP) was formulated in an oil-in-water emulsion that possesses the capacity to deliver in a sustained manner therapeutic doses of DXM to the retina and choroid. DXP is an ester prodrug of DXM that greatly increases the lipophilicity of DXM, thus allowing for its formulation in the oily core of an oil-in-water emulsion. Unlike other intravitreally administered corticosteroids, DXP is inactive in the vitreous cavity because (1) DXP is entrapped in the oil droplets that are dispersed in the vitreous following the injection of the emulsion, (2) DXP is practically insoluble in aqueous media (i.e., there is no free DXP in the vitreous humor), and (3) the palmitate tail of ester prodrug inactivates DXM (DXP has a 47-fold lower affinity for the glucocorticoid receptor than DXM). Thus, DXP is expected to have a limited effect on the lens and the anterior chamber angle structures. It is only following the hydrolysis of DXP by tissue esterases in the retina and choroid that free DXM is elaborated to exert its anti-angiogenic and anti-inflammatory actions locally in these target tissues (Fig. 1). In the present report we present the results of preclinical studies evaluating the pharmacokinetics (PK), safety, and efficacy of DXP emulsions injected intravitreally via 30-gauge needles in animal eyes. The results of these experiments establish a proof of concept for the utilization of lipophilic prodrug oil-in-water emulsions as a potentially safer sustained IVT vehicle for DXM retinal delivery.
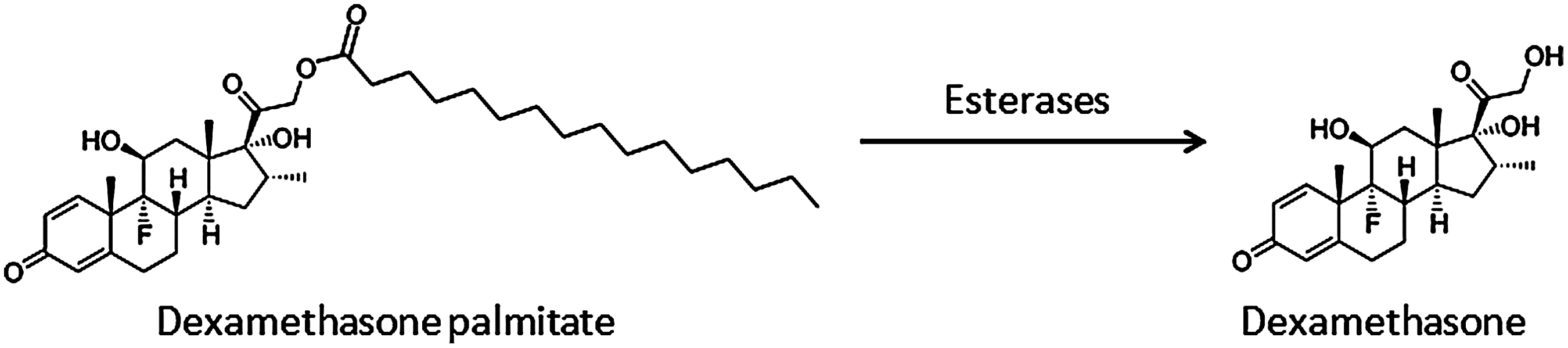
Enzymatic hydrolysis of dexamethasone palmitate (DXP) into dexamethasone (DXM).
Methods
Reagents
All solvents were of high-pressure liquid chromatography (HPLC) grade, while chemicals and reagents were of analytical grade and excipients conformed to USP standards. DXP was obtained from Symbiotica.
DXP emulsion
DXP emulsions at strengths ranging from 0.56% to 5.2% were used for this study. Briefly, DXP was solubilized in the oil phase at the desired concentration along with lipophilic nonionic surfactants. The oil phase was then mixed to the aqueous phase containing nonionic surfactants and osmotic agents to generate a stable oil-in-water emulsion. The final emulsion contains oil nanodroplets (∼200 nm) dispersed in an aqueous phase at pH 7.0 (Table 1).
Mean droplet size was determined by dynamic light scattering (HPPS; Malvern Instruments), and zeta potential by electrophoretic mobility measurement (Zetasizer 2000; Malvern Instruments).
Animals
All animals were treated according to the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research (ARVO Handbook, 1993). Brown Norway male rats (Charles River) were housed 4 per standard cages. Male and female adult rabbits (2–2.9 kg) from the Fauve de Bourgogne and HYRNZ104 strains (pigmented) and New Zealand White rabbits (albino) obtained from CEGAV) and Centre LAGO, respectively, were ear tagged upon arrival. Following a 7-day quarantine period and a thorough ocular examination the rabbits were randomly assigned to study groups. One-year-old, domestic, shorthair female cats were obtained from Cherry Hills Kennels. Three- to 4-month-old male and female Göttingen minipigs (Ellegaard) were used for the long-term safety evaluation.
Rabbits and cats were housed individually in standard cages, while minipigs were housed 2–3 per pen. All the animals had free access to food and water ad libitum and were kept under 12-h-light and 12-h-dark cycles throughout the study. On completion of the observation period, the animals were anesthetized and sacrificed by an overdose of pentobarbital.
In vivo experimental procedures
A summary of the PK, efficacy, and safety studies is presented in Table 2.
CNV, choroidal neovascularization; PK, pharmacokinetic; IOP, intraocular pressure.
Efficacy evaluation of DXP emulsion in the rat by angiography and inhibition of choroidal neovascularization
Twenty-four male Brown Norway rats were divided into 3 groups of 8 rats per group. On the first day of experiment (day 0), choroidal neovascularization (CNV) was induced with a 532-nm argon laser photocoagulator (Viridis; Quantel Medial) in the right eyes (eight 75 μm-sized spots at 150 mW for 100 ms) of the anesthetized animals. The rupture of Bruch's membrane was confirmed by the formation of a bubble. Following the laser procedure on day 0 supratemporal IVT injections of either the vehicle [phosphate-buffered saline (PBS); 2 μL), 0.8% DXP emulsion (4 μg DXP; 0.5 μL), and Kenacort® (80 μg TA; 2 μL) were administered to the treated right eyes. Fluorescein angiography was performed on days 7, 14, and 21 with a Heidelberg's Retinal Angiograph (Sanotek) to characterize the leakage intensity of the induced neovascularization, which was scored from 0 to 3 (score 0, no leakage; 1, slight leakage; 2, moderate leakage; 3, strong leakage). 10 The grading was based on the highest intensity of fluorescein in each lesion, and was not determined by the size of the leakage area. At the end of the experiment on day 23, right eyes were harvested and fixed 1 h in 4% paraformaldehyde, and the dissected flat-mounted choroid/sclera incubated with FITC-isolectine B4 antibody. Fluorescence-labeled preparations were viewed under an Operating Microscope OPMI® MDOxy (Carl Zeiss) equipped with Apotom at 488 nm, and the size of the CNV was measured by a morphometric analysis with Axiovis 4.8 image analysis software (Carl Zeiss). 7–9
PK of DXP emulsion in pigmented rabbit
PK studies with low and high DXP doses were conducted with DXP emulsions at different strengths (0.8% and 3.2% DXP) to assess the ocular tissue concentrations of DXP and DXM over time following a single IVT injection. Pigmented rabbits of the Fauve de Bourgogne strain were used for these studies. Plasma samples were analyzed by an HPLC-MS/MS method [lowest levels of quantification (LLOQ)=0.5 ng/mL], while ocular tissue samples were analyzed by rapid resolution liquid chromatography (RRLC)-MS/MS methods described in the assays section.
In the low-dose PK study, 24 male rabbits were divided into 3 treatment groups of 8 animals each and received single bilateral IVT injections of 12.5, 25, or 50 μL of 0.8% DXP emulsion, corresponding to 100, 200, and 400 μg of DXP, respectively. At 1 week and 1, 2, and 8 months, rabbits were anesthetized and whole blood was collected for DXP and DXM plasma concentrations. After euthanasia, the eyes were harvested, and aqueous humor (AH), iris/ciliary body (ICB), vitreous (V), and retina/choroid (RC) were collected to assess their DXP and DXM content.
In the high-dose PK study, with the 3.2% DXP emulsion, both male and female pigmented rabbits were used to characterize the ocular PK profile. Thirty rabbits were randomly divided into 5 subgroups of 6 animals (3 males + 3 females) corresponding to 5 time-points (1 week and 1, 2, 6, and 9 months). On day 1, 40 μL of the 3.2% DXP emulsion corresponding to 1,280 μg of DXP was administered by an IVT injection into the right eye of each rabbit while the left eye remained untreated, and served as control. At each time-point animals were sacrificed and aqueous humor (AH), vitreous (V), retina (R), and choroid (CH) from treated eyes were analyzed for both DXP and DXM concentrations.
Sustained efficacy evaluation of DXP emulsion in the rabbit by inhibition of VEGF-induced vascular permeability
For the 4-month efficacy study of the DXP emulsion, 24 pigmented rabbits were randomly divided into 4 groups of 6 animals each, and dosed (50 μL, once) with bilateral IVT injections of 0.56% (i.e., 280 μg DXP) or 1.12% (i.e., 560 μg DXP) DXP emulsions, Kenacort (4% TA, 2 mg), or PBS at the beginning of the study. Breakdown of the blood–retinal barrier was induced 120 days after the treatment by a single 50 μL IVT injection of 500 ng rhVEGF165 with carrier protein (diluted in PBS) in both eyes. Forty-eight hours after the induction, sodium fluorescein leakage was quantified with an FM-2 Fluorotron Master ocular photometer (OcuMetrics). The efficacy of the emulsion was determined as the percentage of fluorescein leakage reduction when compared to the control group. IOP was measured in parallel with a pneumotonometer Model 30 classic (Medtronic Solan).
In the 9-month efficacy study, VEGF-induced retinal permeability was assessed 4, 6, and 9 months after a single IVT injection. Six rabbits (3 males + 3 females) were injected on day 1 with 40 μL of the 3.2% (i.e., 1,280 μg DXP) DXP emulsion in the right eye, while the left eye remained untreated and served as control. At the aforementioned time-points, increased retinal vascular permeability was induced by a single 50 μL IVT injection of 500 ng of rhVEGF165 with carrier protein (diluted in PBS) into the right eye. Forty-eight hours after the induction, sodium fluorescein leakage was quantified with an FM-2 Fluorotron Master ocular photometer (OcuMetrics) in both the treated and VEGF-challenged right eye and the untreated and unchallenged control left eye. The efficacy of the emulsion was determined by comparing the extent of fluorescein leakage in the right and left eyes. A ratio (treated eye/untreated eye) of 1 indicated that VEGF-induced vascular permeability was normalized. 11
Toxicity evaluation of DXP emulsion in the rabbit (2-month ocular toxicity study)
For the short-term safety study 6 New Zealand White rabbits, 3 per group, received either a 40 μL IVT injection of 3.2% (i.e., 1,280 μg DXP) DXP emulsion or PBS in both eyes on day 1 and were observed over an 8-week period. Throughout the experiment, the animals were checked daily for mortality, clinical signs, and food consumption. Body weight was recorded during the pretreatment period, on day −1, on day 8, and then once weekly. Complete ophthalmic examinations, including biomicroscopy and indirect ophthalmoscopy, were performed during the pretreatment period, immediately after administration, on days 15 and 29, and during weeks 6 and 8.12,13 IOP was recorded pretest, on day 8, and then weekly. Plasma levels of DXP and DXM were determined in samples collected on day 15 and during weeks 4 and 8. On completion of the 8-week observation period, the animals were sacrificed and the eyes with optic nerves were preserved for subsequent histopathologic examination (using standard tissue preparation procedures and hematoxylin and eosin staining).
Evaluation of the ocular tolerance of DXP emulsion in a feline model of DXM-induced elevated IOP
Colonies of socialized cats were trained for measurement of IOP using a pneumotonometer. After establishing a baseline IOP, cats received topical 0.1% DXM 3 times daily and underwent daily IOP measurements. Cats that did not respond with a significant rise in IOP were selected out and eliminated from all studies. Following 10 days of topical DXM applications, treatment was suspended and IOP returned to normal levels in 2 to 3 days. This model has been used extensively for over a decade to evaluate ocular hypertensive potential of numerous anti-inflammatory compounds. 14 The present study was divided into 2 phases: (1) In phase I, 7 cats, demonstrating an elevated IOP response to topical DXM, were used to establish the IOP response to a 50 μL IVT injection of TA (Kenacort). The outcome of this study validated the use of the feline model for phase II. (2) In phase II, 18 topical DXM responsive cats were monitored over 120 days for an IOP response to (i) 50 μL IVT injection of TA (Kenacort), (ii) 20 μL IVT injection of 0.8% (i.e., 160 μg DXP), DXP emulsion, or (iii) 20 μL IVT injection of blank emulsion.
Long-term safety assessment in the minipig
Thirty eight (38) Göttingen minipigs were divided into 3 groups corresponding to control (PBS, 7 males + 7 females), low-dose DXP emulsion (5 males + 5 females), and high-dose DXP emulsion (7 males + 7 females). All animals received 50 μL bilateral IVT injections of PBS, 1.6% (i.e., 800 μg DXP per eye; low dose) DXP emulsion, or 5.2% (i.e., 2,600 μg DXP per eye; high dose) DXP emulsion, respectively. Animal well-being, body weight, clinical signs, and food consumption were assessed regularly throughout the study in parallel to complete ophthalmic examinations (biomicroscopy, indirect ophthalmoscopy, electroretinography, and IOP evaluation). Blood samples were collected for plasma DXP and DXM concentrations (by HPLC-MS/MS), hematology, and blood biochemistry evaluations. At 2 and 13 weeks post-IVT and on completion of the 39-week observation period, a full macroscopic postmortem examination on selected organs and histopathologic examination (using standard tissue preparation procedures and hematoxylin and eosin staining) of the eyes and optic nerve were performed in all animals. 15
Assay methods
HPLC-MS/MS and RRLC-MS/MS methods
A HPLC MS/MS was developed and validated for the simultaneous quantification of DXP and DXM in rabbit and minipig plasma. Briefly, plasma proteins were precipitated with acetonitrile and the supernatant (containing DXP, DXM, and the internal standard, i.e., beclomethasone) was analyzed by reversed phase (HPLC) with MS/MS detection (positive mode) after ionization using atmospheric pressure chemical ionization.
An RRLC-MS/MS method for the quantification of DXP and DXM in rabbit aqueous humor (AH), vitreous (V), retina (R), and choroid (CH) was developed.
All matrices were treated with ethylacetate and the respective supernatants (containing DXP, DXM, and the internal standards, that is, d3-DXP and d3-DXM) were analyzed by RRLC with MS/MS detection (positive mode) after ionization using an electrospray interface (ESI). The methods were validated according to the SFSTP 16 and FDA (U.S. Department of Health, 2001) guidelines.
The LLOQs in rabbit ocular tissues were set at 10 ng/mL (AH), 2.5 ng/mL (V), 10.7 ng/g (R), 6.8 ng/g (CH), and in minipig and rabbit plasma at 0.5 ng/mL for both DXP and DXM.
Data analysis and statistical methods
The tissue concentration data from the PK and toxicokinetics are presented as mean±standard deviation and expressed in ng/g or ng/mL. WinNonlin software (v. 5.0; Pharsight, Sunnyvale, CA) was used to calculate the half-life (T1/2) and Cmax, Tmax, and area under the curve (AUC) AUCs were calculated with Microsoft Excel® software. Statistical evaluation of significant differences between sample means by 2-tailed Student's t-test was made using Excel Microsoft software.7–9,11
Results
DXM ocular distribution following a single IVT administration of the prodrug DXP
Ocular tissue distribution of both the prodrug DXP and its metabolized product-free DXM was investigated following a single IVT injection of DXP emulsions in pigmented rabbits. The animals were dosed either with a 0.8% DXP emulsion at different volumes up to a maximum of 50 μL to test doses up to 400 μg DXP per eye or a 3.2% DXP emulsion at a dose of 1,280 μg DXP. Aqueous humor (AH), vitreous (V), iris/ciliary body (ICB), and retina/choroid (RC) concentrations were determined 1 week and 1, 2, and 8 months after the IVT injection (Figs. 2 and 3) of 0.8% DXP emulsion (DXP doses: 100, 200, and 400 μg). In the anterior segment of the eye, elevated levels of DXP were measured only at 1 week in the ICB, that is, up to 18 μg/g DXP at the 400 μg DXP dose, and decreased rapidly to 6.3, 3.6, and 1.1 μg/g DXP at 1, 2, and 8 months, respectively. In contrast, DXM concentrations transiently reached effective levels (i.e., >100 times the IC50 of DXM for the glucocorticoid receptor) in the ICB only during the first week post-IVT, but decreased rapidly at 1 and 2 months and were below the LLOQ by 8 months. Only the 400 μg DXP dose was able to sustain detectable DXM level by 2 months (118 ng/g). In aqueous humor DXM concentrations remained very low at 1 week (6.1, 10.6, and 20.4 ng/mL for the 100, 200, and 400 μg DXP dose, respectively) and were undetectable by 1-month post-IVT. As demonstrated by the DXP vitreous concentrations, the 0.8% DXP emulsion seems to act as a reservoir and remained in the vitreous over 8 months, even at the lowest 100 μg DXP dose. In contrast, only very low levels of DXM were detected in the vitreous when compared to DXP, with DXM concentrations ranging from 156-fold lower (at 1 week for the 200 μg DXP dose) to 397-fold lower (at 8 months for the 400 μg DXP dose), thus clearly demonstrating that the emulsion retained its integrity and only limited DXP hydrolysis to free DXM takes place within the vitreous. The retina/choroid DXP concentrations were comparable to those observed in the vitreous and therapeutic levels of DXM were sustained over 8 months with the 400 μg DXP dose (Figs. 2D and 3D).
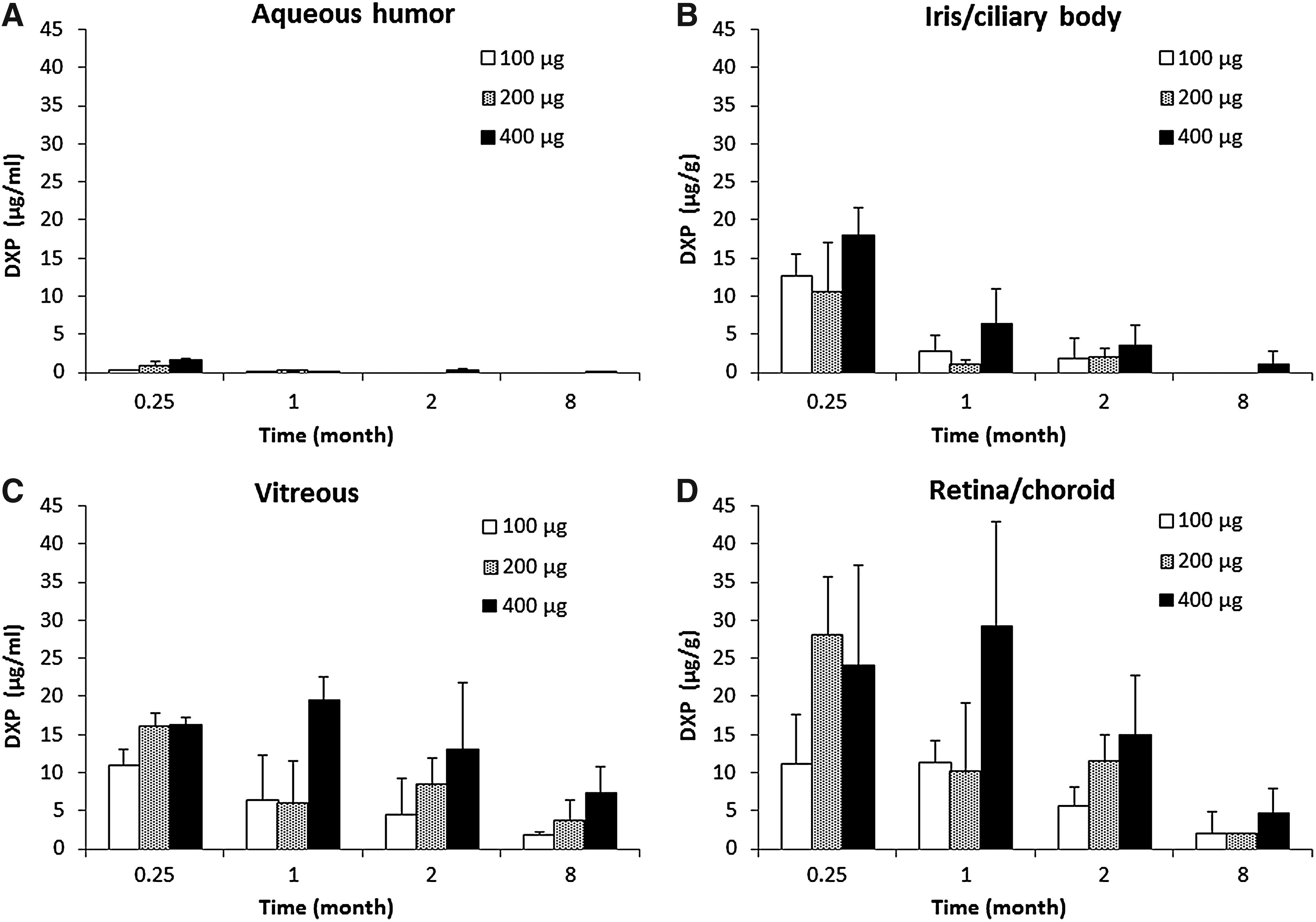
DXP ocular tissue concentrations (μg/g or mL) after a single intravitreal (IVT) in rabbits of 0.8% DXP emulsion (n=8 rabbits per treatment group).
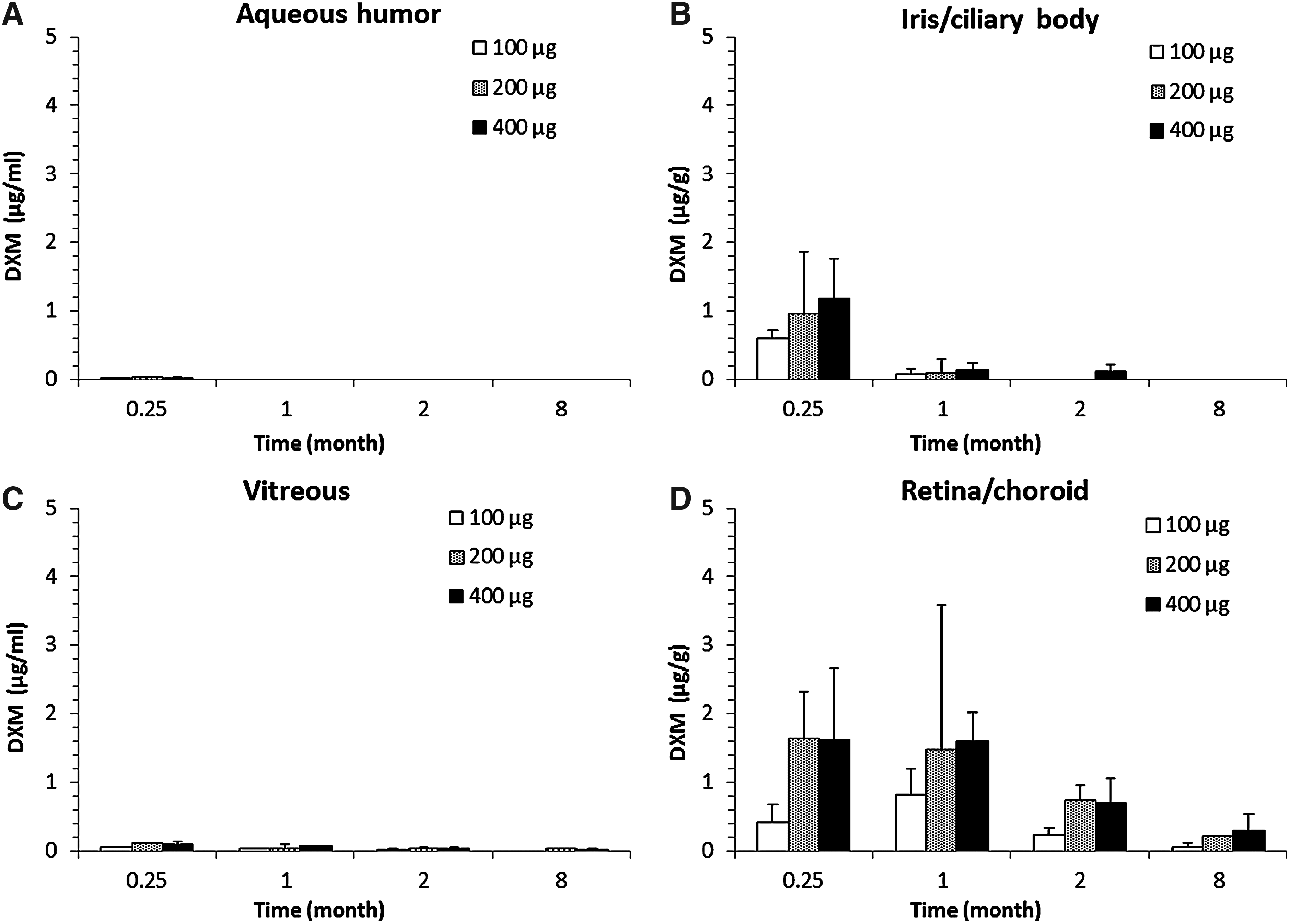
DXM ocular tissue concentrations (ng/g or mL) after a single IVT in rabbits of 0.8% DXP emulsion (n=8 rabbits per treatment group).
With the highest dose (1,280 μg DXP, Table 3), only very low levels of DXM were present in the aqueous humor and vitreous, even at the 1 week time point: 61±57 and 157±18 ng/mL, respectively. In contrast, both retina and choroid DXM concentrations remained elevated at 9 months post administration, measuring 1,175±924 and 577±337 ng/g in retina and choroid, respectively. Vitreous, retina, and choroid DXP concentrations remained elevated throughout the study, with a trend in DXP accumulation after the 2-month time point. These DXM and DXP concentrations were subsequently found to be correlated with the duration of effect as assessed by VEGF challenges in the rabbit.
/, not determined; —, not calculated due to experimental problems during sampling; LLOQ, lowest levels of quantification.
Efficacy of DXP emulsion in a rat model of CNV
The efficacy of 0.8% DXP emulsion was assessed in a rat model of laser-induced CNV. Immediately after verifying the rupture of Bruch's membrane in 8 different spots around the papilla, the rats were injected with either 4 μg DXP, TA (80 μg), or vehicle. The severity of the fluorescein leakage from the induced CNV was assessed on day 7, 14, and 21. The number and the leakage intensity scores of CNV lesions are presented in Table 4, and served to calculate the mean score per treatment group. The mean scores of the vehicle group were used to characterize the percentage of leakage reduction induced by the different treatments. TA (80 μg) was most effective at reducing the severity and incidence of fluorescein leakage throughout the 21-day observation period; that is, 72%, 71%, and 67% reduction for time points 7, 14, and 21, respectively, whereas the 0.8% DXP emulsion (4 μg DXP) reduced fluorescein leakage by 52%, 39%, and 29%, respectively, at the indicated assessment time points. These reductions in fluorescein leakage correlate with the CNV size observed on day 23 on flat-mounted choroid/sclera (Table 5). A 57% CNV size reduction was observed with 0.8% DXP emulsion (4 μg DXP) when compared to untreated controls; 505±461 versus 1,172±719 mm3. By comparison the 80 μg TA dose reduced the CNV size by 77%.
Fluorescein leakage intensity of the angiograms were evaluated by 2 examiners in a masked manner and graded as follows: score 0, no leakage; score 1, slightly stained; score 2, moderately stained; score 3, strongly stained. Mean score calculation: 8 laser burns per right eye of each of the 8 rats per group (i.e., 64 laser burns/group) were performed to induce CNV. The intensity of fluorescein leakage around each one of these 64 laser burns per right eye was scored (from 0 to 3), and the mean score calculated. % of reduction: for each time point, the % of reduction was calculated by comparing the treatment groups' mean score to the vehicle.
TA, triamcinolone acetonide (Kenacort®).
Thus, although the 4 μg DXP dose appeared to be less effective than an 80 μg dose of triamcinolone for reducing CNV size and leakage, these data demonstrate that IVT administration of DXP emulsions is effective for delivering therapeutic concentrations of DXM at the level of the choroid.
Efficacy of DXP emulsion in a rabbit model of VEGF-induced vascular permeability
Rabbit PK data presented in Figs. 2 and 3 and in Table 3 suggest that DXP emulsions can be effective over prolonged periods of time following IVT administration. The duration of effect of IVT DXP emulsions was demonstrated in rabbits challenged with VEGF. IVT injections of rhVEGF165 in rabbits induce an increase in vascular permeability that is easily quantified by the measurement of the intensity of fluorescein leakage. Thus, measuring the intensity of VEGF-induced fluorescein leakage is a direct indication of DXM's potential efficacy for controlling vascular permeability. The efficacy of DXP emulsions (0.56% and 1.12% DXP emulsion) was assessed 4 months after the administration of 280 and 560 μg DXP in the vitreous of pigmented rabbits, and was compared to PBS (control) and TA (2 mg) IVT injections. The data presented in Fig. 4 demonstrate that DXP emulsions significantly reduced VEGF-induced vascular hyperpermeability (p<0.01 when compared to PBS, and p<0.05 when compared to TA). Four months after dosing, the 560 μg DXP dose reduced fluorescein leakage by approximately 84% when compared to PBS, while the 280 μg DXP dose was almost as effective with a 70% reduction in fluorescein leakage. In contrast, although there was broad intra-group variability, TA appeared to be less effective showing no reduction in fluorescein leakage compared to PBS.
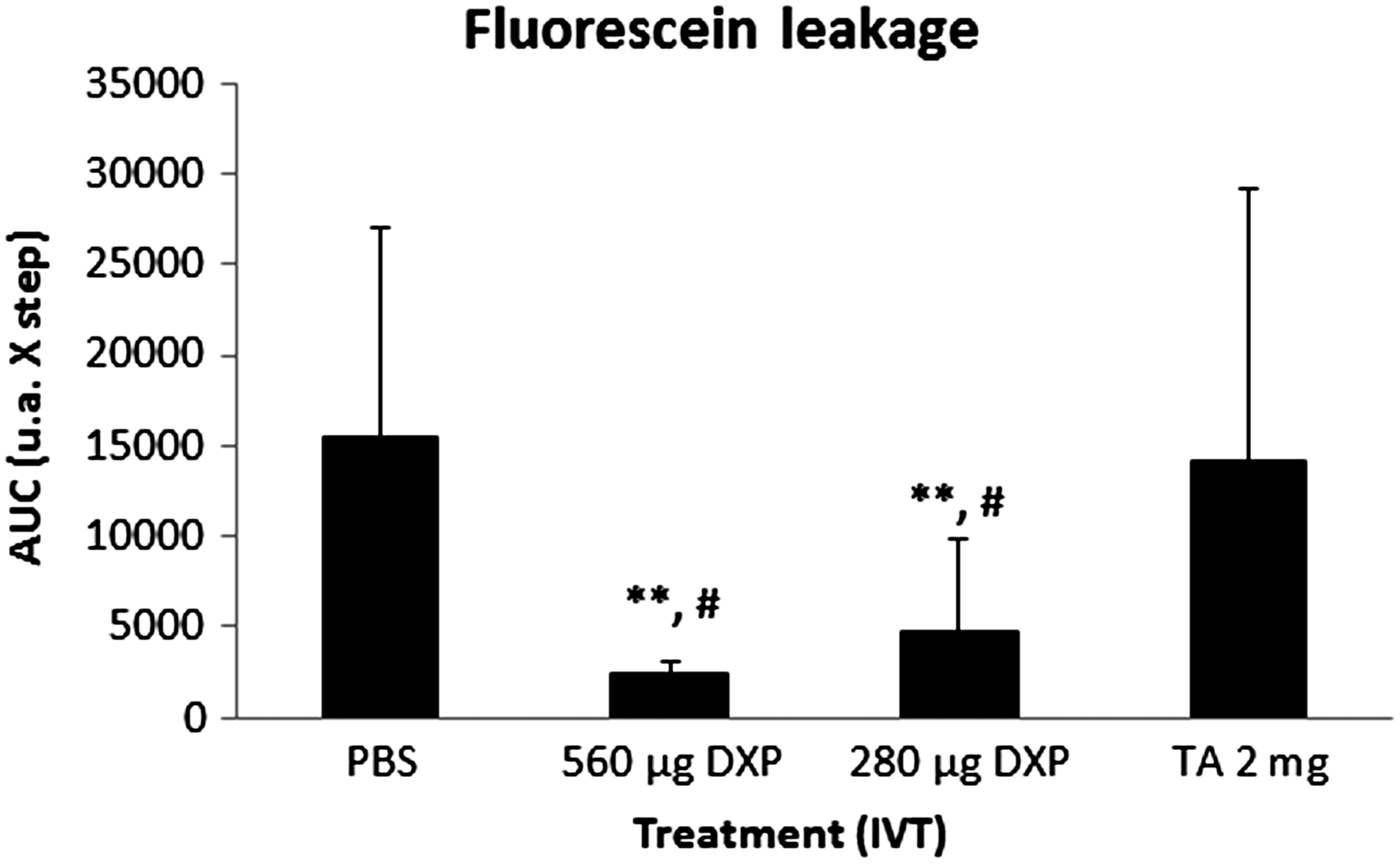
Sustained efficacy of low doses of DXP emulsion in a rabbit model of VEGF-induced vascular permeability (n=6 rabbits per treatment group). **P<0.01 when compared to phosphate-buffered saline (PBS), and #P<0.05 when compared to triamcinolone acetonide (TA).
With the higher 1,280 μg DXP dose VEGF-induced vascular permeability was controlled over 9 months post-IVT administration (Fig. 5) as demonstrated by the ratios of fluorescein leakage in the treated/untreated eyes. In this experiment, the contralateral eye served as control and was representative of a healthy eye; thus, a ratio of 1 indicates that the treatment was able to normalize vascular permeability. Altogether, these data demonstrate that DXP emulsions reduce VEGF-induced retinal vascular permeability and have the potential for sustained duration of effect beyond 6 months following just 1 IVT administration.

Long-term efficacy of high-dose DXP emulsion in a rabbit model of VEGF-induced vascular permeability (n=6 rabbits).
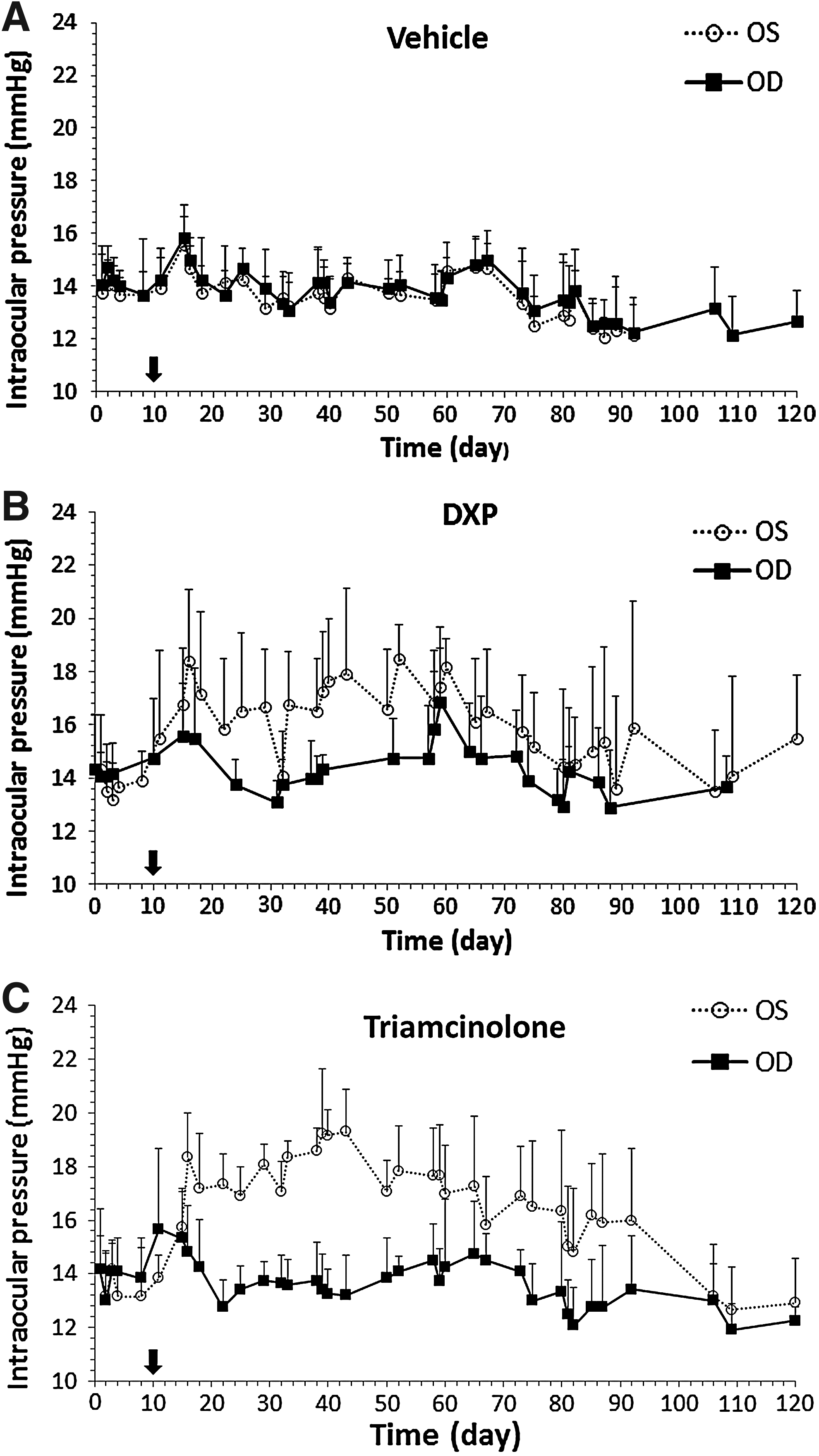
Ocular tolerance of DXP emulsion in a validated feline model of DXM-induced elevated IOP
Since it is well known that the benefits of IVT corticosteroid treatments are offset by the development of ocular complications such as increased IOP, it was of interest to evaluate the potential of DXP emulsions with regard to this particular side effect. For that purpose the effects of a 0.8% DXP emulsion on IOP was explored in a feline model of elevated IOP. Steroid responsive cats, that is, those demonstrated to have an increased IOP following the topical administration of DXM, were given IVT injections of equal volumes of 0.8% DXP emulsion, blank emulsion (vehicle), or TA. The vehicle did not induce any rise in IOP (Fig. 6A). TA induced an increase in IOP that peaked on day 42 at 19.3±2.4 mmHg, a maximum elevation of +5.8 mmHg when compared to the contralateral untreated eye (Fig. 6C). In contrast, an IVT injection of a 0.8% (160 μg DXP) DXP emulsion resulted in a lower, transient IOP increase (maximum IOP peak, 18.42±2.67 mmHg at day 16) which more rapidly returned to normal levels. However, IOP in both the injected and noninjected eyes showed more variability over the study period (Fig. 6B). At the end of the study it was noted that 6 months post-IVT most of the TA injected eyes (5/6) had developed cataract, while none (0/6) of the 0.8% (160 μg DXP) DXP emulsion injected eyes showed cataract.
Comparison of the ocular hypertensive effect of
Short- and long-term safety assessment of DXP emulsions in rabbit and minipig preclinical models
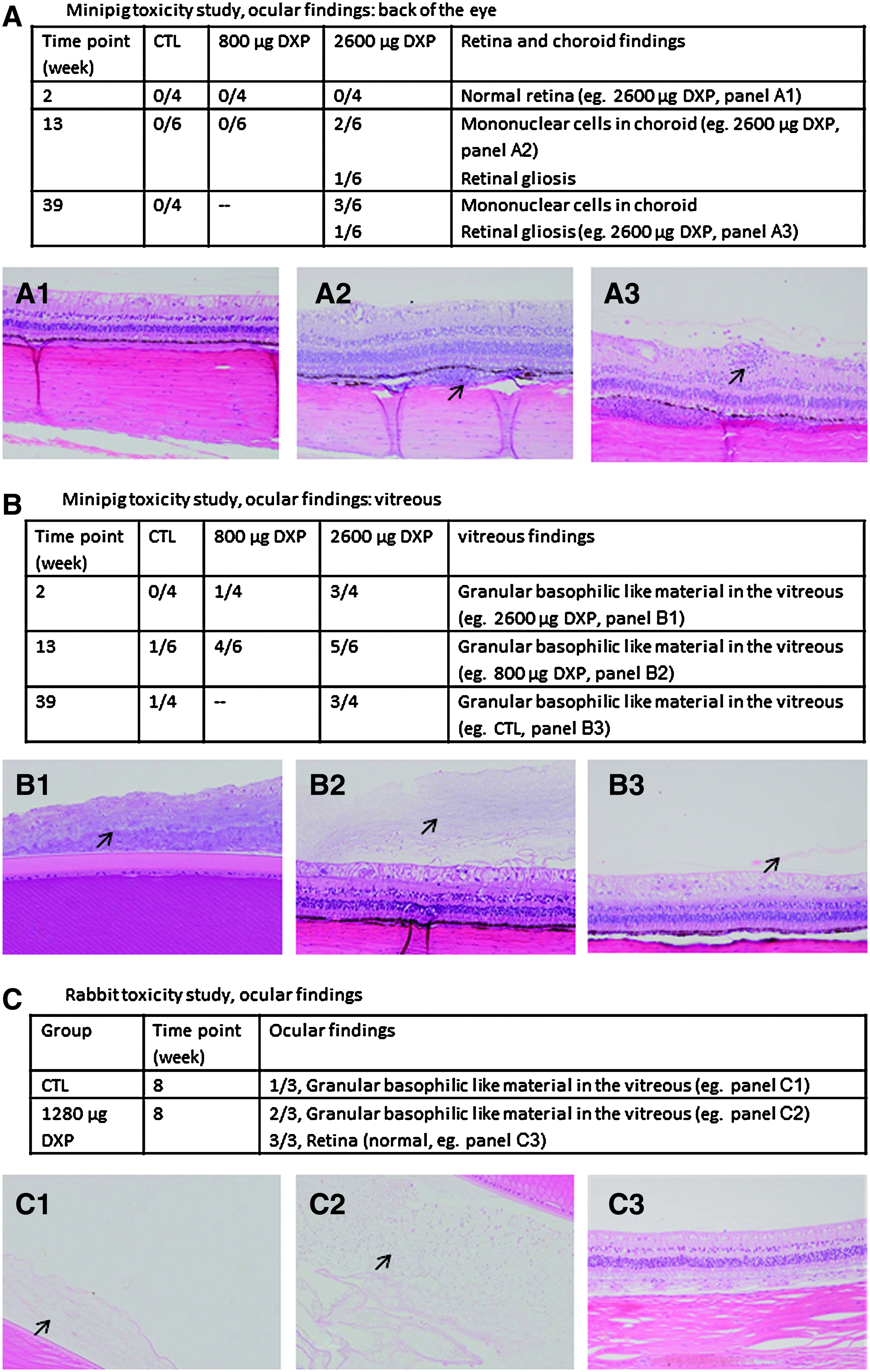
Ocular and general safety was assessed in both rabbits and minipigs. The rabbit is a more sensitive species and, therefore, maybe better suited for the characterization of the ocular early side effects that might result from the IVT injection of DXP emulsions. A long-term safety study in the minipig (9 months) was designed to evaluate primarily the systemic toxicity and local tolerance of DXP emulsions. Table 6 summarizes the findings of the 8-week rabbit and 39-week minipig studies (Fig. 7). In the rabbits, the no observed adverse effect level was set at 1,280 μg DXP. Neither ocular nor systemic side effects were observed at this dose. Histopathologic examination of ocular tissues was remarkable only for granular amorphous material in the vitreous cavity that was hypothesized to represent the dispersed emulsion (Fig. 7C). The toxicokinetic findings after bilateral injections of 1,280 μg DXP demonstrated that low levels of DXM were detected in plasma both on day 15 and 1 month post-IVT; 1.51±0.56 and 0.66±0.18 ng/mL, respectively. DXP levels remained below the LLOQ (0.5 ng/mL) throughout the study.
Minipig
DXM, dexamethasone; DXP, dexamethasone palmitate; ILQ, inferior to the limit of quantification (LLOQ at 0.5 ng/mL for both DXP and DXM); ND, not determined; NOAEL, no observed adverse effect level; NOSEL, no observed systemic effect level.
Two doses were tested in minipigs: 800 and 2,600 μg DXP. No abnormal ocular or systemic findings were reported at the lowest dose. Microscopic evidence of ocular toxicity described as a mononuclear cell infiltration in the choroid and retinal gliosis was observed at the high dose (Fig. 7A, B) at week 13, and 39 time points. In contrast, no systemic toxicity findings were observed at the high dose, and the plasma concentration profile remained below the LLOQ for both DXP and DXM, except for DXM in 1 animal (out of 10) on day 1 in the high-dose group. Hence, the no observed systemic effect level was set at 2,600 μg DXP in the minipig. Collectively, these data demonstrate that DXP emulsion injections were safe up to a dose of 1,280 μg DXP.
Discussion
The studies presented in this report demonstrate that IVT injections of DXP emulsions are an effective vehicle for the sustained IVT delivery of DXM to the back of the eye (retina and choroid). Following a single IVT administration of the DXP emulsion DXM was present in the retina and choroid for extended intervals at concentrations sufficient to inhibit VEGF-induced vascular hyperpermeability in rabbit eyes. In addition, DXP emulsions were well tolerated in both rabbit and minipig at doses as high as 1,280 μg DXP, equivalent to an IVT injection of 800 μg DXM. Hence, these data provide the rationale for IVT injections of DXP emulsions as an innovative therapeutic approach to the treatment of macular edema17–22 associated with chronic posterior segment eye diseases.
DXP is a long-chain fatty acid ester of DXM, the pharmacologically active ingredient. Free DXM is formed in vivo by hydrolytic cleavage of the palmitate-ester linkage by esterases, ubiquitous enzymes known to play a role in the specific activation of prodrugs. In the eye, esterases capable of cleaving DXP to DXM have been identified in the cornea, iris/ciliary body, retina, and choroid,23–25 but not in the lens. Additionally, the prodrug DXP can be hydrolyzed to free DXM by plasma esterases (data not shown). 26 The conversion of DXP to DXM only in the tissues allows DXP to serve as an IVT reservoir for DXM, limits the dispersion of free DXM reducing the potential for corticosteroid side effects, and localizes the anti-inflammatory and angiogenic effect of DXM on the target tissues. As only very low amounts of free DXM are present in DXP emulsions, less than 0.05% of the DXP strength of DXM, the levels of DXM detected in ocular tissues (Fig. 3) can only be explained by the hydrolysis of the prodrug by the intraocular tissue esterases.
The PK profile of both DXP and DXM demonstrated that IVT injections of DXP emulsions were able to deliver substantial amounts of the prodrug to the retina/choroid. DXP was present up to 9 months at the highest dose (1,280 μg DXP, Table 3), and even at the lower doses DXP was detectable in the retina/choroid at 8 months (Fig. 2D). Vitreous DXP concentrations correspond to the quantification of the remaining oil droplets present in the vitreous and their solubilized DXP content. Since DXP is very lipophilic, it is very unlikely that DXP diffused from the oily core of the emulsion toward the aqueous environment of the vitreous. Thus, DXP vitreous concentrations represent a measure of the emulsion present within the vitreous. The very low levels of DXM found in the vitreous suggested that the emulsion is stable and not degraded. It appears that DXP emulsions act as a sustained IVT drug delivery vehicle that is maintained unaltered in the vitreous, with a slow elimination rate. The emulsion being cleared from the vitreous through the combination of 2 mechanisms; through the front of the eye where unaltered oil droplets are flowing with the aqueous humor, and through the back of the eye where the oil droplets release the prodrug into the retina. Both routes being modulated by the emulsion oil droplets size and composition.
The PK profile of DXM in the retina and choroid mimics the one observed with PLGA/DXM implant (Ozurdex®), 27 an initial burst followed by a sustained release that allows for the detection of DXM in the retina and choroid until 8 or 9 months post-IVT injection, depending on the administered dose.
Corticosteroids exert their anti-inflammatory effects by modulating VEGF and many other transduction pathways.11,22,28,29 The PK data can be correlated to the efficacy data which demonstrated that DXP emulsions were able to reduce VEGF-induced vascular hyperpermeability in a dose-dependent manner (Fig. 4) and up to 9 months (Fig. 5). For the management of chronic diseases, such as diabetic macular edema, this sustained efficacy observed with DXP emulsions could allow for a reduced number of IVT injections per year relative to the required number of injections required for anti-VEGF therapies. The long-lasting effect of DXP emulsions might be the combination of (1) the long residence time in the vitreous of the emulsion itself, where it acts as a reservoir for the sustained release of the lipophilic prodrug, and (2) the slow metabolic conversion of DXP in free DXM in the retina and choroid. In addition, the lipophilic nature of the prodrug allows for its accumulation in the choroid/RPE, where it forms a second reservoir as demonstrated by IVT injections of high doses of DXP oil solution (data not shown). Regarding the active principle there is no difference between DXP emulsion and Ozurdex (Allergan); DXM in both cases. The difference resides in the mean used to deliver DXM; a solid PLGA implant of water soluble DXM in the case of Ozurdex and an oil-in-water emulsion of the water insoluble prodrug DXP in the case of the DXP emulsion. Both approaches allow for a sustained release and prolonged efficacy of DXM. In the case of Ozurdex, DXM is first solubilized in the vitreous before it reaches the retina. As a consequence, elevated levels of DXM are found in rabbit vitreous (up to 791 ng/mL 22 days post-IVT injection of the implant), 30 that may lead to increased risks of side effects. In contrast, the risks of DXM-associated side effects (cataract and glaucoma) with the DXP emulsion are reduced since there is no free DXM in the vitreous of animals treated with the DXP emulsion.
The ocular side effects of the corticosteroids are well known and the evidence to date suggests that they may be unavoidable.2–6 All approved corticosteroids for IVT administration, TA solutions (Trivaris®, Allergan; Triescence®, Alcon), and FA (Retisert®; Bausch and Lomb) and DXM (Ozurdex; Allergan) 31 implants are known to result in elevated IOP and cataract formation. Jaffe et al. 5 reported that 51% of the patients treated with FA implants required anti-glaucoma medications, 5.8% underwent glaucoma-filtering surgery, and cataract progression occurred in 19.8% of phakic eyes. Moreover, Pearson et al. 32 demonstrated that very high IOP (≥30 mmHg) was recorded in 61.4% of treated eyes, with 33.8% requiring surgery for ocular hypertension by 4 years, and 91% of treated phakic eyes had cataract extraction by 4 years. DXM implants were associated with increased IOP in 17% of patients. 33 These side effects were all directly associated to the drugs action on the lens, trabecular meshwork, and ciliary body cells.34–36 Hence, it appears that it is important to lower DXM levels in the anterior part of the eye to avoid the aforementioned side effects. The PK profile of DXP emulsions demonstrated that even high doses of a 3.2% DXP emulsion (1,280 μg DXP) did not result in sustained, high levels of free DXM in the aqueous humor and vitreous (Table 3); thus, the risk of elevated IOP and cataract formation following DXP emulsion injections are anticipated to be lower than with other intravitreally administered corticosteroid therapies.
The ocular and systemic safety of DXP emulsions was assessed in rabbits and minipigs, and a feline model of DXM-induced elevated IOP 14 was used to evaluate the potential of an IVT injection of DXP emulsion at increasing IOP. The data summarized in Table 6 and in Figs. 6 and 7 demonstrated that DXP emulsions are well tolerated at doses as high as 1,280 μg DXP/eye, with normal IOP and no cataract formation. However, in steroid responsive cats DXP emulsions demonstrated the potential to transiently increase IOP although to a lesser extent than triamcinolone. Although no cataract formation was evident at 6 months in cats given the slower evolution of cataract development it cannot be concluded that DXP emulsions will not induce cataracts. Ultimately, additional studies at the most appropriate selected therapeutic dosage will be needed to more accurately determine the side effect profile of DXP emulsions. However, based on the findings in this study it can be anticipated that DXP emulsions might have a better safety profile over a long period of time relative to other approved intravitreally administered corticosteroid therapies since only very low levels of free DXM are present in the vitreous.
To adequately manage the expected future increase in macular edema, more convenient therapies with better safety profiles will be needed. In this study we found that a single IVT injection of DXP emulsion resulted in the presence of therapeutic levels of DXM in the retina and the normalization of VEGF-induced vascular permeability for up to 9 months. The overall safety profile of DXP emulsion at doses as high as 1,280 μg DXP suggests that this approach might serve as a promising therapeutic alternative to improve the management of chronic posterior segment ocular diseases complicated by macular edema.
Footnotes
Author Disclosure Statement
P. Daull: Novagali employee; J.-S. Garrigue: Novagali employee; C. Paterson: none; B. Kuppermann: none.