
Abstract
Abstract
Purpose:
To report on tamoxifen crystalline maculopathy in an 80-year-old patient and to review the ocular side effects of oral tamoxifen.
Methods:
We report a case of an 80-year-old female patient who presented to our ophthalmic institute with painless gradual progressive diminution of vision in both eyes. She had a history of surgery for breast cancer after which she had been treated with oral tamoxifen citrate for 2 years before presentation.
Results:
Our patient had profound visual impairment in both eyes. The anterior segments were found to be normal; in particular, the corneas were clear; the intraocular pressures in both eyes were 12 mm Hg. The perimacular region in both eyes showed deposits of multiple, fine crystalline material. Color vision was found to be impaired in both eyes and optical coherence tomography (OCT) confirmed the diagnosis of tamoxifen-induced maculopathy.
Conclusion:
Tamoxifen is a selective estrogen receptor modulator widely used in the treatment of hormone-responsive breast cancer. Ocular complications are rare with tamoxifen therapy and include cataract, vortex keratopathy, optic neuritis, and retinopathy. Crystalline maculopathy is one of the rare side effects of long-term tamoxifen use, which can be detected by noninvasive diagnostic tools such as OCT. Our patient is the oldest such patient reported in literature. Patients receiving tamoxifen therapy must be informed about the potential side-effects, and the need for serial ophthalmic examination to detect early signs of toxicity.
Introduction
Case Report
We report the case of an 80-year-old female patient who presented to our clinic with complaints of gradual progressive diminution of vision in both eyes over the past year. Her past medical history included a radical modified mastectomy of the left breast for cancer 2 years ago and subsequent initiation of oral tamoxifen, which had been recently discontinued as per the advice of the patient's treating physician. She was on a dose of 20 mg of tamoxifen per day and had received a cumulative dose of 14 g. On examination, her best-corrected visual acuity was 3/60, N12 in the right eye and 6/60, N12 in the left eye. External examination and pupillary evaluation were normal. Color vision using Ishihara's pseudoisochromatic color plates showed impaired color vision. Slit lamp examination revealed clear corneas and quiet anterior chambers in both eyes. The right eye showed a grade II nuclear sclerosis, whereas the left eye had a posterior chamber intraocular lens in situ following a cataract extraction surgery 6 years before presentation. Intraocular pressures in both eyes were within normal limits. On dilated fundus examination, the optic discs showed temporal pallor. The perimacular region showed multiple, fine, crystalline deposits in both eyes (Fig. 1). A clinical diagnosis of tamoxifen-related maculopathy in both eyes was made. Humphrey's visual fields showed cecocentral and inferior defects in both eyes. A fundus fluorescein angiogram was advised, which the patient declined. Optical coherence tomography (OCT) (Carl Zeiss Meditec, Inc., Dublin, CA) was performed (Fig. 2), and the left eye showed loss of foveal contour and pseudocyst formation, which is typical of tamoxifen maculopathy. There was also focal disruption of the photoreceptor line. The foveal thickness in both eyes was normal at 162 μm. The right eye, however, showed a large cystic space seen subfoveally; a shallow foveal contour was seen and a few hyper-relective dot-like echoes were seen intraretinally at the fovea suggestive of crystalline deposits. There was no macular edema seen. Since her treating physician had already advised her to stop tamoxifen, a cataract surgery was offered in the right eye, which the patient declined. The patient was subsequently lost to follow-up.
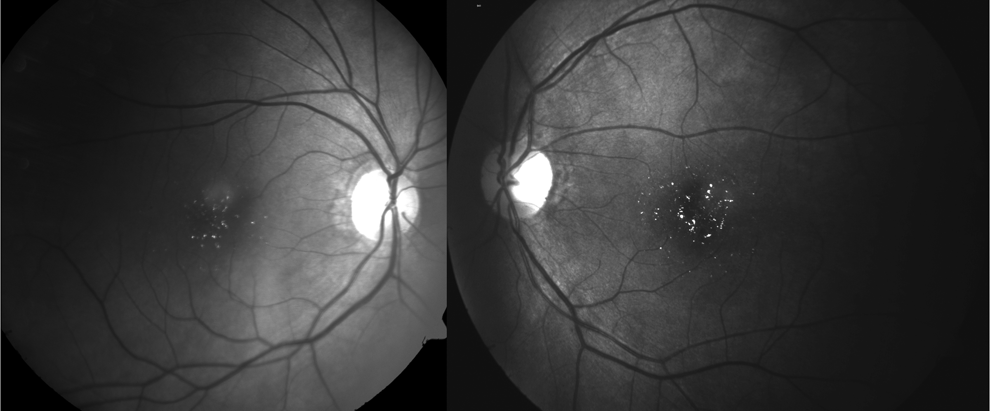
Red-free fundus photographs showing multiple, discrete, crystalline deposits in the perimacular area in both eyes.

Optical coherence tomography (Carl Zeiss Meditec, Inc., Dublin, CA): in the right eye
Discussion
The various ocular side effects of tamoxifen that have been described in literature include crystalline maculopathy, macular edema, keratopathy, optic neuritis, and cataract formation (Table 1). The structure of tamoxifen is similar to other cationic amphiphilic drugs known to produce retinopathy and keratopathy, such as chloroquine, chlorpromazine, thioridazine, and amiodarone hydrochloride. 4
Corneal toxicity seen in patients on long-term tamoxifen includes subepithelial deposits, whorls, and linear deposits. The whorl-like or linear subepithelial opacities, white to brown in color, are often bilateral and occur in the inferior and occasionally the central portions of the cornea. Subepithelial lines may appear as obliquely oriented brown streaks or discreet horizontal lines in the center of the cornea and may occur in both eyes. 5 Corneal toxicity has been reported to be reversible with the stoppage of tamoxifen therapy. 6
Tamoxifen retinopathy classically is characterized by the presence of small crystalline deposits that may occur in the nerve fiber and inner plexiform layers near the fovea. 7 Kaiser-Kupfer reported that they found white refractive opacities superficial to retinal blood vessels, forming clusters located in the paramacular and foveal areas, with the highest concentration temporally. 3 These deposits are often associated with macular edema, that is, the accumulation of fluid within the retinal cellular layers, and subsequently, impaired visual acuity. Small numbers of crystals seem not to cause visual acuity loss. 5 However, microcystoid maculopathy may occur even without the presence of crystalline deposits in an apparently normal looking fundus. 8
The reported prevalence rates of tamoxifen retinopathy for breast cancer survivors using standard doses vary substantially between studies, from <1% to about 6%. 7 Although tamoxifen retinopathy typically is considered to depend on total cumulative dose, spectral-domain OCT can reveal foveal cystoid spaces within only a year or two of the start of tamoxifen use for some patients on contemporary dosing levels, which are 20 mg/day as was the case in our patient.5,9 Interestingly, unlike tamoxifen keratopathy, the induced retinopathy does not reverse when treatment with tamoxifen is stopped.
It has been suggested that tamoxifen may act as an antagonist of glutamate transporters in retinal pigment epithelium cells. 10 This leads to an increase in glutamate, leading to axonal degeneration, which has been noted histopathologically. 11 Müller cell impairment may follow a retinal neuron injury and generate atrophy and formation of an intraretinal foveolar cyst.12,13 These foveolar cystoid spaces or pseudocysts seen on OCT have been described as being pathognomonic of tamoxifen-induced maculopathy and is an indication to discontinue treatment. 14 Previously described reports indicated the presence of macular edema; 3 however, there have been a few reports that have not shown any increase in foveal thickness,13,14 as was noted in our patient. Furthermore, as was noted in our case, in the absence of any other pathology, the need for an invasive investigation such as fundus fluorescein angiography is obviated with the advent of OCT, which can diagnose tamoxifen maculopathy.
The histopathological examination of a patient who had characteristic retinal deposits showed that the lesions were restricted to the nerve fiber layer and inner plexiform layers and stained for glycosaminoglycans, perhaps representing the previously described axonal degeneration. This could probably explain the associated visual loss, which is not a classic feature of other crystalline retinopathies.11,15
Tamoxifen-related ocular toxicity, although rare, can be distressing for the patient. While keratopathy is readily reversible, maculopathy—a vision-threatening side effect of long-term treatment—may not reverse with cessation of treatment. Physicians treating with tamoxifen therefore must encourage patients to undergo a baseline ophthalmic examination before treatment initiation, as well as periodic evaluations—preferably six monthly—during the treatment to detect early signs of retinal toxicity. In the monitoring of such patients, OCT plays an important role to detect subclinical changes associated with the toxicity.
Footnotes
Acknowledgments
The authors would like to acknowledge the assistance provided by Veena Iyer, M.D.; Department of Diagnostic Radiology, the University of Minnesota, Minneapolis, MN.
Author Disclosure Statement
No competing financial interests exist.