
Abstract
Abstract
Purpose:
The aim of this study was to investigate the immunosuppressive activity of a mycophenolate mofetil (MMF) intraocular-implantable drug delivery system (IDDS) in a rabbit model of high-risk penetrating keratoplasty and to determine the biocompatibility of such a device when implanted in the anterior chamber.
Methods:
Corneal vascularization was induced in New Zealand white rabbits by passing 5-0 silk sutures through the corneal stroma in each quadrant. The corneal neovascularized rabbits received a unilateral 7-mm-diameter central-penetrating keratoplasty. New Zealand white rabbits were used as donors and were divided into 4 treatment groups: the control group, which received no therapy; the 1% MMF eye drop group; the 1.0 mg cyclosporin A (CsA)-IDDS-implanted group; and the 1.0 mg MMF-IDDS-implanted group. Animals were followed up for 150 days, which involved examination of the corneal allografts (opacity, edema, and neovascularization) by slit-lamp biomicroscopy. The survival time of corneal allografts of these animal models was recorded in 4 groups. Histopathologic studies were carried out on the procured specimens of corneal allografts. The biocompatibility of MMF-IDDS in the anterior chamber in rabbits was also investigated.
Results:
The mean survival time of corneal allografts in the control and MMF eye drop groups was 18.7±3.0 and 37.5±6.2 days, respectively (P=0.005). Allografts from the CsA-IDDS-implanted group were transparent, except 1 allograft, which showed immune rejection after 130 days. Allografts from the MMF-IDDS-implanted group were transparent throughout the entire observation period. The incidence of allograft rejection was 100% in the control and MMF eye drop groups, respectively. The rejected allografts were much more edematous and more heavily infiltrated with leukocytes than the nonrejected allografts. MMF-IDDS was tolerated well in the anterior chamber, even with 3 MMF-IDDS implanted in the anterior chamber at 1 time.
Conclusions:
MMF-IDDS was able to prolong high-risk allograft survival time and significantly inhibited corneal immune rejection in the rabbit model of penetrating keratoplasty. The device could safely be implanted in the anterior chamber without adverse effects.
Introduction
Corneal allograft survival depends on local or systemic immunosuppression for a prolonged, if not indefinite, period. 2 Topical and systemic corticosteroids used for both prophylaxis and the treatment of rejection episodes have not been successful in high-risk patients. Clinically, cyclosporin A (CsA) is most commonly used, but it cannot inhibit corneal neovascular proliferation.
Mycophenolate mofetil (MMF), as a very promising immunoregulating substance, is the morpholinoethyl ester of mycophenolic acid (MPA), and it shows rapid hydrolysis to MPA in vivo. 3 MPA prevents the replication of T- and B-lymphocytes by inhibiting the de novo pathway of purine synthesis. 4 MMF has been successfully used in the treatment of high-risk immune rejection after corneal transplantation.5–10 The only available formulations are administered through the oral route. 11 However, oral administration of MMF can cause various side effects. It was reported that about 18% of patients receiving MMF orally had to stop medication due to serious side effects. 12 Furthermore, the drug concentrations in ocular tissues were very low after oral administration due to the presence of the blood–ocular barrier. All factors mentioned above limit the satisfactory application of MMF in ophthalmology.
The intraocular implantable drug delivery system (IDDS) can overcome the blood–aqueous barrier and maintain a stable drug concentration in the aqueous humor. In this study, we formulated MMF in biodegradable poly-lactic-co-glycolic acid (PLGA) as a sort of MMF intraocular IDDS, and implanted the MMF-IDDS into the anterior chamber to investigate its immunosuppressive activity in the rabbit model of high-risk penetrating keratoplasty. The biocompatibility after implantation in the anterior chamber was also evaluated.
Methods
Chemical reagents
MMF and MPA were kindly provided by North China Pharmaceutical Group New Drug Research and Development Co., Ltd. PLGA (Wη 35000, lactide/glycolide ratio, 50/50) was purchased from the Chengdu Institute of Organic Chemistry, Chinese Academy of Sciences. Soya lecithin was bought for injections from Shanghai Aikang Fine Chemicals Co., Ltd. Pluronic F68 was kindly provided by Nanjing WELL Chemical Corporation, Ltd. Ethylene oxide, triethylamine, sodium dihydrogen phosphate, phosphoric acid, and hydrochloric acid were of analytical grade. The methanol was high-performance liquid chromatography (HPLC) grade.
Animals
Male and female New Zealand albino rabbits were obtained from the Shandong Academy of Agricultural Sciences, China [License No : SCXK (Lu) 20040013]. The experimental animals weighed between 2 and 2.5 kg, and were individually housed in an air-conditioned and light-controlled room at 25°C±2°C and at 70%±5% relative humidity. They were given a standard pellet and were provided with water ad libitum. All animals were healthy and free of clinically observable ocular abnormalities. The local ethics committees for animal experimentation approved all experiments.
Fabrication of the MMF-IDDS
PLGA was used in the fabrication of the implant, which contained 50% w/w of MMF. The fabrication procedure was performed as described previously,13–16 with some modifications. Briefly, 125 mg PLGA was dissolved in 2 mL 1,4-dioxane, and then the 125 mg MMF was added and dissolved in the PLGA solution. The resultant solution was lyophilized (model DF-1CE; Detianyou Instruments) to obtain a homogeneous cake. The cake was then fabricated into an implant on a hot plate (Model DB-1; Guohua Instruments) at a temperature ranging from 60°C to 70°C. The implant weighed 2.0 mg and was 0.7 mm long and 2.0 mm in diameter. Likewise, CsA-IDDS containing 1.0 mg of CsA and 1.0 mg of PLGA was prepared in a similar fashion to be used as a positive control in this article. The final formulation of MMF-IDDS and CsA-IDDS was sterilized by a STERRAD® sterilizer.
Morphological and topographical characterization of the implants
Implants were observed and photographed with a JSM-840 scanning electron microscope (Jeol). The implants were deposited on a glass disk that had been applied on a metallic stub. Before the scanning electron microscopy (SEM) analysis, the samples were metallized under an argon atmosphere with a 10-nm-thick gold palladium sheet (EMITECH-K550 Sputter Coater).
In vivo release of MMF-IDDS
The right eyes of 6 rabbits (IDDS implanted eyes) were used for pharmacokinetic analysis. IDDS containing 1.0 mg MMF were surgically implanted into the right eyes of rabbits according to a previously described method. 13 Briefly, general anesthesia was achieved by injecting ketamine (25 mg/kg) and chlorpromazine (25 mg/kg) intramuscularly. Topical anesthesia was achieved with the administration of 1 drop of proparacaine ophthalmic solution to the eye; then, the eye was held steady with clamping forceps. A 1.8-mm corneal tunnel was created at the superotemporal limbus using a disposable metal keratome, through which the MMF-IDDS was implanted into the anterior chamber. All eyes received a 0.2-mL subconjunctival injection of 40 mg/mL tobramycin solution immediately after surgery to prevent infection, and were then given a 0.3% ofloxacin eye ointment at the end of the procedure to be administered once a day for 3 consecutive days thereafter.
On days 1, 3, and 7 and weeks 2, 4, 6, and 8 after MMF-DDS was implanted, rabbits were anesthetized, and then 100 μL of aqueous humor was aspirated from the anterior chamber using a 29-gauge needle. 17 The aqueous humor samples were stored at−80°C. For analysis, each sample was mixed with 40 μL 1 M HCl and 140 μL methanol, and then centrifuged. The supernatant was analyzed by HPLC.
Quantitative determination of MMF and MPA
The quantitative determination of MMF and MPA was performed on a HPLC system 18 composed of a G1314A UV Detector (detection at a maximum of 214 nm) and an L-6200 Intelligent Pump (Merck Hitachi). Reversed phase columns Agilent C18 (150 mm×4.60 mm, 5 μm; Agilent) were used for separations. The eluent for the lipophilic prodrug MMF consisted of 68% methanol and 32% 0.02 M phosphate buffer (containing 0.1% triethylamine, adjusting the pH to 4.0 with phosphoric acid 85%), whereas the eluent for the less lipophilic MPA consisted of 53% methanol and 47% 0.02 M phosphate buffer (containing 0.1% triethylamine, adjusting the pH to 4.0 by phosphoric acid 85%). The flow rate was kept constant at 1.0 mL/min. The detection was performed at 50°C.
Preparation of the MMF ophthalmic suspension
The 1% MMF ophthalmic suspension (SUS) was prepared with soya lecithin (0.5%) and F68 (1%). A high concentration of F68 was necessary to stabilize the SUS. The preparation procedure was as follows: F68 was completely dissolved in 30 mL water. The soya lecithin and MMF were combined in a clean, dry round-bottomed flask and were dissolved in 50 mL ethylether. The ethylether was then removed using a rotary evaporator (Huxi RE52-3) under reduced pressure, and final trace organic solvents were removed under vacuum overnight. The deposited lipid film was hydrated with F68 solution at 55°C by rotation at 60 r/min for 1 h. Sonication for 10 min at 55°C was performed to obtain coarse presuspensions. These presuspensions were homogenized using a piston-gap high-pressure homogenizer (NS1001L) at 500 bar and 15 cycles. Then, the pH was adjusted to be in the range of 5.9–6.1(MODEL 828; Orion), and the osmotic pressure was measured and was ensured to be in the range of 280–330 mOsmol/kg (STY-1E Osmometer).
Corneal transplantation and immunosuppression
Penetrating keratoplasty
Neovascularization was induced in the right cornea of each rabbit by placing a 5-0 silk suture into each of the corneal quadrants. Slit-lamp biomicroscopy was performed 3 times a week before the sutures were removed. The sutures were removed under topical anesthesia 2 weeks later when superficial vessels had grown at least 4 mm into the cornea in 3 or more of the quadrants.
Two days after removing the sutures, the penetrating keratoplasty was performed as previously described. 13 Briefly, general anesthesia was achieved by injecting ketamine (25 mg/kg) and chlorpromazine (25 mg/kg) intramuscularly. The eyes of the donor rabbits were sterilized, and a 7.5-mm punch was used to produce a central corneal button graft. The recipient corneas were prepared similarly but with a 7.0-mm biopsy punch. The donor grafts were joined with the recipient corneas using a 10-0 monofilament nylon suture (Alcon Laboratories). An MMF-IDDS or CsA-IDDS was implanted into the anterior chamber at the end of the surgery, and the anterior chamber was reconstructed using a balanced sodium solution. Heparin (1,000 U/mL) was applied topically to prevent aqueous clot formation in the anterior chamber during the surgery. All grafted eyes received a 0.2-mL subconjunctival injection of 40-mg/mL tobramycin solution immediately after surgery to prevent infection, and were then given a 0.3% ofloxacin eye ointment at the end of the procedure to be administered once a day for 3 consecutive days thereafter. The sutures were removed immediately when loosed.
Clinical evaluation
Two investigators examined the corneal allografts by slit-lamp microscopy each day for the first 3 weeks and once a week thereafter. A rejection index (RI), on a scale of 0 to 12, was calculated, which was based on the combined scores of 3 allograft indicators: clarity, edema, and neovascularization, each of which was scored on a scale of 0 to 4. The scoring system for clarity was as follows: 0, clear cornea; 1, slight haze; 2, increased haze but anterior chamber structures still clear; 3, advanced haze with difficult view of the anterior chamber; 4, opaque cornea without view of the anterior chamber. The scoring system for edema was as follows: 0, no stromal or epithelial edema; 1, slight stromal thickness; 2, diffuse stromal edema; 3, diffuse stromal edema with microcystic edema of the epithelium; 4, bullous keratopathy. The scoring system for neovascularization was as follows: 0, no vascularization at the graft–host junction (GHJ); 1, vascularization at the GHJ in 1 quadrant only; 2, vascularization at the GHJ in 2 quadrants only; 3, vascularization at the GHJ in 3 quadrants only; 4, vascularization at the GHJ in all 4 quadrants.
Histopathological examination
Eight grafts chosen from the 4 groups were detected using standard histological methods. The allografts in 4 groups were collected and fixed in 10% formol, and then embedded in paraffin. Hematoxylin–eosin (HE) staining was performed.
Biocompatibility of MMF-IDDS in the anterior chamber
In this experiment, 1 or 3 MMF-IDDS pellets were implanted into the anterior chamber of New Zealand white rabbits to study the biocompatibility. Eighteen rabbits were randomly distributed to 3 groups, with 6 in each group. The left eye was designated as the experimental eye. The groups were the group implanted with 1 MMF-IDDS in the anterior chamber of each eye; the group implanted with 3 MMF-IDDS in the anterior chamber of each eye; and the surgical group, which was subjected to a sham surgical procedure.
Rabbits were examined on days 1 and 3 and weeks 1, 2, 3, 4, 6, 8, and 9 after implantation. A slit-lamp experiment was performed to examine the IDDS–tissue interaction in the anterior chamber. The ocular grading method was used for biomicroscopic examinations, which was described in detailed by Yang and Li. 19 After the implanted IDDS had completely degraded, a 2-week recovery period was set. Rabbits were then euthanized, and the implanted eyes were harvested to histopathological examination. Three eyes from each group were fixed in a 10% formol solution for at least 24 h and dehydrated with gradient alcohol; then, the eyeballs were prepared for HE using routine methods and analyzed with light microscopy to examine the cornea, the iris and the retina. The presence of neutrophils, lymphocytes, macrophages, fibroblasts, and giant cells was regarded as evidence of the tissue response. Every sample was treated simultaneously to reduce variation among fixation procedures.
The corneas of the other 3 eyes in each group were separated and fixed in glutaraldehyde 2.5% in 0.1 M sodium cacodylate buffer and prepared for SEM. The corneas were bisected and postfixed in osmium tetroxide 2% for 2 h. For SEM, samples were prepared using critical point drying. The tissue was glued to stubs, sputter-coated with gold palladium, and viewed with a JSM-840 scanning electron microscope (Jeol).
Data analysis
The MPA concentration in the humor and median survival time of grafts were expressed as mean±standard deviation. Statistical analysis was performed using the two-tailed Student's t-test. The survival time was compared between the various groups by means of one-way ANOVA.
Results
Morphological and topographical characterization of implants
All MMF-DDS obtained were round, uniform, off-white color mini-tablets with smooth surfaces, as determined through macroscopic observation. SEM revealed that lots of micropores were found on the surface of the implants (see Fig. 1).
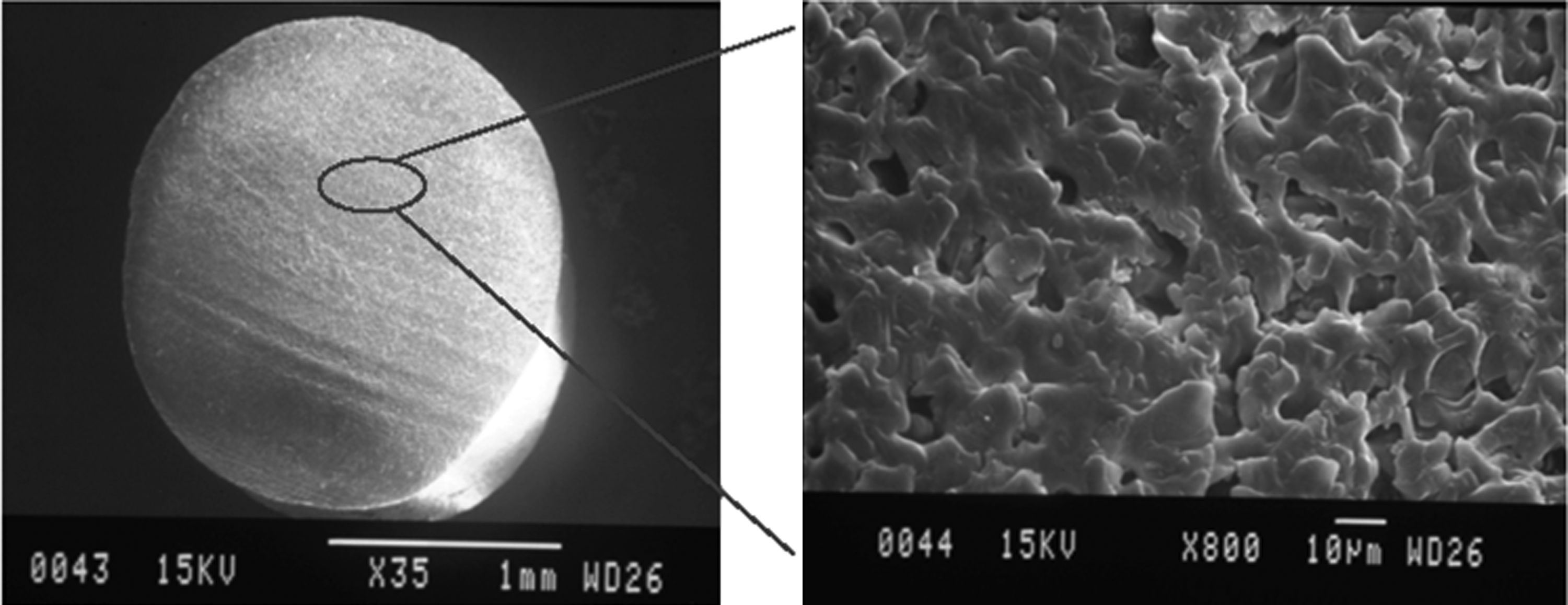
Scanning electron microscopy micrographs of MMF-DDS. Lots of micropores were found on the surface of the implants. MMF, mycophenolate mofetil.
In vivo release characteristics of implants
In vivo release was determined by measuring the drug concentration in the aqueous humor. There was no MMF detected in aqueous humor, because MMF was completely degraded during its release. Figure 2 shows the profile of in vivo MPA release from the MMF-IDDS. The MPA concentration in the humor ranged from 0.247 to 4.376 μg/mL over the course of 56 days.
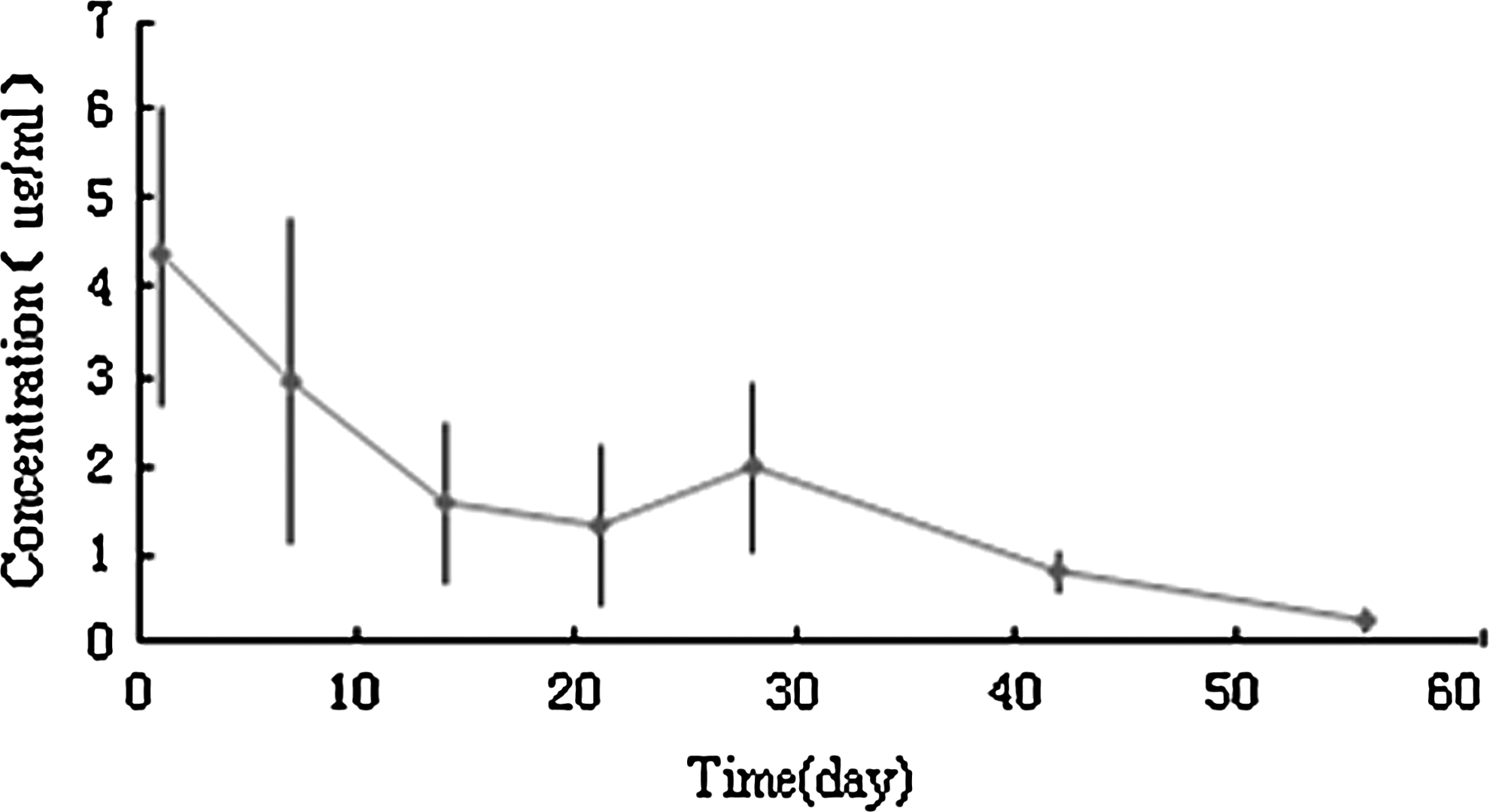
The MPA concentrations in aqueous humor of MMF-DDS (n=6). The MPA concentration in the humor ranged from 0.247 to 4.376 μg/mL over the course of 56 days. MPA, mycophenolic acid.
Superiority of MMF-IDDS over MMF eye drops for preventing corneal allograft rejection
Clinical observation
After surgery, mild corneal edema was seen in all animals but disappeared 3 days after transplantation. In all treatment groups, enlarged blood vessels were seen around the graft. The details of each group are described as follows.
Control group: The graft was transparent, and mild edema was observed, but the vessels in the recipient cornea were engorged at day 2 after transplantation. Seven days after surgery, some of these vessels began to enter the grafts in 1–2 quadrants with a length of 0.5–1 mm. The grafts were mildly opaque and edematous (grade 0–1). The vessels in the recipient cornea were still engorged. About 2 weeks after transplantation, the opacity of the grafts worsened to grade 2–3, while edema worsened to grade 2–4. The vessels in the recipient corneas began to enter the grafts in quadrants 3–4 with a length of 1–2 mm. All of these characteristics suggested that the graft had been rejected. Three weeks after transplantation, the opacity of the grafts worsened to grade 3–4, while edema worsened to grade 2–3. The vessels in the grafts were 1–2 mm in length. All of these characteristics predicted that the graft would be completely rejected (see Fig. 3).
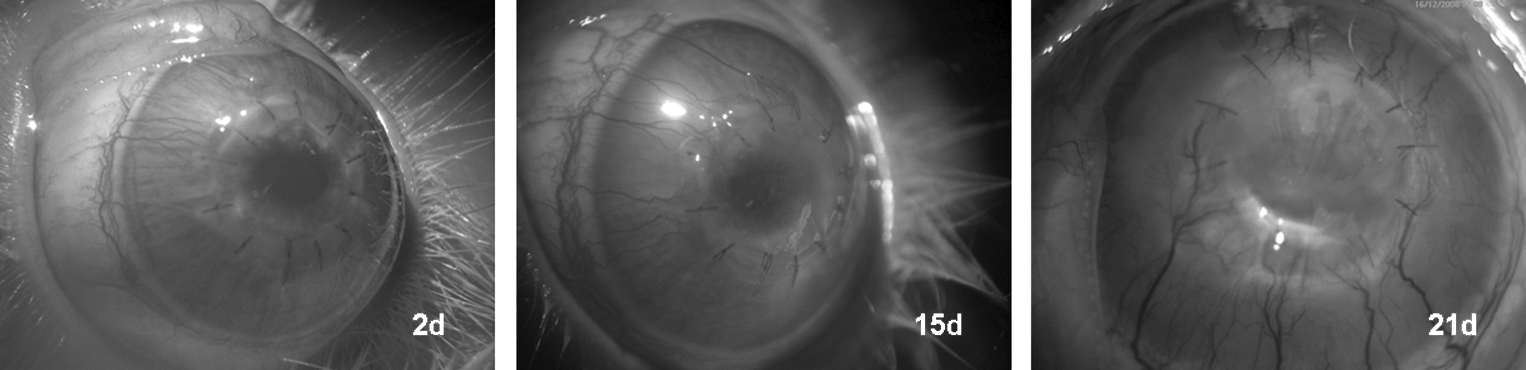
The rejected graft appears completely vascularized on day 15 and 21 in the control group.
MMF ophthalmic SUS group: The graft was transparent, with mild edema observed. The vessels in the recipient cornea were a little engorged, although the magnitude of this engorgement was less than in the control group at day 2 after transplantation. Seven days after surgery, the graft was still transparent, and the vessels in the recipient cornea were still a little engorged, but no vessels in the recipient cornea had entered into the grafts. Two weeks after transplantation, the opacity of the grafts worsened to grade 0–1, with edema of grade 0–1. Some vessels in several rabbits began to enter the grafts, in 1–2 quadrants with a length of 0.5–1 mm. About 4 weeks after transplantation, the opacity of the grafts worsened to grade 2–3, with edema grade 2–3. The vessels in the recipient cornea began to enter the grafts with a length of 2–3 mm. These were signs of graft rejection.
MMF-IDDS and CsA-IDDS groups: In the CsA-IDDS group, the graft was transparent and mild edema was observed, but the vessels in the recipient cornea were a little engorged at day 2 after transplantation. During the following observation, all grafts remained clear within 150 days. Opacification and neovascularization of 1 graft was seen at day 130, which was a sign of rejection. As in the MMF-IDDS group, the cornea was also a little engorged at day 2 after transplantation, and then the cornea engorged was recovered gradually with the vessels disappeared gradually, and the grafts were clear for more than 150 days. The IDDS gradually biodegraded and was no longer visible by slit-lamp microscopy (see Fig. 4).
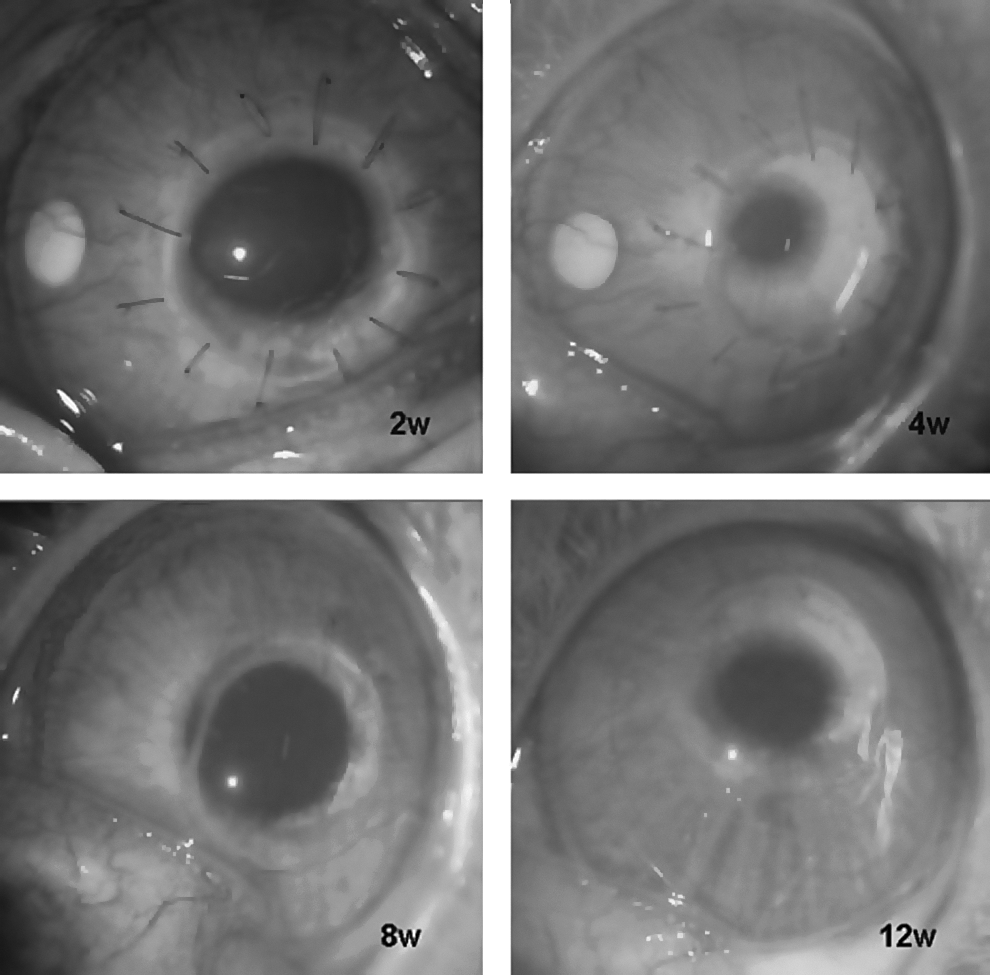
The corneal graft remains clear on weeks 2, 4, 8, and 12 in the MMF-IDDS group. The IDDS gradually becomes small until it completely dissolves. IDDS, implantable drug delivery system.
Allografts with RIs of 6 or greater were considered as rejected. In the control groups, opacification peaked within 22 days, with a large amount of neovascularization invading the grafts in most quadrants. The median survival time of these grafts was 18.7±3.0 days. In the MMF group treated with eye drops, the graft remained clear for between 31 and 40 days with a median survival time of 37.5±6.2 days after PK, with less neovasculature moving into the grafts. In the CsA-IDDS group, there was only 1 graft rejected at day 130 after the operation. In contrast, none of the animals in the MMF-IDDS group were rejected throughout the entire 150 days of observation.
As for histopathological examination of the grafts, in the control group, severe infiltration of inflammatory cells occurred and the blood vessels were observed to have infiltrated into the graft (Fig. 5A). There was mild neovascularization and inflammatory cell infiltration when allograft rejection occurred in the MMF/drops group; these effects were much milder in corneas rejected in the CsA-IDDS group. In the MMF-IDDS group, all the allografts had normal corneal thickness, fewer infiltrating cells, and no neovascularization throughout the observation period (Fig. 5B).
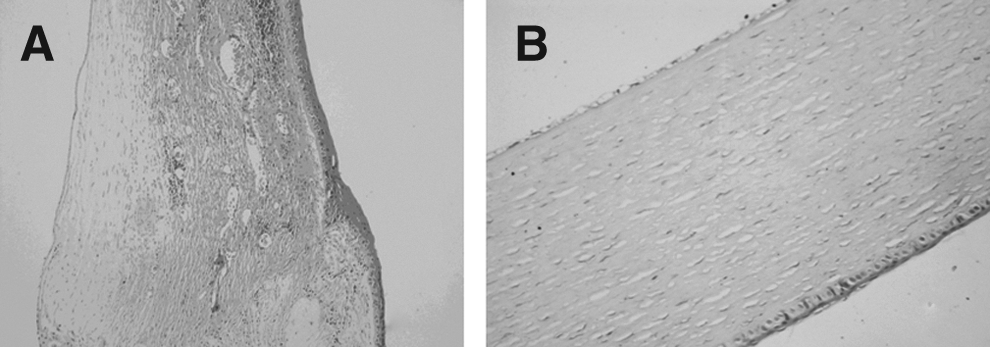
Histopathological examinations of grafts in control and MMF-IDDS group
Biocompatibility of MMF-IDDS in the anterior chamber
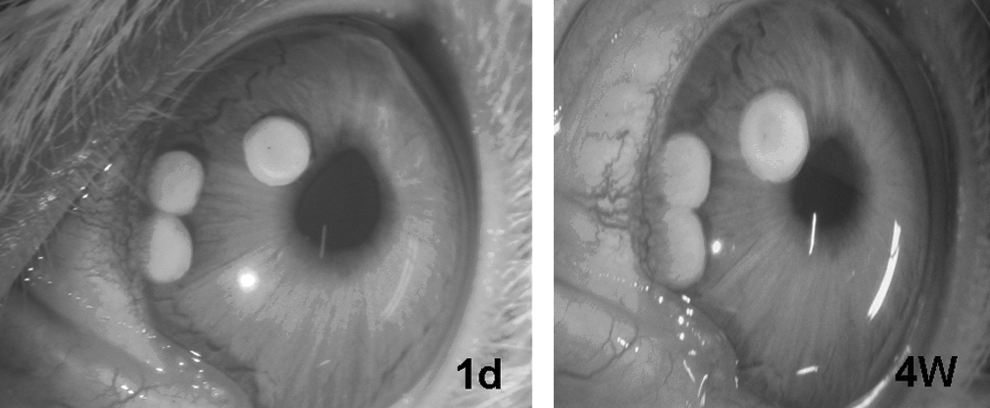
The general performance of the rabbits after implantation was normal in all 3 groups. As to the MMF-IDDS in the anterior chamber, there was no obvious difference between rabbits implanted with 1 versus 3 MMF-IDDS in the first week after implantation. The surface appeared a little fluffy under the slit lamp after 2 weeks, and the structure of the IDDS was slightly loose after 4 weeks. Six weeks after implantation, degradation was obvious, and the IDDS appeared as a lamellar structure. Only minimal residue was observed at 8 weeks (see Fig. 6). The degradation process was similar in groups implanted with 1 or 3 MMF-IDDS devices (see Fig. 7). The time required for degradation was 56.33±3.44 and 58.67±2.73 days in the groups implanted with 1 and 3 MMF-IDDS devices, respectively.

The degradation of 1 MMF-IDDS in the anterior chamber. The surface appeared a little fluffy under the slit lamp after 2 weeks, and the structure of the IDDS was slightly loose after 4 weeks. Six weeks after implantation, degradation was obvious, and the IDDS appeared as a lamellar structure. Only minimal residue was observed at 8 weeks.
The biocompatibility of 3 MMF-IDDS in the anterior chamber. The MMF-IDDS had good biocompatibility in the anterior chamber.
Clinical observations are discussed in the following sections.
Cornea
There was no corneal edema observed throughout the experiment period of the 3 groups. In all 3 groups, the clarity of the cornea increased throughout the experimental period. No keratic precipitate was found in any eye throughout the experiment.
Anterior chamber
In terms of the observation of aqueous flare in the anterior chamber at day 1 after implantation, there were 4 eyes scored as 1 in the control group, 1 eye scored as 2 and 5 eyes scored as 1 in the 1MMF-IDDS group, and 4 eyes scored as 2 and 2 eyes scored as 1 in the 3MMF-IDDS group. The extent of aqueous flare had decreased upon subsequent observation. There were 3 eyes scored as 1 in the control group, 4 eyes scored as 1 in the 1MMF-IDDS group, and 2 eyes scored as 2 and 3 eyes scored as 1 in the 3MMF-IDDS group, respectively, at day 3 after implantation. At 1 week after implantation, all of the eyes with aqueous flare recovered well and no aqueous flare was observed in any of the 3 groups.
With respect to aqueous cells in the anterior chamber, 3 eyes were scored as 1 in the control group, 1 eye was scored as 2, and 4 eyes were scored as 1 in the 1MMF-IDDS group on day 1 after implantation. Four eyes were scored as 2 and 2 eyes were scored as 1 in the 3MMF-IDDS group, respectively, on day 1 after implantation. As in aqueous flare, the density of aqueous cells was reduced upon subsequent observation. There were 2 eyes scored as 1 in the control group, 3 eyes scored as 1 in the 1MMF-IDDS group, and 2 eyes scored as 2 and 2 eyes scored as 1 in the 3MMF-IDDS group, respectively, on day 3 after implantation. All of the eyes with aqueous cells had recovered completely at 1 week after implantation.
There were only 1, 2, and 3 eyes scored as 1 in terms of fibrin exudate in the control, 1 and 3 MMF-IDDS groups, respectively, on day 1 after implantation. The fibrin exudate disappeared completely at 3–7 days after implantation.
The iris and lens were normal throughout the entire observation period for all 3 groups.
Histological analysis of the eyes is presented in Fig. 8. The integrity of the cornea of a rabbit eye from each of the 3 groups can be observed. Neither cell infiltration to the cornea nor alteration of the endothelial cell layer was found. All eyes in all groups had a clean vitreous cavity, explicit retinal structure, and a compact sclera. The structure of the chamber angle and iris was normal.
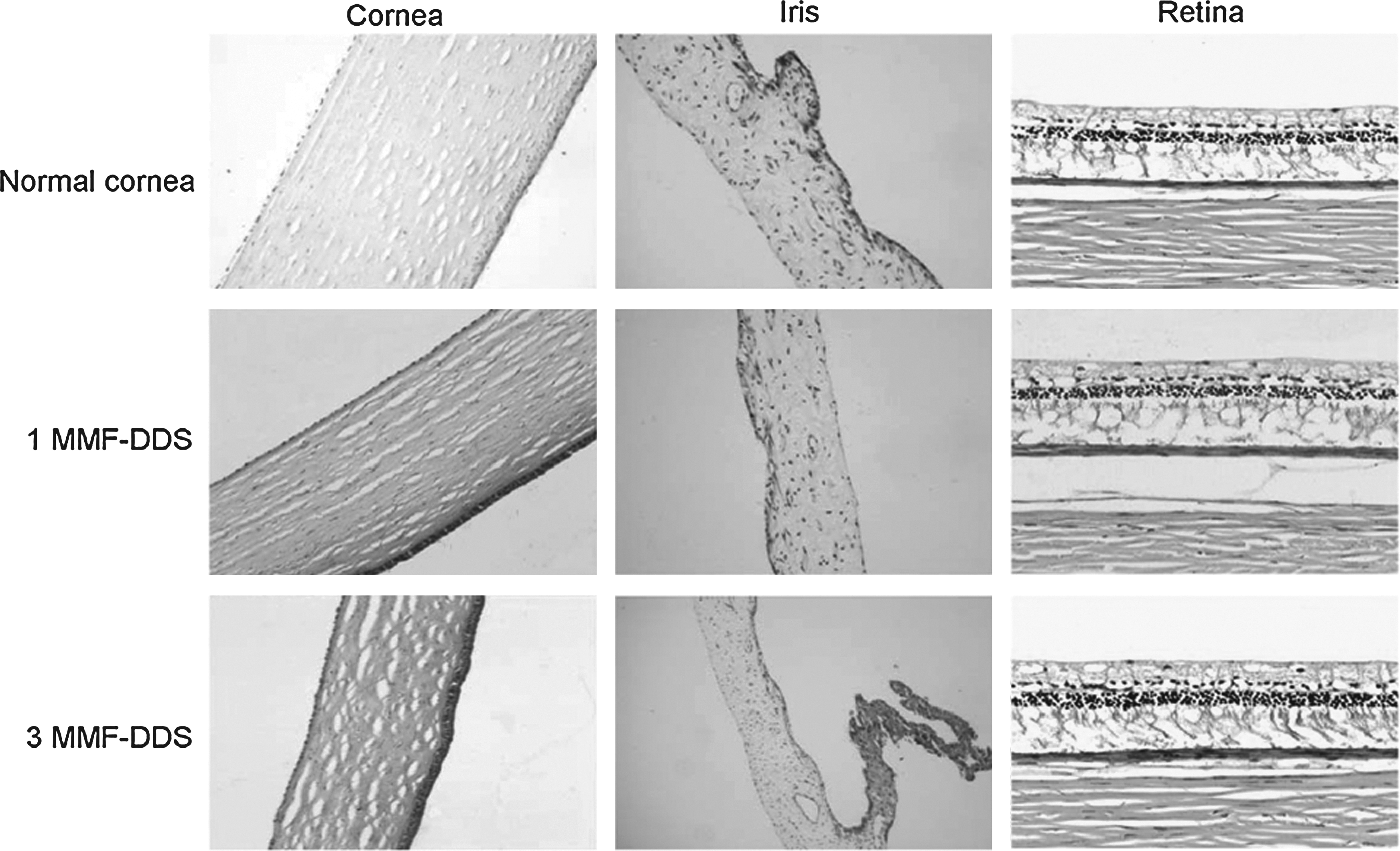
Representative histopathologic images of rabbit eyes at the end of the observation period (×200). The integrity of the cornea from each of the 3 groups can be observed. Neither cell infiltration to the cornea nor alteration of the endothelial cell layer was found. A clean vitreous cavity, explicit retinal structure, and a compact sclera were also observed, and the structure of the chamber angle and iris were normal.
The endothelial cells of the cornea were observed by electron microscopy (see Fig. 9) at the end of the observation period. The results from electron microscopy showed that all eyes in all 3 groups had well-preserved hexagonal endothelial cell mosaics and normal microvilli on their endothelial cell surfaces; no edema or necrosis was found.
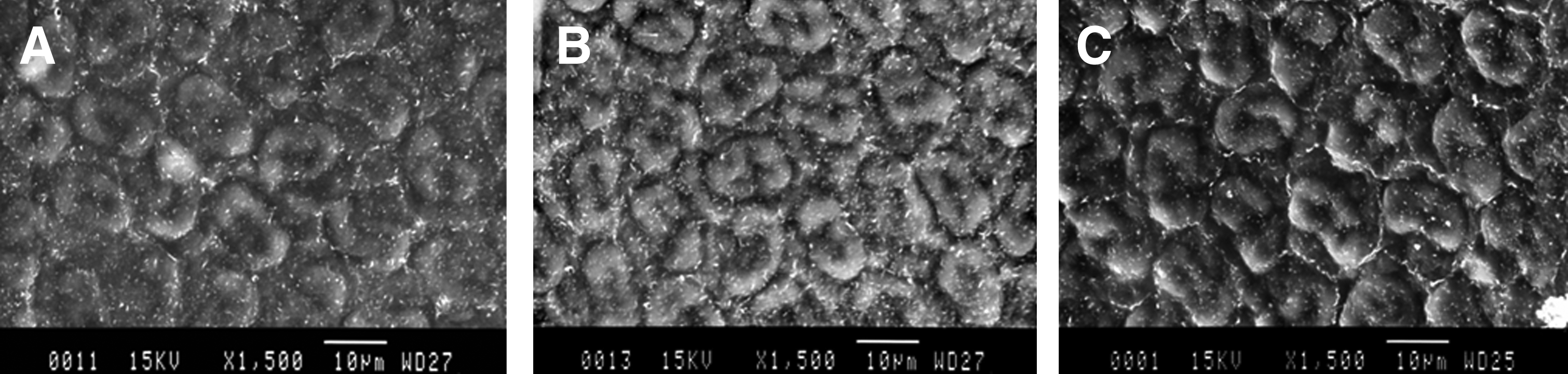
Scanning electron micrographs of rabbit corneal endothelial cells at the end of the observation period
Discussion
Intracameral implantable delivery of immunosuppressive drug is effective in the prevention of corneal allograft rejection in normal-risk and high-risk recipients, and in delaying the incidence of rejection in high-risk recipients.13,14,20 This study demonstrated prominent prolongation of corneal allograft survival in the MMF-IDDS group and the MMF group treated with drops as compared with the untreated group. Thus, acute rejection was suppressed or delayed in the former groups. The corneal grafts in the MMF-IDDS group remained clear and were not subject to acute rejection throughout the entire study period. However, allograft acute rejection was delayed at the beginning but not suppressed at the end in the MMF group treated with drops. As determined by changes in the aqueous MPA concentration, MMF-IDDS devices were able to maintain sustained release of the drug into the aqueous humor to achieve longer graft survival. Therefore, we can conclude that the aqueous concentration of MPA is extremely essential in preventing high-risk corneal allograft rejection. Corneal allograft rejection is caused by delayed hypersensitivity. Acute rejection typically occurred within 1–3 months. Clinically, 65% of rejection is endothelium-based and often occurs at a later time point. 13 Due to the corneal barrier, topical MMF can reach high concentrations on the ocular surface and in the upper layer of the cornea but also fails to penetrate the inner layer and aqueous humor. Therefore, MMF drops failed to prevent the occurrence of graft rejection.
CsA-IDDS was researched and developed by the Shandong Eye Institute, and it was proven that CsA-IDDS placed in the anterior chamber can significantly prolong the survival of grafts.14,20 The drug was successfully approved by the Food and Drug Administration of China to perform clinical trials (clinical trial no. 2006L02840). The CsA-IDDS group was set as the positive control in this study. In the CsA-IDDS group, all grafts remained clear within 150 days except for 1 graft, in which opacification and neovascularization were seen on day 130. Our results showed that MMF-IDDS is just as effective as CsA-IDDS in preventing acute rejection. Birnbaum et al. determined that the frequency of clear graft survival after 1 and 3 years was 92% and 77% in the CsA group and 96% and 87% in the MMF group, respectively, as demonstrated by the long-term results of 417 high-risk keratoplasties with systemic immunosuppression. 5 Notably, the MMF-treated patients showed fewer side effects than the CsA-treated patients. 5 As to the implants, the MMF implant also has an advantage over the CsA implant. The CsA implant in this clinical trial, which was developed by our research team, had a flaw of slow degradation after the complete release of CsA. The matrix of the implant was still in the anterior chamber and needed 3–4 months to degrade completely. The MMF implant covered this flaw. It might be explained that the MPA, an acidic molecule, could speed up the degradation of PLGA, and the mechanism is under investigation in our group.
Statistically, there was a significant difference in the median survival time of the grafts between the control and eye drops groups (P=0.000). Both the CsA-IDDS and MMF-IDDS groups displayed significant differences in median survival time compared with the control and eye drops groups (P<0.001). There was a statistically significant difference between the CsA-IDDS and MMF-IDDS groups (P=0.000).
To investigate the biocompatibility of MMF-IDDS in the anterior chamber, aqueous cells are a reliable indicator of inflammation in the aqueous humor. 21 The density of aqueous cells reflects the severity of inflammation. In this study, on days 1 to day 3 after implantation, sparse aqueous cells could be observed in the control, 1MMF-IDDS, and 3MMF-IDDS eyes, representing a weak inflammatory response. No aqueous cells were observed upon subsequent observation, which indicates that recovery was successful. Therefore, the results suggest that implanting MMF-IDDS, whether 1 or 3 in the anterior chamber, does not induce a significant inflammatory reaction. Aqueous flare is caused by increased protein concentration in the anterior chamber, which reflects the blood–aqueous barrier's integrity. Some factors, such as inflammation, trauma, and intraocular pressure, can damage the blood–aqueous barrier, at which point plasma proteins penetrate the anterior chamber, which in turn causes aqueous flare. Therefore, aqueous flare serves as an indicator of the integrity of the blood–aqueous barrier. The results of the biocompatibility experiment also suggest that MMF-IDDS, whether 1 or 3 in the anterior chamber, had little effect on the integrity of the blood–aqueous barrier.
It has been reported that cellular hexagonality is a sensitive indicator of endothelial damage or instability and may be valuable in qualitative observations of cell appearance.22,23 In this biocompatibility study, there was no difference in the corneal endothelium when comparing the 1 or 3MMF-IDDS group to the control group. Therefore, MMF-IDDS, whether 1 or 3 in the anterior chamber, has no negative impact on the corneal endothelium. MMF-IDDS devices pose no danger to the corneal endothelium when implanted into the anterior chamber.
Although there was no direct comparison between the MMF-IDDS and systemic MMF in this text, we could conclude safely that MMF-IDDS would decrease the dosage dramatically. As we know, systemic MMF was scheduled for 6 to 12 months at a daily dose of 2 g in preventing immune rejection in ophthalmology.5,24 The total dosage of MMF was about 360 to 720 g during that scheduled time, while about 3 to 6 mg MMF in MMF-IDDS was enough.
In conclusion, MMF-IDDS effectively prevented immune rejection in rabbit eyes with high-risk keratoplasty over the long-term. The biocompatibility of the device was verified. The device holds potential as a tool to prolong corneal allograft survival in ophthalmology.
Footnotes
Acknowledgments
This research work is supported by the Taishan Scholar Program, Shandong Province of China (project no. ts20081148).
Author Disclosure Statement
We have no proprietary or commercial interest in any of the mentioned drugs or companies.