
Abstract
Abstract
Purpose:
The purpose of the present study was to elucidate the effects of oral administration of black currant anthocyanins (BCACs) on intraocular pressure (IOP) in both healthy subjects and patients with glaucoma.
Methods:
(1) A placebo-controlled, double-masked, crossover study (n=12) was conducted, during which BCACs (50 mg/day) or placebos were orally administered to 12 healthy subjects once daily for 4 weeks. (2) A total of 21 glaucoma patients (BCACs, n=12; placebo, n=9) treated with a single antiglaucoma medication who had participated in a previous study (a randomized, double-masked, placebo-controlled trial, Ophthalmologica 2012) were selected and analyzed. Systemic blood pressure, pulse rates, IOP, and Humphrey visual-field mean deviation (MD) (program 30-2, SITA standard) were evaluated.
Results:
(1) A statistically significant decrease in the mean IOP was observed at 2 weeks (P=0.002, paired t-test) and 4 weeks (P=0.039, paired t-test) from the baseline in BCAC-treated healthy subjects. This decrease, however, was not observed in the placebo group. In addition, at 2 weeks after the baseline, changes were also statistically significant between the groups (P=0.027, paired t-test). (2) Intergroup and between-group analyses revealed statistically significant decreases in mean IOP in the glaucoma patients taking BCACs (P=0.027, paired t-test; P=0.024, unpaired t-test) at 24 months after the baseline. In addition, mean changes of MD deterioration were significantly less in BCAC glaucoma patients administered with BCACs at 12 months (P=0.017, Mann–Whitney U test) and 18 months (P=0.050, Mann–Whitney U test) after the baseline. No clinically significant changes were observed in systemic blood pressure or pulse rates in either trial.
Conclusions:
Our results suggested that oral administration of BCACs may induce a beneficial decrease in IOP levels in healthy subjects as well as in patients with glaucoma.
Introduction
Elevated intraocular pressure (IOP) is generally recognized as the most important risk factor for glaucomatous optic neuropathy, and therefore lowering the IOP through antiglaucoma medication and/or surgical intervention is necessary.8–10 Since BCACs modulate ET-related metabolisms within the ciliary body as noted above, we speculated that BCACs could also affect IOP levels by changing aqueous humor production. It was therefore of great interest to determine whether systemic administration of BCACs affected IOP levels in patients with glaucoma as well as healthy subjects.
In the current study, we described the results of 2 trials. In the first, we investigated whether oral administration of BCACs can affect the IOP levels. A placebo-controlled, double-masked, crossover study was performed using healthy volunteers. In the subsequent trial, we analyzed changes of IOP and visual field deterioration in a total of 21 OAG patients received a single glaucoma medication and had participated in our previous 24-month randomized, placebo-controlled study of BCACs. 7
Subjects and Methods
A placebo-controlled, double-masked, crossover study using healthy volunteers
A placebo-controlled, double-masked, crossover study using healthy volunteers was performed at the Yagi clinic (Tokyo, Japan). The protocol of this single-center study of 12 healthy volunteers was approved by the Ethics Committee of the Aisei-Byouin Ueno Clinic and conducted in accordance with the Declaration of Helsinki.
Subjects
In a screening to determine an individual's eligibility, a medical and ocular history was obtained, and a complete ophthalmic examination, including IOP measurement by an auto-noncontact pneumotonometer, and dilated fundus evaluation were performed. From among the 79 applicants, 47 eligible volunteers met the standards in the inclusion and exclusion criteria described below. Of these, 12 subjects agreed to participate in the study after an explanation of the study's purpose, and its protocols were provided, and written informed consent was obtained from all participants during the period from April 16, 2011, through July 31, 2011 (Fig. 1).
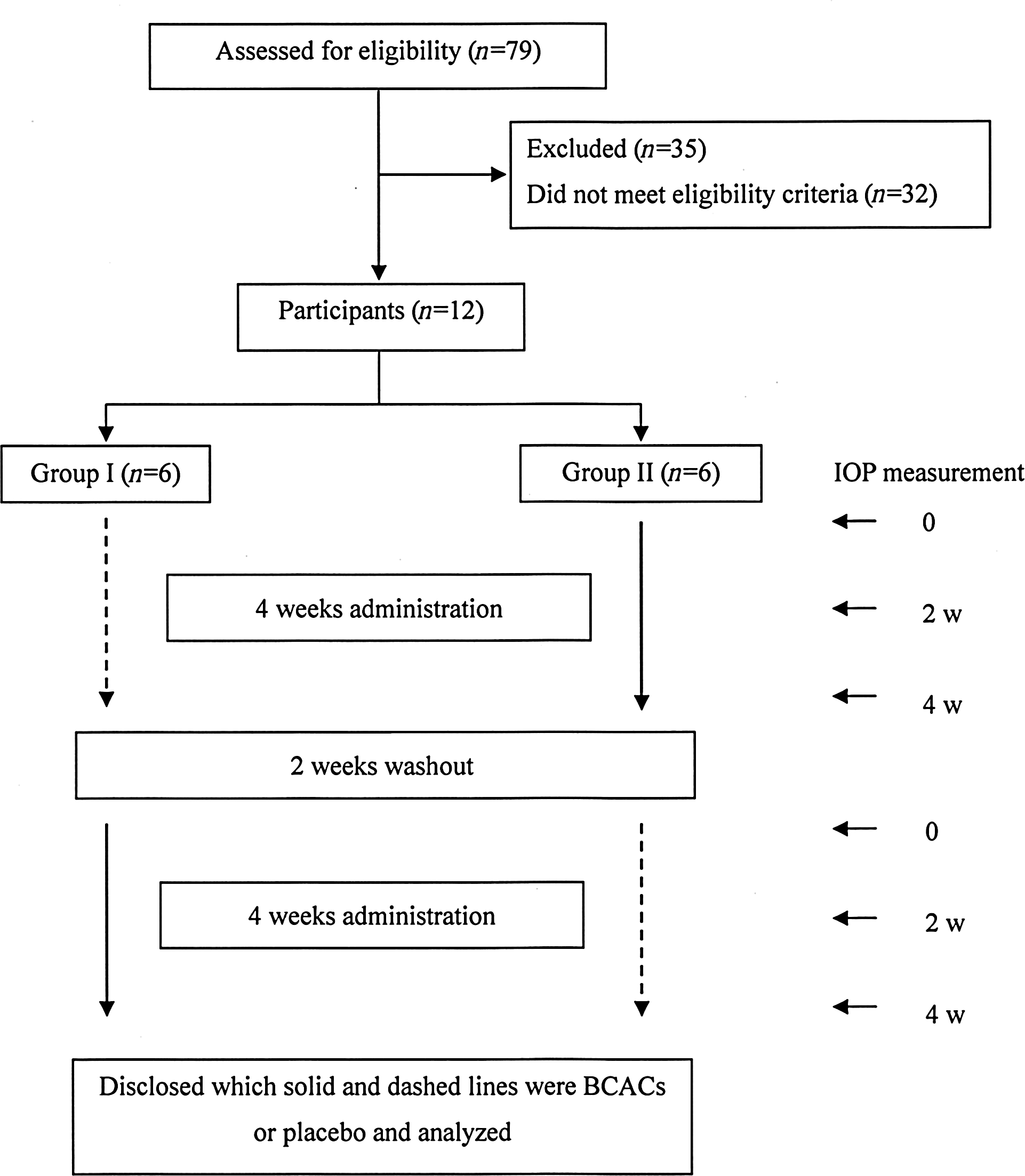
Flow chart of a placebo-controlled, double-masked, crossover study in healthy volunteers.
Inclusion and exclusion criteria
(1) No ocular pathologic condition other than minor refractive errors, with a spherical equivalent <5 diopters and baseline IOP more than 16 mmHg and less than 21 mmHg in at least one eye.
(2) No use of any medications or supplements.
(3) No history of drug or food allergies.
Study design
This study was a double-blind placebo-controlled crossover trial (Fig. 1, n=12). The supplementation and washout periods were 4 and 2 weeks, respectively. Subjects received daily doses of either BCACs (3 capsules, 50 mg/day) or placebo capsules. IOP before and after the 2 and 4 weeks of supplementation was measured by investigators or technicians unaware of the subjects' group assignments. IOP changes during the trial were analyzed, examining the left eyes of each subject. In terms of the examining eye, we decided to use data from the left eye, because IOP of the right eye from 3 subjects demonstrated more than 21 mmHg at least once during 3 consecutive analyses of subjects' screening tests. Despite these exclusions and although the focus of this study is on patients' left eyes, we have included data regarding tests of the right eyes in the Results section.
24-month randomized, placebo-controlled study of BCACs in patients with glaucoma
A randomized, double-masked, placebo-controlled single-center trial using 38 patients with OAG meeting the inclusion and exclusion criteria described below was conducted between November 1, 2006, and March 31, 2010 in the glaucoma clinic of the Department of Ophthalmology, the Sapporo Medical University Hospital. 7 The experimental protocol is briefly described below (Fig. 2).

Flow chart of a randomized, placebo-controlled, double-masked trial in glaucoma patients. The analysis of a total of 38 glaucoma patients (black currants anthocyanins [BCACs]; n=19, placebo; n=19) within large solid square is already described in previous report (ref 7). In the current study, further analysis was performed using a total of 21 patients who were treated by a single antiglaucoma medication (shown within a dotted square).
Inclusion and exclusion criteria
From among eligible 250 patients with OAG, a total of 38 patients meeting the following inclusion and exclusion criteria were enrolled in the study.
Inclusion criteria
(1) More than 24 months of treatment by antiglaucoma drops and regularly receiving IOP measurements at 1–2-month intervals and the Humphrey visual field 30-2 test (Humphrey Instruments, San Leandro, CA) at 3–6-month intervals.
(2) Early-to-moderate stages of glaucomatous optic neuropathy (MD >–12 dB) in at least one eye.
(3) Best-corrected visual acuity >0.6 at the trial baseline in at least one eye.
(4) Reliable performance on the Humphrey visual-field testing 30-2 program (fixation loss of <20%, and a false-positive or false-negative response of <33%).
Exclusion criteria
(1) Ocular diseases other than OAG and an early or mild senile cataract that would not influence the Humphrey visual field testing.
(2) No other ocular, neurological, otolaryngological, or systemic diseases affecting optic disc damage.
(3) History of cataract surgery within the previous 24 months.
(4) History of glaucoma surgery.
(5) Use of supplements.
(6) History of drug or food allergies.
Study design
This was a randomized, double-masked, placebo-controlled single-center trial, and its enrollment and follow-up were conducted between November 1, 2006, and March 31, 2010. Subjects meeting the inclusion and exclusion criteria randomly received daily doses of BCACs (2 capsules, 50 mg/day, n=19) or placebo capsules (n=19) for 24 months. Randomization was based on a computer-generated list created by a biostatistician (Y. M.), who was not involved in any other aspect of the current study. The list was disclosed after all patients completed the 24-month administration. Slit-lamp examinations and IOP measurements through a Goldmann applanation tonometer were performed during patients' monthly visits, and systemic blood pressure, visual acuity, and a Humphrey visual-field 30-2 test (SITA standard) were measured at the trial baseline and again every 6 months during the 24-month period. All examinations and measurements were carried out between ∼9 and −11 a.m. During the follow-up period, glaucoma medications were not altered. Among the 38 patients, 21 patients (BCACs, n=12; placebo, n=9) were selected to be treated by a single antiglaucoma drop (prostaglandin analogs), and other 17 patients (BCACs, n=7; placebo, n=10) treated by more than 2 antiglaucoma were excluded. Mean changes of IOP and MD deterioration in their left eyes during the 24-month trial were analyzed. We chose to analyze the left eyes of patients, because MD at baseline of right eye from one patient from the BCAC group and 2 patients from the placebo group were excluded based upon the inclusion criteria of the MD levels described above. Despite these exclusions and although the focus of this study is on patients' left eyes, we have included data regarding tests of the right eyes in the Results section.
Statistical analysis
A Shapiro–Wilk test confirmed normal distribution in all subjects' data, except MD values at baseline. Thus, during the follow-up period, differences of changes of values at each time point from trial baseline in several observational data, including systolic or diastolic blood pressure and IOP, were compared by unpaired t-test between the BCAC and placebo groups. Additionally, differences in changes at each time point of the above observational data from baseline values within each group were compared by a paired t-test. In terms of visual field MD, statistical analysis for differences between groups at each time point and inter-group differences between baseline and each time point were performed by a Mann–Whitney U test and a Wilcoxon signed
All statistical analyses were performed with MS-Excel. The significance level was set at P<0.05 for all statistical analysis.
Results
A placebo-controlled, double-masked, crossover study using healthy volunteers
Table 1 summarizes the baseline characteristics of the participants. Between the 2 groups, no significant difference was observed in age and gender, the systemic conditions, including systolic and diastolic blood pressure and pulse rates, or ocular conditions, including IOP and refractive errors. BCACs or placebos were orally administered to participants of each group for 4 weeks in a double-masked manner. IOP was measured at baseline and at 2 and 4 weeks. After 2 weeks of the washing-out, the same protocol was repeated, except those previously receiving BCACs were now given placebos, and the group originally administered with placebos received BCACs (Fig. 1). As shown in Fig. 3, statistically significant decreases in IOP were observed at 2 weeks (left eye: −1.89±1.58 mmHg, P=0.002) and 4 weeks (left eye: −1.19±1.77 mmHg, P=0.039) from the baseline in the BCACs group, but no significant changes were observed in the placebo group. In addition, the mean change of IOP at 2 weeks from the baseline was also statistically significant between groups (left eye: P=0.027). In terms of the right eye, although a few eyes were excluded due to the inclusion criteria as described in the Methods section, similar effects for IOP were observed: significant decrease in the BCAC group (at 2 weeks: −1.85±1.46 mmHg, P=0.001; at 4 weeks: −1.36±1.65 mmHg, P=0.001, paired t-test), but not in the placebo group, and significant changes between groups at 2 weeks (P=0.032, unpaired t-test) were observed.
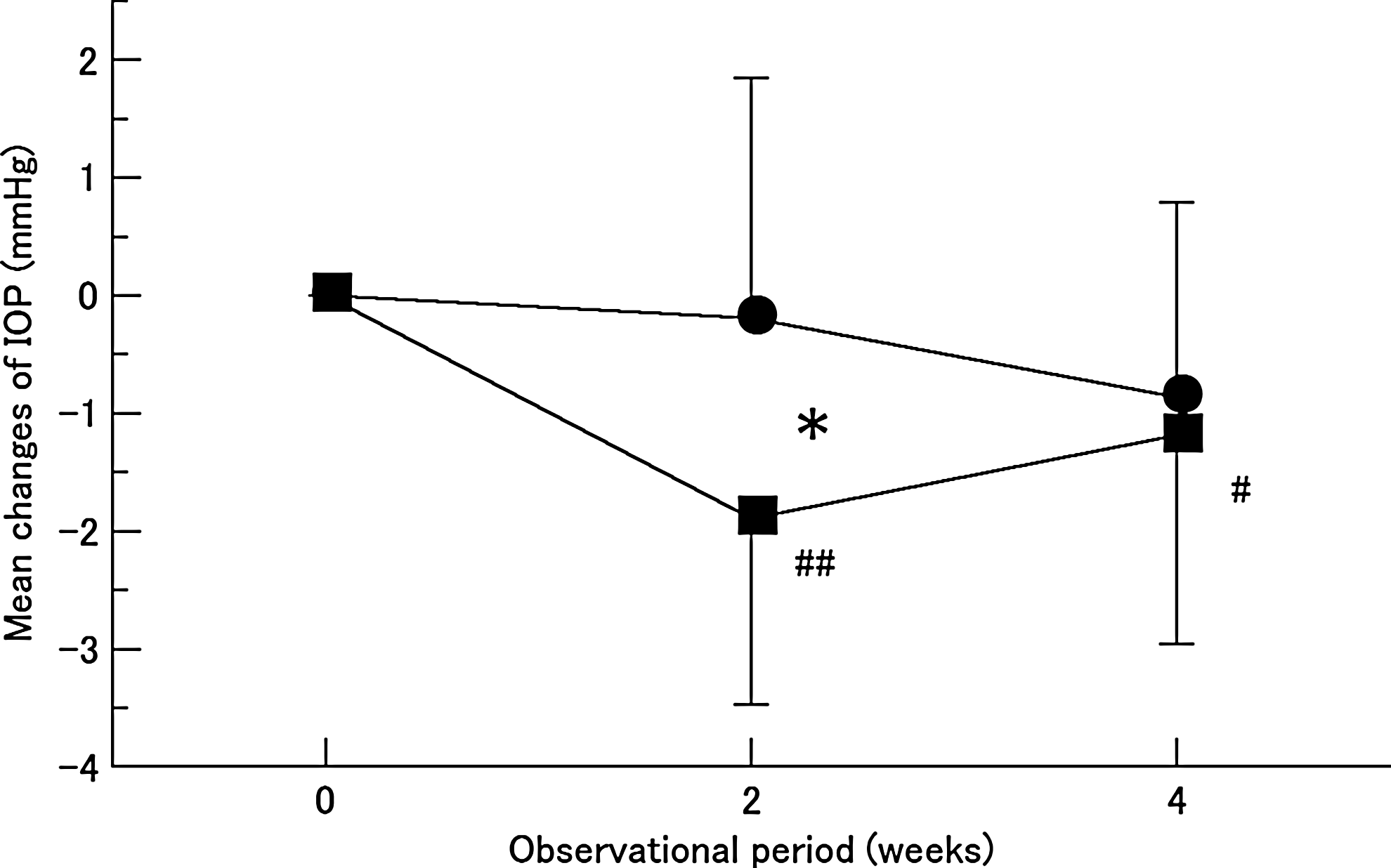
The time course changes of intraocular pressure (IOP) in a placebo-controlled, double-masked, crossover study. The differences between baseline and each trial time point (2 and 4 weeks) of IOP of the left eyes in the BCAC intake group (filled square) or placebo intake group (filled circle) were plotted. Data are expressed as mean±SD. Significant difference between groups (*P<0.05, paired t-test). Significant intergroups difference between each time point and baseline (#P<0.05, ##P<0.01, paired t-test).
P values for difference between I and II groups were calculated by Fischer-test for gender and unpaired t-test for others.
Mean±SD (all such values).
95% CI in parentheses (all such values).
CI, confidence interval.
24-month randomized, placebo-controlled study of BCACs in patients with glaucoma
The results described above suggest that BCACs may also decrease IOP in patients with glaucoma. Therefore, to determine whether BCACs may indeed be beneficial for IOP control as well as visual field deterioration, in the subsequent trial, we analyzed a total 21 patients (BCACs, n=12; placebo, n=9) who received single antiglaucoma drop of prostaglandin analogs and were selected from our previous study of the 24-month randomized, placebo-controlled study of BCACs. 7
No significant difference between newly selected groups was observed in age, gender, the systemic conditions, including systolic and diastolic blood pressure, pulse rates, or ocular conditions, including visual acuity, IOP and MD in the Humphrey visual field-testing 30-2 program at baseline (Table 2). As shown in Fig. 4, mean IOP was significantly decreased at 24 months from the baseline in the BCAC group (left eye: −0.58±0.79 mmHg, P=0.027, paired t-test), and this change was also statistically significant between both groups (P=0.024, unpaired t-test). In terms of visual field defect progression, mean changes of MD deterioration were statistically significant in the placebo group at 12 months (P=0.017, Mann–Whitney U test) and 18 months (P=0.050, Mann–Whitney U test) after the baseline, but no significant changes were observed in the BCAC group during the 24-month trial. In the right eye, a few eyes were excluded due to the inclusion criteria as described in the Methods section, but similar effects for IOP reduction were also observed in the BCAC group (−0.70±0.82 mmHg, P=0.037, paired t-test) as well as between groups (P=0.023, unpaired t-test) at 24 months from the baseline. A statistically significant decrease was observed in MD deterioration in the placebo group at 18 months (P=0.02, Mann–Whitney U test) and 24 months (P=0.01, Mann–Whitney U test) after the baseline, but no significant changes were observed in the BCAC group during the 24-month trial.
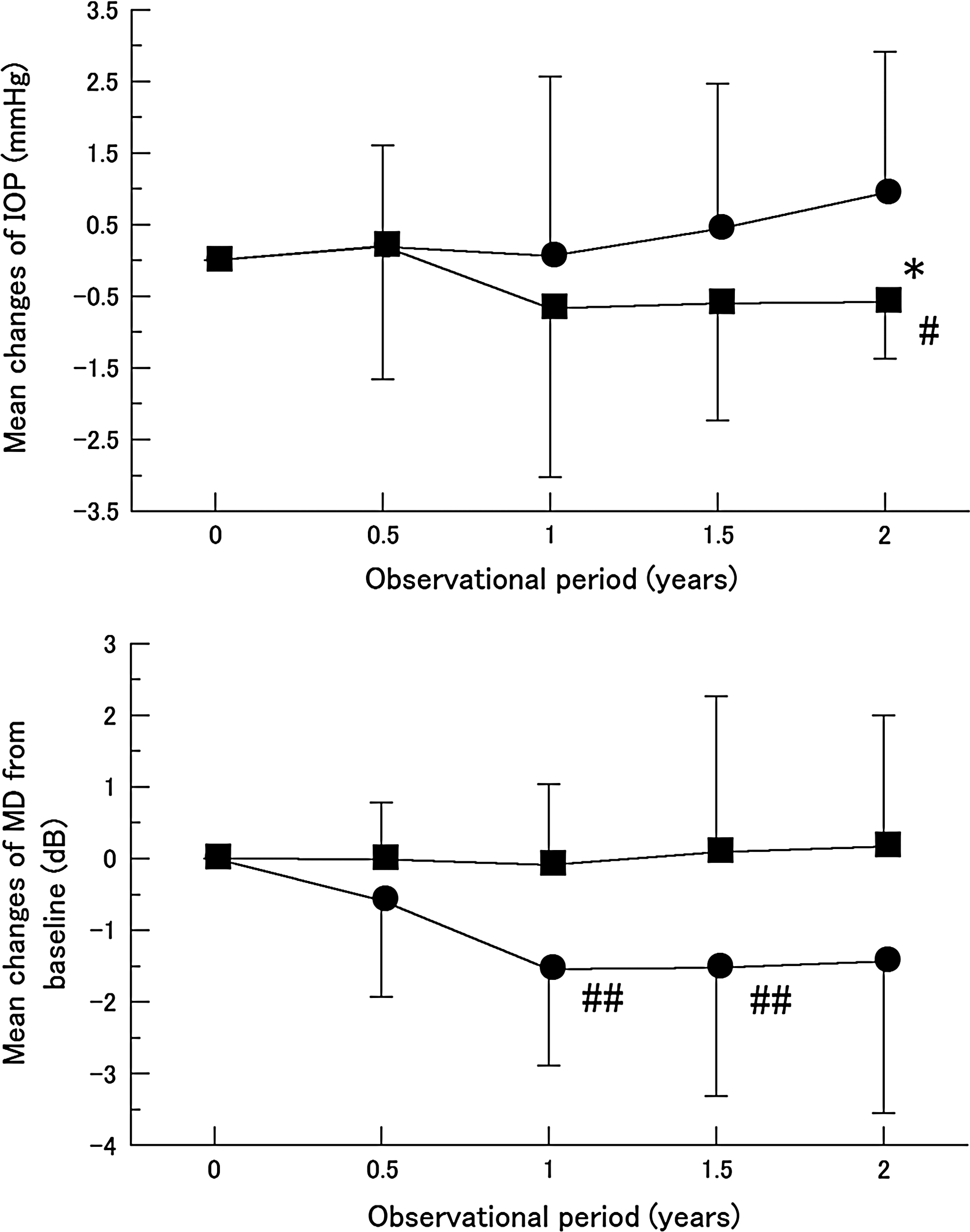
The time course changes of intraocular pressures (IOPs) and visual field mean deviation (MD). The differences between baseline and each time point of the trial period (0.5, 1, 1.5, and 2 years) of IOPs (upper) and MD (bottom) of the left eyes in the BCAC intake group (filled square) or placebo intake group (filled circle) were plotted. Data are expressed as mean±SD. Significant difference between groups (*P<0.05, unpaired t-test). Significant intergroup difference between each time point and baseline (#P<0.05, paired t-test; ##P<0.05, Mann–Whitney U test).
P values for difference between anthocyanin and placebo treatment groups were calculated by Fischer-test for gender and unpaired t-test for others.
Mean±SD (all such values).
95% CI in parentheses (all such values).
BCACs, black currant anthocyanins.
In terms of the systemic conditions, including blood pressure and pulse rates, no significant changes were observed in the analysis between groups and intergroups (Fig. 5).
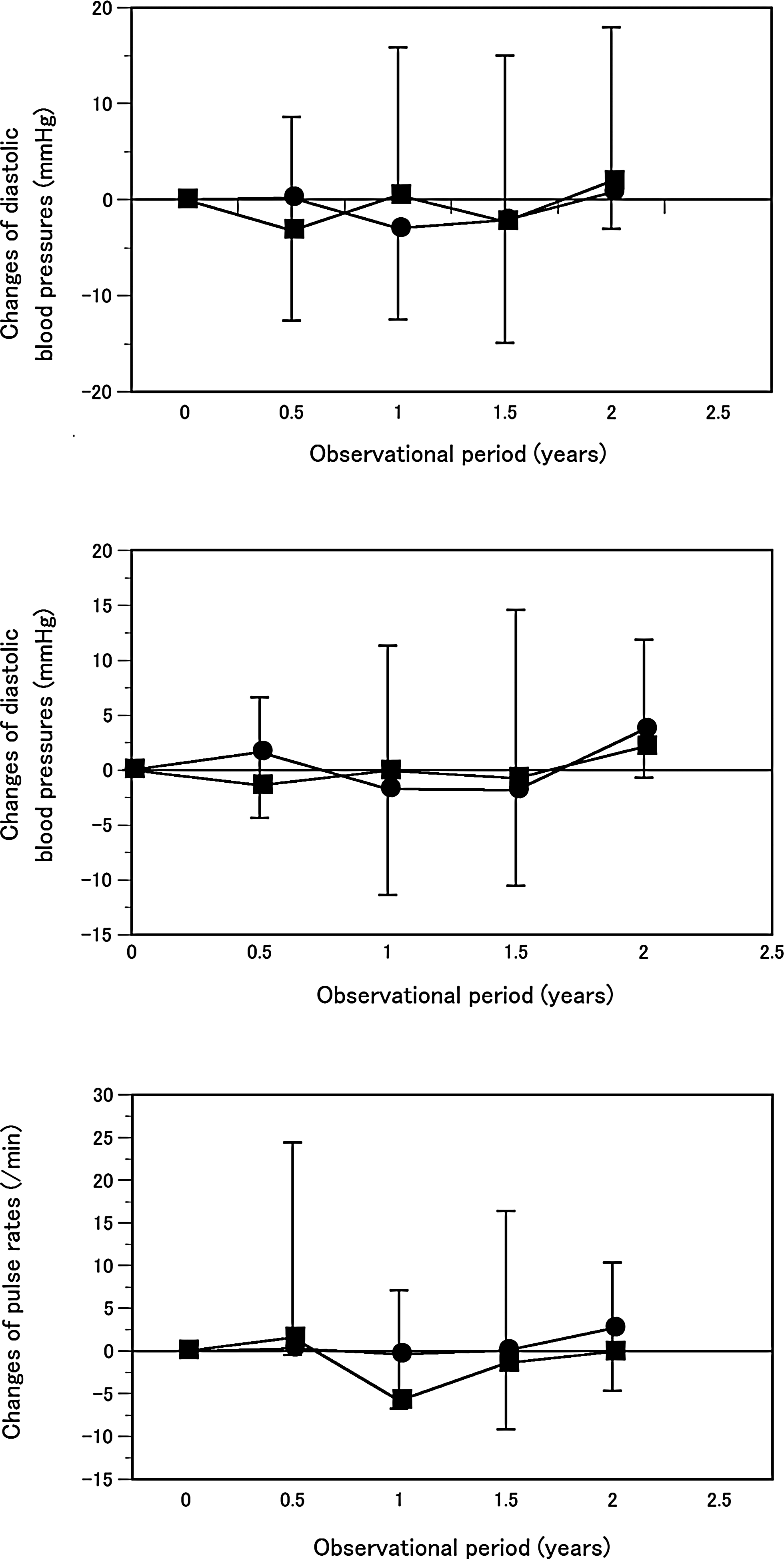
The time course changes of mean systemic and diastolic blood pressures and pulse rates. The differences between baseline and each time point of the trial period (0.5, 1, 1.5, and 2 years) of mean systemic systolic and diastolic blood pressures and pulse rates in the BCAC intake group (filled square) or placebo intake group (filled circle) were plotted. Data are expressed as mean±SD. Significant differences between groups or intergroups were not observed.
Discussion
It has been demonstrated that 4 types of BCACs were purified and characterized: delphinidin-3-rutinoside (D3R), delphinidin-3-glucoside (D3G), cyaniding-3-rutinoside (C3R), and cyaniding-3-glucoside (C3G). 11 Upon oral administration, these BCACs were directly absorbed into plasma without degradation and then transferred beyond the blood–aqueous barrier and blood–retina barrier into ocular tissues, including the retina, choroid, and ciliary body. 12 In vitro experiments revealed that BCACs caused several kinds of ocular biological activities, including stimulation of rhodopsin regeneration in frog retinas 13 and suppression of ocular globe elongation in chick myopia models 14 in addition to the ET-dependent vasodilation in the bovine ciliary body. 5 In vivo, oral administration of the BCACs significantly improved dark adaptation and video display terminal work-induced transient refractive alteration in healthy human volunteers. 4
In our earlier study, we found that systemic administration of BCACs (50 mg/day) caused a significant beneficial effect against glaucoma visual field progression. 7 Although we do not know what kind of underlying mechanism is involved in this effect, we can speculate that BCACs may affect ocular blood circulation and/or IOP, because BCACs are known to modulate ET-dependent biological properties as above. 5 In fact, the oral administration of BCACs capsules (50 mg/day) normalized the abnormal plasma concentration levels of ET-1 in patients with NTG, 6 and caused a significant increase in ocular blood circulations around ONH.6,7 No statistically significant difference was observed between the BCAC and placebo groups in the trial. IOPs of these glaucoma patients were controlled by antiglaucoma medications at trial baseline and the following 24 months. 7 However, in the present study, among the participants we selected and analyzed 21 who were treated by a single antiglaucoma drop of prostaglandin analogs. Upon administration of BCACs, we found a statistically significant decrease of IOP, and significantly less MD deterioration in comparison to the placebo groups. In addition, BCAC-induced IOP reduction of healthy subjects was ∼1–2 mmHg. According to a recent meta-analysis investigating the efficacy of the addition of the antiglaucoma drops of β-adrenergic antagonists, carbonic anhydrase inhibitors, or α2-adrenergic agonists to prostaglandin analogs, IOP reduction of ∼2–3 mmHg could be expected in patients with glaucoma. 15 In the current analysis, IOP reduction by BCACs in glaucoma patients treated with single prostaglandin analogs was 0.6 mmHg greater than the baseline, and it was 1.5 mmHg greater than that of patients receiving placebo at 24 months. Although the rate of IOP reduction in patients with OAG by BCACs was less than that in those receiving the antiglaucoma drops, we speculated that this could be beneficial to reduce glaucoma progression if this BCAC-induced IOP reduction was continued long term.
Several studies have shown that ET-1 may be implicated in glaucoma16–20 and other ocular ischemic vascular diseases such as diabetic retinopathy, 21 retinal vein occlusion, and retinal artery occlusion. 22 It has been shown that there are statistically significant differences of plasma ET-1 levels in glaucoma patients as compared to those in control subjects.19,20,23 ET metabolism is believed to be involved in the glaucoma etiology, and therefore modulation of ET metabolism through its specific receptors is thought be a promising therapeutic strategy for these ocular diseases. 24 The ET-1 receptors belong to the family of G-protein-coupled receptors. Three types, ETA, ETB (subtypes 1 and 2), and ETC receptors, have been characterized in humans. 25 Within ocular tissues, ETA and ETB are also constitutively expressed in human uveal tissues, 26 the retina and ONH. 27 Functionally, ET-1 induces vasoconstriction by its interaction with ETA receptors on vascular smooth muscle cells, but can also stimulate NO-mediated vasodilation by activation of ETB receptors on endothelium. 24 Thus, blocking ETA receptor action or stimulation of ETB receptor action is theoretically required for the purpose of lowering IOP levels. Interestingly, in fact, human and animal studies demonstrated that ETA receptor blockers28,29 and an ETB receptor agonist30,31 indeed caused IOP reduction and an increase of ocular blood flow. Regarding the effect of BCACs toward ET-1 metabolisms, it was reported that BCACs could stimulate the ETB receptor in a ciliary body. 5 Taken together, we speculated that orally administrated BCACs transferred into ocular tissues possibly caused activation of the ETB receptor functions in the ciliary body, thereby resulting in IOP reduction and an increase of the ocular blood circulation by its NO-induced vasodilation effect. However, since BCACs possess several kinds of biological effects other than ET-dependent mechanisms such as antioxidants and anti-inflamation,32,33 for our next project, it will be important to identify the molecular mechanisms causing the beneficial effects of BCACs toward IOP reduction and increased ocular blood flow.
Footnotes
Author Disclosure Statement
No competing financial interests exist.