
Abstract
Abstract
Purpose:
To describe the retinal changes occurring after Ozurdex® (Ozurdex, Allergan, Inc., Irvine, CA) injection and peripheral laser treatment in a case of central retinal vein occlusion (CRVO).
Case Report:
A 51-year-old Caucasian man with massive retinal edema (926 μm) and hand motion visual acuity due to severe CRVO was treated early with Ozurdex intravitreal injection. Detailed monthly follow-up examinations showed complete resorption of the edema (253 μm) after 2 months and a 20/32 visual outcome after 3 months. The patient subsequently developed peripheral retinal ischemia accompanied by recurrence of small retinal cystoid spaces (295 μm); therefore, he underwent an associated laser treatment on the involved peripheral retina, which led to a recovery in retinal thickness (280 μm). His visual acuity remained stable at 20/32.
Conclusions:
Early Ozurdex injection in association with late laser photocoagulation was effective in the resorption of CRVO macular edema and in restoring reasonably good visual acuity.
Introduction
The full pathogenesis of macular edema in CRVO is not yet completely understood. It may involve many different factors triggered by vein occlusion, including the hydrostatic effect from increased venous pressure, secretion of inflammatory cytokines, deregulation of endothelial tight-junction proteins, and increased levels of vascular permeability factors, such as the vascular endothelial growth factor (VEGF). 6 Consequently, multiple treatment strategies have been attempted for the treatment of macular edema, including laser photocoagulation, anti-VEGF injections, to control both neovascularization and exudation, and corticosteroid injections to attenuate the inflammatory pathway that leads to macular edema. Incidentally, corticosteroid therapy, although widely used with fairly good clinical results, is limited by the numerous adverse effects associated with prolonged steroid administration, such as increased intraocular pressure (IOP) and cataract formation.7,8 The significant efficacy of corticosteroid intravitreal injection (preservative-free triamcinolone) to treat macular edema was shown for the first time in 2009 by the SCORE study, but only relative to CRVO (compared to observation only); in cases of branch retinal vein occlusion (BRVO), triamcinolone treatment did not appear to be superior to macular grid laser photocoagulation.9–11 At present, many pharmacological corticosteroid molecules, with varying potency levels, concentrations, and half-lives are available for intravitreal injections. Triamcinolone acetonide has been widely used and reviewed due to its vitreous injectable property, while dexamethasone, which is approximately 5 times more potent than triamcinolone acetonide and also more hydrophilic,12,13 has had limited clinical utility due to a very short half-life (3 h). 14 To avoid this drawback, a dexamethasone delivery system has recently been released (Ozurdex®, Allergan, Inc., Irvine, CA) that facilitates sustained delivery of preservative-free dexamethasone to the vitreous cavity and retina. 15
Herein, we report a case of severe CRVO that was treated early with Ozurdex vitreal injection.
Case Report
A 51-year-old Caucasian man came to our emergency service in April 2011 due to sudden and severe visual loss in his left eye oculus sinister (OS), which had started 2 h before. Upon medical examination, best corrected visual acuity was 20/20 in the right eye oculus dexter (OD) and hand motion in the OS. Pupils were normal, with a moderate relative afferent defect in the OS. Anterior segment examination revealed normal findings bilaterally, and the IOP was 14 mm Hg. Fundus examination in the OS showed massive retinal edema with diffused hemorrhages, disc swelling, cotton-wool spots, and tortuous and dilated retinal veins in all 4 quadrants; a diagnosis of CRVO was made. Fluorescein angiography (FA) showed cystoid macular edema with many superficial hemorrhages and massive swelling, and diffused capillary dilatation and leakage (Fig. 1A), but it did not show ischemia. The right eye was normal in both ophthalmoscopy and FA. Optical coherence tomography (OCT) examination revealed a considerable increase in retinal thickness, with a central value of 926 μm. Large cystoid spaces distributed over 2 or more layers were visible, although image quality was poor, mainly in the outer retinal layers, due to the massive amounts of dense fluid. The external limiting membrane (ELM) appeared to be intact throughout its length. Moreover, a subretinal serous detachment was faintly visible.
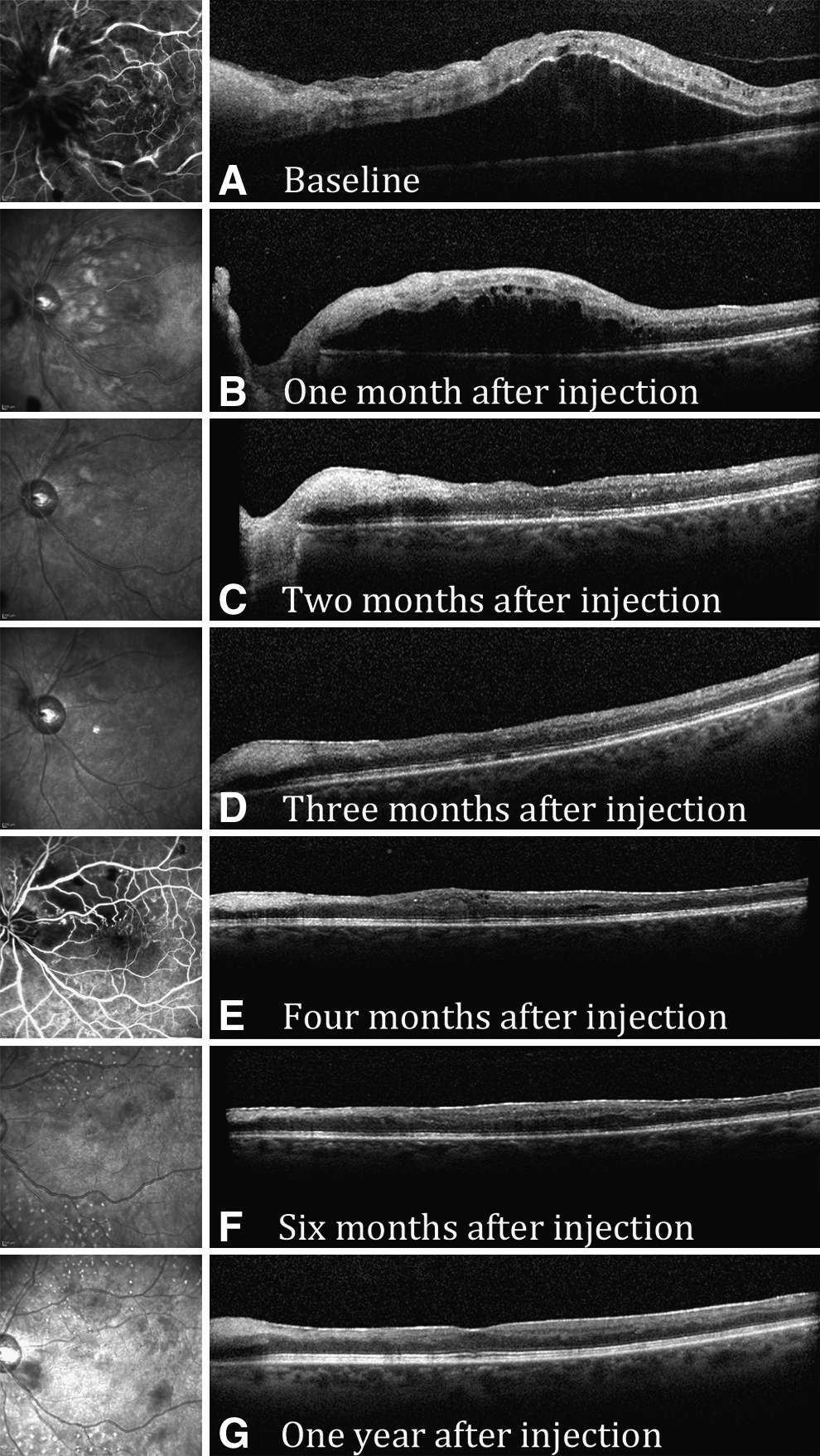
Reperfused central retinal vein occlusion with massive cystoid macular edema and swelling before and after therapy with intravitreous injection of dexamethasone implant (Ozurdex®, Allergan) associated with laser photocoagulation. 1-year follow-up.
The patient's medical history was negative for any significant systemic pathology, and he denied substance abuse that could have contributed to CRVO, such as smoking and the use of illicit drugs. The results of laboratory tests, including a complete hypercoagulability and thrombotic workup (assessment of dyslipidemia, inflammatory diseases, hyperhomocysteinemia, factor V Leiden mutation, deficiency in protein C or S, prothrombin gene mutation, and anticardiolipin antibodies) were negative, but repeated measurements of blood pressure showed uncontrolled hypertension; average systolic pressure was 170 mm Hg and diastolic pressure was 110 mm Hg. The patient was therefore prescribed aspirin 100 mg daily, and 10 mg amlodipine and 25 mg hydrochlorothiazide were added to achieve better blood pressure control.
Five days after the onset of CRVO, Ozurdex injection was proposed to the patient, and after obtaining written informed consent, the drug was injected.
Follow-up visit 1 (30 days)
OS visual acuity was counting fingers. FA and OCT analysis showed reduced retinal thickness (680 μm), but the large cystoid spaces were still visible and placed in 2 different layers: between the outer nuclear and plexiform layers and in the inner nuclear layer (Fig. 1B). IOP was 18 mm Hg.
Follow-up visit 2 (60 days)
Visual acuity had significantly improved to 20/50, and OCT examination showed a significant thinning of the retina at 253 μm. The foveal depression as well as the retinal layers had regained an almost normal appearance, without any cystoid space, although the IS/OS interface and ELM were hyper-reflective and slightly uneven (Fig. 1C). Serous detachment was completely resolved, whereas some hyper-reflective dots gleamed in the outer nuclear and plexiform layers. IOP increased to 25 mm Hg; therefore, IOP-lowering therapy was initiated along with administration of a timolol–dorzolamide fixed combination twice daily.
Follow-up visit 3 (90 days)
Visual acuity had further increased to 20/32, and retinal appearance was nearly normal. OCT showed a smoother IS/OS interface and ELM. Hyper-reflective dots had mostly disappeared, while retinal pigment epithelium appeared perfectly normal (Fig. 1D). IOP had dropped to 20 mm Hg on therapy, and no other adverse effects were noticed.
Follow-up visit 4 (120 days)
Visual acuity was still 20/32, but OCT showed a slight increase in retinal thickness to 295 μm with the reappearance of small cystoid spaces in the inner retinal layers (Fig. 1E). Moreover, FA showed the onset of retinal ischemia next to the optic disc with extension mainly to the upper and temporal quadrants. The area of retinal capillary obliteration was 10 discs, with sparing of the macula. Laser photocoagulation of the ischemic retina was done in an attempt to reduce macular thickness.
Follow-up visit 5 (180 days)
The patient's visual acuity remained stable at 20/32. FA did not show any further retinal ischemia, and OCT showed light central retinal thickness reduction to 280 μm with the disappearance of the small cystoid spaces, although the retina lost the foveal depression and was diffusely thickened and hyporeflective in the outer layers (Fig. 1F).
1-year follow-up visit
Visual acuity was stable at 20/32, and OCT showed a further thickness reduction to 231 μm in the central macular subfield with no intraretinal edema. The IS/OS line was present with a slight subfoveal irregularity. A small foveal depression had reappeared despite the presence of a thin epiretinal membrane.
Discussion
It has recently been demonstrated in a multicenter study that Ozurdex is effective in reducing macular edema, and thereby improving visual acuity in both CRVO and BRVO. This is apparently due to the progressive release of dexamethasone that evidently ensures a prolonged action lasting between 4 and 6 months, with a concomitant attenuation of the possible complications, such as refractory glaucoma and cataract.16,17 In that study, performed by the Ozurdex Geneva Study Group, a significant difference in visual acuity was found between the dexamethasone implant and sham groups at day 180 from injection, although there was no between-group difference in retinal thickness at that time point. This suggests that other factors in addition to changes in central retinal thickness may affect visual acuity in RVO eyes with macular edema, 16 and it is also consistent with the first report of the SCORE study, in which the correlation between OCT-measured center point thickness and visual acuity letter score was poor and, therefore, this correlation cannot reliably be substituted for visual acuity measurements. 18
The case of CRVO we report herein showed partial conversion to the ischemic form (10 discs area of retinal ischemia only) and was successfully treated with a single injection of dexamethasone implant associated with peripheral laser photocoagulation.
While visual acuity was severely impaired at presentation (hand motion), consistent with the clinical course of younger patients with CRVO, 19 the treatment produced a significant improvement in visual acuity (more than 6 ETDRS lines), accompanied by an excellent recovery in retinal thickness, which had returned to normal values just 2 months after the injection. The recovery of visual acuity we observed may also be explained by the early commencement of therapy, since it has been shown in a post hoc analysis that the response to treatment is often greater among eyes with a shorter duration of macular edema at baseline (<90 days) compared to those with a longer duration. 16 It has also been shown that in cases of late treatment with Ozurdex injection, the results obtained are weaker, although still present. 20
Since central vision was good, peripheral laser photocoagulation of the ischemic retina could be performed without unduly compromising the visual field, in an attempt to reduce macular edema. Although visual acuity did not improve, central retinal thickness reduced from 295 to 231 μm following photocoagulation. Laser-induced reduction of macular edema in CRVO is consistent with the findings of a previous study reported by the Central Vein Occlusion Study Group. 21
According to the Geneva Study Group and other authors, the peak of treatment efficacy occurred at the 60th day, when vitreous concentration was the highest, and was maintained through to the 90th day. Subsequently, it faded slightly probably due to the Ozurdex implant being designed to deliver therapeutic levels of dexamethasone for a maximum period of 6 months.15–17
Anti-VEGF administration is an effective alternative therapy for RVO. CRUISE and BRAVO studies compared ranibizumab with a placebo in eyes with macular edema secondary to CRVO or BRVO, respectively.22,23 Ranibizumab-treated eyes with CRVO fared significantly better than sham-treated eyes, gaining ≥15 letters in 46.2% for the 0.3 mg group and 47.7% for the 0.5 mg group. Results from BRAVO were similar. 23 In any case, a direct comparison of results from SCORE, BRAVO, and CRUISE studies with Ozurdex is difficult due to the differing patient populations and study designs among the studies. In this regard, the COMO study is being completed to directly compare Ozurdex and ranibizumab in BRVO. In the case reported herein, in accordance with the patient, we preferred to inject the dexamethasone implant to obtain a longer lasting effect and to reduce the total number of injections required.
The only side effect we encountered in 1-year follow-up was an IOP increase (28 mm Hg) promptly controlled with topical therapy (timolol–dorzolamide fixed combination). No lens opacities were observed and this is consistent with a previous phase 2 trial of dexamethasone implant that found low rates of both cataract development and IOP increase.24,25 Nevertheless, a longer administration and observation period is probably needed to better evaluate cataract progression, as ascertained in the 12 months of results reported by the Geneva Study. 26 Neither anterior chamber inflammation after injection nor neovascularization or rubeosis was found, despite mild retinal ischemia. Follow-up visits are required to evaluate the need for retreatment, which could be recommendable if retinal thickness increases over 250 μm in the central 1-mm macular subfield with a visual acuity still less than 20/20, as proposed as retreatment criteria by Haller et al. 26
In conclusion, the Ozurdex implant may be a valuable new treatment option for eyes with visual impairment due to macular edema related to ischemic CRVO, and may be safely administered in conjunction with peripheral laser treatment with no risk of excessive damage to the visual field, due to the good macular outcome. Further studies with longer follow-up are needed to better understand the long-term efficacy of treatment and to evaluate the possibility of PRN retreatment, also in comparison with anti-VEGF drugs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.