
Abstract
Abstract
Purpose:
To report the effects of intravitreal bevacizumab injection (IVBI) in a patient affected by retinal neovascularizations (RNVs) associated with myelinated nerve fibers (MNF) and complicated by vitreous hemorrhage.
Methods:
A 23-year-old female was referred because of sudden visual acuity deterioration in the left eye. Nine years earlier, the subject underwent retinal laser photocoagulation for recurrent vitreous hemorrhages related to the development of RNV associated with MNF. The ophthalmological evaluation revealed a new recurrence of vitreous hemorrhage associated with fluorescein leakage from RNV. After careful discussion, the patient underwent IVBI.
Results:
One month after the injection, the best corrected visual acuity (BCVA) improved from 20/400 to 20/100, with a vitreous hemorrhage resolution, and cessation of fluorescein leakage. Over the 24-month follow-up, 2 additional IVBIs were administered due to further vitreous hemorrhage associated with fluorescein leakage from RNV, achieving a final BCVA of 20/80.
Conclusions:
IVBI may temporarily counteract the vascular hyperpermeability typical of RNV associated with MNF, leading to the cessation of fluorescein leakage, but does not result in RNV regression.
Introduction
We describe a patient affected by MNF and RNV, who complicated with vitreous hemorrhage, and was successfully treated with intravitreal bevacizumab injection (IVBI).
Case Report
A 23-year-old girl was referred because of visual deterioration in the left eye (LE). General history was negative. The patient was diagnosed with MNF in 1990, and underwent laser photocoagulation in 2000 because of repeated vitreous hemorrhages related to the development of RNV. The patient referred a stabilization of the picture until May 2009, when she was referred to our center because of sudden and spontaneous visual acuity deterioration. Best corrected visual acuity (BCVA) was 20/20 (−0.50 D) in the right eye (RE) and 20/400 (−0.50 D) in the LE, with referred amblyopic defect in the LE. Ophthalmoscopic examination of the RE was normal. The LE showed white patches with feathery edges, located around the optic disc and along the superotemporal arcade. Atrophic changes were also detectable at the posterior pole, especially in the superotemporal and superonasal sectors, owing to previous thermal laser treatments. A vitreous hemorrhage associated with small retinal hemorrhages was also detectable (Fig. 1).
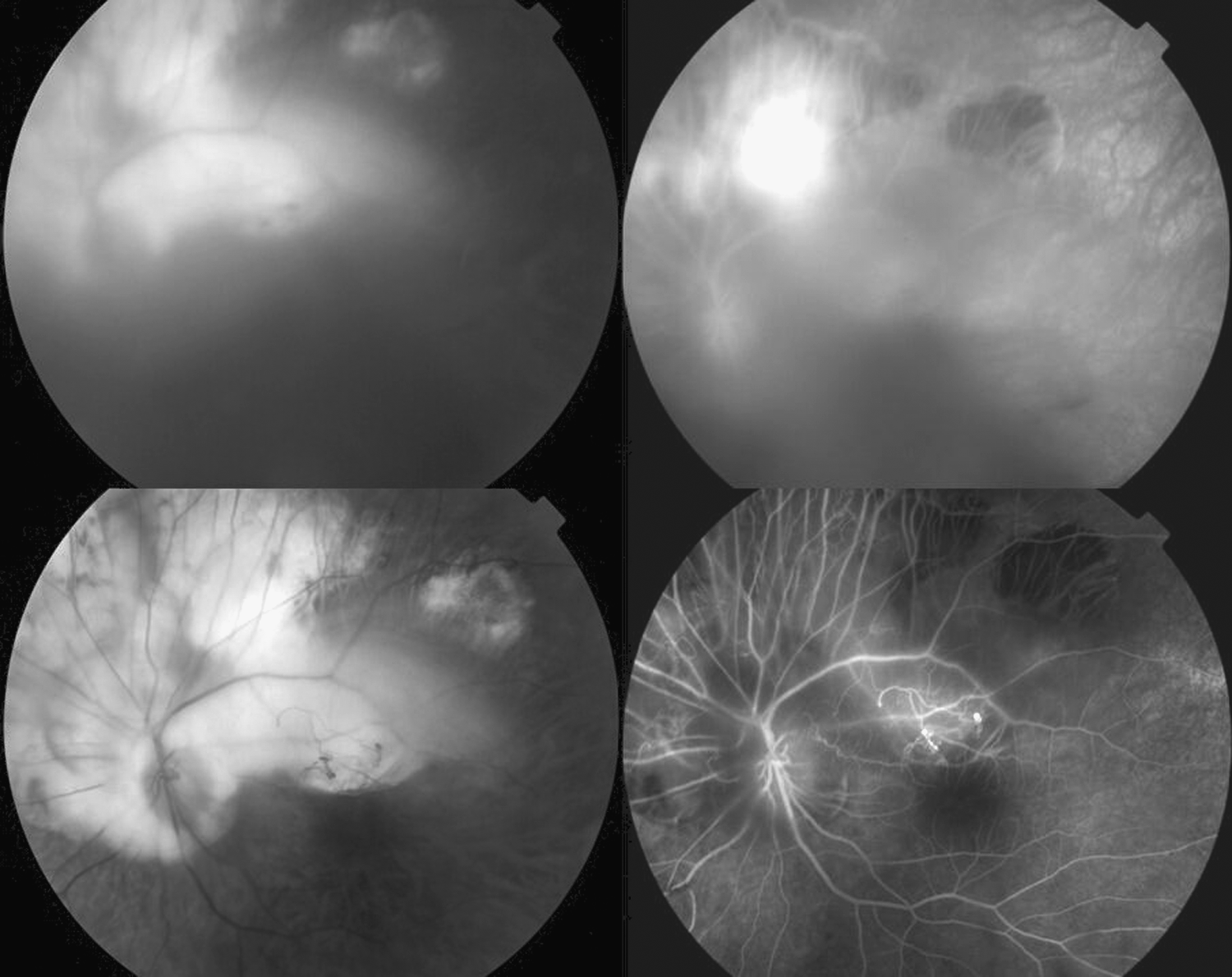
Top left: Image of the left eye showing vitreous hemorrhage secondary to retinal neovascularization (RNV) related to myelinated nerve fibers. Top right: fluorescein angiography revealing dye leakage from RNVs. Bottom left: Photograph after the first intravitreal bevacizumab injection, with vitreous hemorrhage resolution. Bottom right: fluorescein angiography showing the absence of late leakage from the retinal neovascularization.
Fluorescein angiography showed a hypofluorescence corresponding to the MNF, due to their masking affect, without evidence of retinal ischemia. The fluorescein leakage distinctive of the RNV was visible especially along the superotemporal arcade (Fig. 1). The patient was simply observed 1 month to allow a spontaneous resolution of the vitreous hemorrhage to occur. Unfortunately, the vitreous hemorrhage intensified, making the fundus examination very difficult. After a thorough discussion, the patient was advised to undergo IVBI, which she accepted, signing an informed consent. IVBI was uneventful. After 1 month, the BCVA was 20/100, with a vitreous hemorrhage resolution and an absence of fluorescein leakage from the RNV. Over the 24-month follow-up, the patient required 2 additional IVBIs, due to repeated vitreous hemorrhages associated with fluorescein leakage from the RNV. At the end of the 24-month follow-up, BCVA in LE was 20/80. Interestingly, IVBI did not determine a RNV regression, but rather was associated with the reduction of the vascular permeability, as pointed out by the cessation of fluorescein leakage (Fig. 1).
Discussion
Many treatment options have been proposed for RNV related to MNF, including observation, laser photocoagulation, cryotherapy, and pars plana vitrectomy.1–4 Our patient had already undergone laser photocoagulation in the past, which brought about wide atrophic changes at the posterior pole. Bearing in mind the potential pathogenetic mechanism of ischemia-related modifications secondary to MNF, a treatment based on anti-VEGF blocking was tried in this unusual condition. The results have been encouraging. We obtained the resolution of the vitreous hemorrhage in association with the cessation of the fluorescein leakage from the RNV, together with a visual acuity improvement. Nevertheless, we have to underline that IVBI was unable to induce the RNV regression to obtain a definitive stabilization of the clinical picture. We hypothesize that the anti-VEGF molecule was able to temporarily stop the vascular hyperpermeability, promoting the vitreous hemorrhage resolution.
Conclusion
In essence, our case report describes a patient affected with MNF complicated by RNV and vitreous hemorrhage, who benefited from multiple bevacizumab injections. IVBI may temporarily stop the vascular hyperpermeability of RNV, leading to the cessation of bleeding, as indicated by the cessation of the fluorescein leakage. Further studies are needed to ascertain the best therapeutic approach for this rare complication.
Footnotes
Author Disclosure Statement
The authors have no proprietary or commercial interest in any materials discussed in this article.