
Abstract
Abstract
Purpose:
To investigate clinically the effects of yeast-fermented bilberry extract on visual outcomes in myopic eyes.
Methods:
In a prospective, randomized, placebo-controlled, cross-over study, we examined 30 eyes of 30 middle-aged healthy volunteers (mean age±standard deviation, 39.5±7.2 years) with myopia [manifest spherical equivalent, −2.40±1.88 diopters (D)], who were randomly assigned to 1 of 2 oral regimens: fermented bilberry extract (400 mg/day) or placebo. We quantitatively assessed visual acuity, refraction, pupil constriction rate, accommodation, and mesopic contrast sensitivity (CS), before and 1 month after treatment. Only the right eyes were tested. The amplitude of accommodation and CS were measured with an accommodometer (D'ACOMO; WOC) and a CS unit (VCTS-6500; Vistech), respectively. From the CS, the area under the log contrast sensitivity function (AULCSF) was calculated.
Results:
The mean amplitude of accommodation increased significantly, from 4.62±1.88 D before treatment, to 5.33±2.03 D after treatment in the study group (Wilcoxon signed-rank test, P=0.002). Moreover, the mesopic AULCSF was significantly increased, from 1.04±0.16 before, to 1.13±0.17 after, treatment (P=0.009). However, we found no significant changes in accommodation or AULCSF in the control group (P>0.05), or any significant changes in any other parameters in either group (P>0.05).
Conclusions:
The present data show that fermented bilberry extract is effective in causing increases in subjective accommodation and in mesopic CS in myopic eyes.
Introduction
Methods
Thirty eyes of 30 healthy volunteers (20 men and 10 women) who had no ophthalmic disease other than myopic refractive errors were enrolled in this prospective study. The sample size in this study offered 82% statistical power at the 5% level in order to detect a 0.7-D difference in accommodation between the 2 groups, when the standard deviation (SD) of the mean difference was 1.3D. It offered 84% statistical power at the 5% level in order to detect a 0.10 difference in the area under the log contrast sensitivity function (AULCSF) between the 2 groups, when the SD of the mean difference was 0.18. The age of the volunteers was 39.5±7.2 years (mean age±SD; range, 31 to 53 years old). The manifest refraction (spherical equivalent) was −2.40±1.88 diopters (D) (range: −0.50 to −5.63 D). Informed consent was obtained from all volunteers in accordance with institutional guidelines, according to the tenets of the Declaration of Helsinki.
The study was conducted in a prospective, randomized, placebo-controlled, 2-period cross-over fashion. This study was registered in the UMIN Clinical Trial Registry (UMIN 000007741). The subjects were randomly assigned to 1 of the 2 regimens: oral administration of fermented bilberry extracts (Fermented Blueberry, Ajinomoto, Co., Inc., Tokyo, Japan), as the study group, and oral placebo, as the control group, by a designated study controller. Fermented bilberry extract is a polyphenol-rich fraction obtained from bilberry fermentation with wine yeast (Saccharomyces cerevisiae) and purified by precipitation with hot alcohol. 10 The subjects took either fermented bilberry extract or a placebo, twice a day for 4 weeks in a blind manner. The active capsules contained 200 mg of fermented bilberry extract, and the placebo capsule contained only inactive ingredients (rapeseed oil). The active and placebo capsules were identical in appearance. After the first 4-week treatment, a 4-week washout period was employed to allow any effect of these treatments on visual performance to dissipate. In the second 4-week treatment period, the subjects who first received active capsules were then given placebo, and the subjects who first received placebo were given active capsules. The participants and investigators were blinded to group assignment. Before and after each 4-week treatment, we determined the following variables: logarithm of the minimal angle of resolution (logMAR) of uncorrected visual acuity (UCVA), logMAR of best spectacle-corrected visual acuity (BSCVA), subjective and objective refraction (spherical equivalent), pupil constriction rate, subjective accommodation, and mesopic CS, in addition to the usual slit-lamp biomicroscopic and funduscopic examinations. Only the right eyes were tested, and blood and urine drug levels were not evaluated in this study.
Objective refraction was measured with an autorefractometer (RK-5; Canon, Tokyo, Japan). The near point of accommodation was evaluated with an accommodometer (D'ACOMO; WOC, Kyoto, Japan) with a constant stimulus speed during binocular viewing using polarizing filters. A spherical lens of +2 or +3 D was added to the distance correction only for the spherical component, and the patient was required to read a cross-shaped target that corresponded in size to a visual acuity of 20/20 at a distance of 30 cm. The chart was slowly brought closer, until the patient reported blurring of the image. The target was then moved back until it became clear. The distance in diopters at which blurring and refocusing occurred was recorded as the near point of accommodation. The amount of accommodation was calculated from the far and near points. The rate of pupil constriction was measured with a compact integrated pupillograph (TriIRIS, Hamamatsu Photonics, Shizuoka, Japan) after 5 min of dark adaptation. CS function was measured with a CS unit (VCTS-6500; Vistech, Dayton, OH) under mesopic conditions (50 lux). The test was performed with best spectacle correction at 2.5 m. From the CS, the AULCSF was determined as previously described. 12 In brief, the log of CS was plotted as a function of log spatial frequency, and third-order polynomials were fitted to the data. The fitted function was integrated between the fixed limits of log spatial frequencies of 0.18 (corresponding to 1.5 cycles/degree) and 1.26 (corresponding to 18 cycles/degree), and the resultant value was defined as the AULCSF. We performed at least 3 measurements for each eye, and the average value was used for statistical analysis. All examinations were performed by one experienced ophthalmic technician.
All statistical analyses were performed using StatView version 5.0 (SAS Institute, Inc., Cary, NC). The Wilcoxon signed-rank test was used for statistical analysis to compare the pre- and post-treated data. The results are expressed as mean±SD, and a value of P<0.05 was considered statistically significant.
Results
The demographics of the study population before treatment are summarized in Table 1. Before treatment, there was no significant difference in LogMAR UCVA (Wilcoxon signed-rank test, P=0.65), LogMAR BSCVA (P=1.00), subjective refraction (P=0.46), objective refraction (P=0.31), pupil constriction rate (P=0.50), accommodation (P=0.61), or mesopic AULSCF (P=0.23), between the 2 groups. The amplitude of accommodation in the study group was significantly increased from 4.62±1.88 D (range, 1.28 to 7.51 D) before treatment to 5.33±2.03 D (range, 1.38 to 8.21 D) after treatment (P=0.002). On the other hand, after treatment in the control group, it was not significantly different, from 4.64±2.03 D (range, 1.08 to 9.13 D) before treatment, to 4.67±2.06 D (range, 0.96 to 9.43 D) (P=0.52) (Fig. 1). The AULCSF was significantly increased, from 1.04±0.16 (range, 0.70 to 1.40) before treatment to 1.13±0.17 (range, 0.77 to 1.45) after treatment in the study group (P=0.009). There was also a significant increase in CS at 2 of 5 spatial frequencies (at 3 and 6 cycles/degree) after treatment in the study group (Fig. 2). On the other hand, the AULCSF was not significantly changed, from 1.08±0.11 (range, 0.92 to 1.32) before treatment, to 1.09±0.11 (range, 0.85 to 1.35) after treatment in the control group (P=0.67). There was no significant change in CS at any spatial frequencies after treatment in the control group (Fig. 3). Otherwise, we found no significant differences in LogMAR UCVA (P=0.87), LogMAR BSCVA (P=1.00), subjective refraction (P=0.48), objective refraction (P=0.78), or pupil constriction rate (P=0.55) as a result of treatment in the study group. Similarly, we found no significant differences due to treatment in LogMAR UCVA (P=0.97), LogMAR BSCVA (P=1.00), subjective refraction (P=0.40), objective refraction (P=0.20), or pupil constriction rate (P=0.61) in the control group.
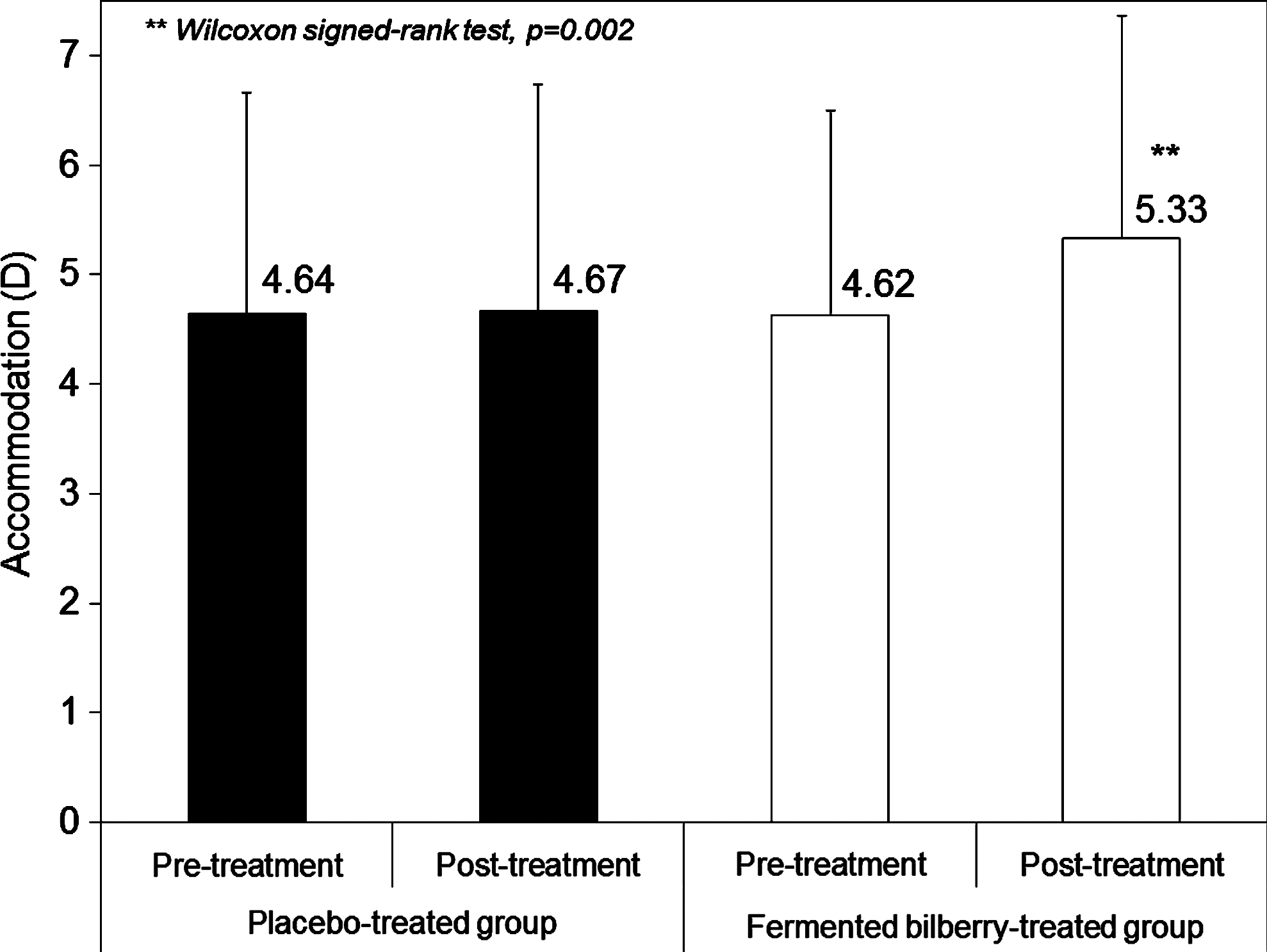
There was a significant improvement of accommodation after fermented bilberry extracts treatment (P=0.002, Wilcoxon signed-rank test), but no significant change after placebo treatment (P=0.52). D, diopters.
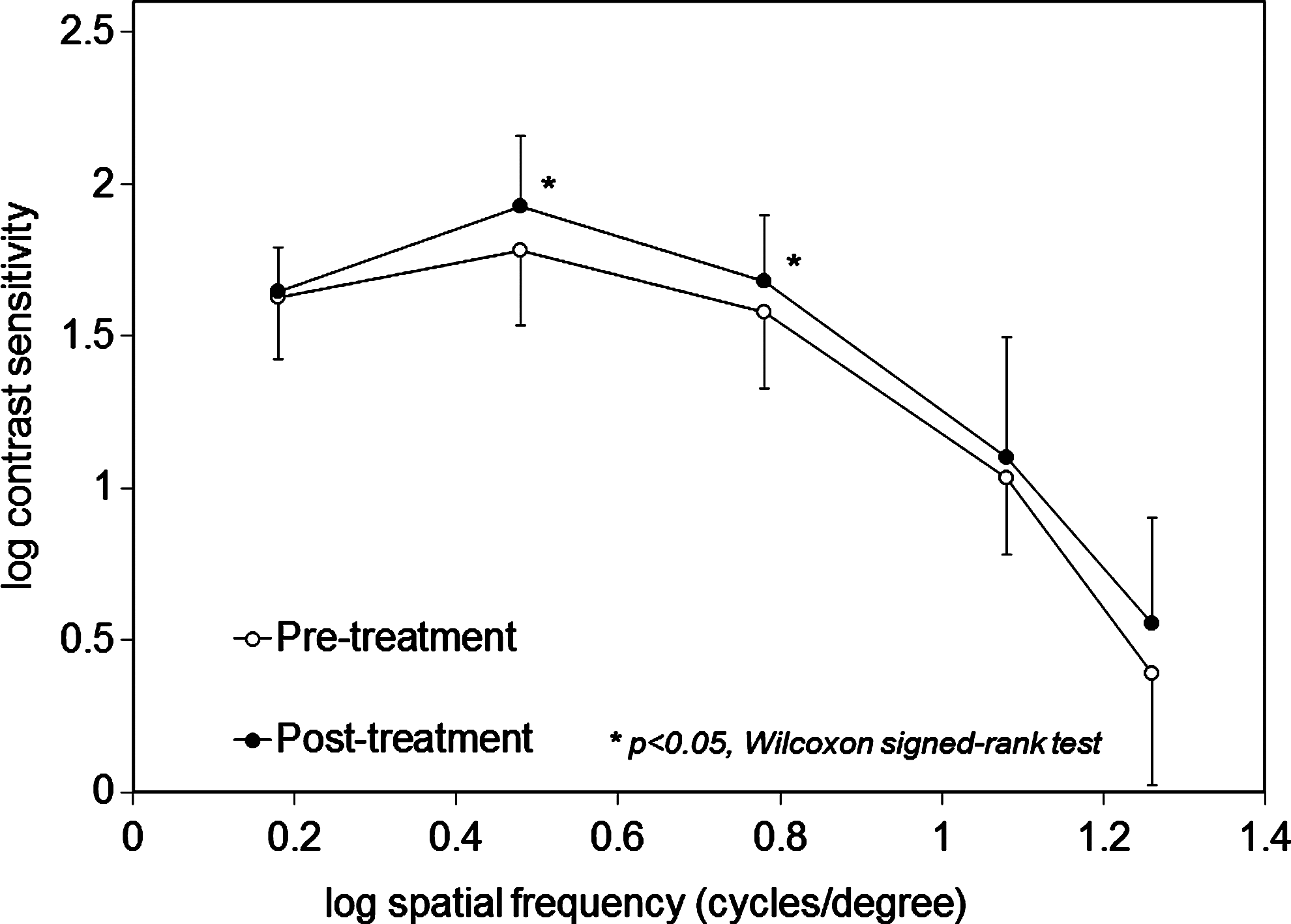
There was a significant improvement of the area under the log contrast sensitivity function under mesopic conditions after fermented bilberry extracts treatment (P=0.009, Wilcoxon signed-rank test).
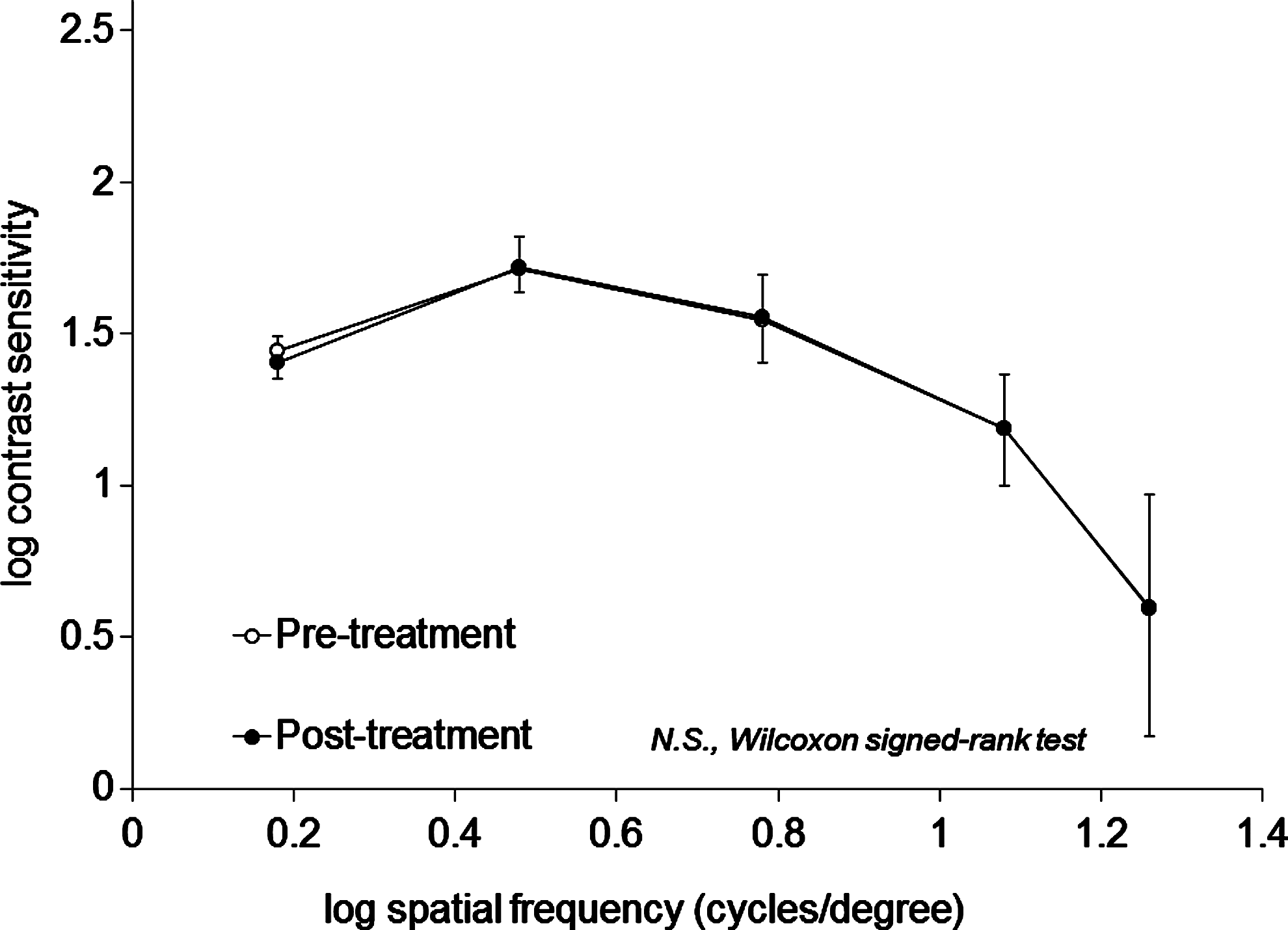
There was no significant change in the area under the log contrast sensitivity function under mesopic conditions after placebo treatment (P=0.67, Wilcoxon signed-rank test). N.S., no significance.
LogMAR, logarithm of the minimal angle of resolution; UCVA, uncorrected visual acuity; BSCVA, best spectacle-corrected visual acuity; D, diopters; AULCSF, area under the log contrast sensitivity function.
Discussion
In the present study, our results demonstrated that fermented bilberry extracts significantly improve the amplitude of accommodation and mesopic CS in eyes with myopia. To the best of our knowledge, this is the first study that investigates the effects of yeast-fermented bilberry extract on visual function in myopic subjects. It has been shown that anthocyanosides accelerate the resynthesis of rhodopsin,13,14 and modulate retinal enzymatic activity. 15 In the present study, we used fermented bilberry extracts for middle-aged myopic subjects (age, 39.5±7.2 years, refraction, −2.40±1.88 D) after oral administration for 4 weeks. The differences in study design regarding materials, doses, durations, methods for evaluating night vision, and types of subjects (age and refraction) may have contributed to the discrepancy. Especially regarding subject age, no placebo-controlled clinical studies for a middle-aged population, who tended to have difficulty in accommodation and nocturnal vision, and to use these nutritional supplements, has been conducted so far, suggesting its importance in clinical use for these subjects.
With regard to the amplitude of accommodation, as far as we can ascertain, this is also the first study that investigates the subjective accommodation after bilberry extract treatment in a clinical setting. Nakanishi et al. 16 reported that the oral intake of anthocyanosides brought about a reduction of the dark adaptation threshold and promoted recovery from transient refractive alternation induced by visual display terminal work, as well as subjective symptoms of visual fatigue in healthy subjects. The authors speculate that accelerated resynthesis of rhodopsin, modulation of retinal enzyme activity, and improved microcirculation may play a role in the improvement of visual function in the present study. However, the active compounds responsible for improved accommodation and mesopic CS were not identified in this study. Mauray et al. demonstrated that fermented bilberry extract exerts more effective antiatherogenic activity in vivo than the bilberry extract, suggesting that fermentation generates some new compounds with improved health-promoting properties as compared with the bilberry extract. 11 It is known that extracts from other fermented soybean foods prevented the progression of atherosclerosis, improved oxidative stress markers, and inhibited intimal thickening.17,18 Other compounds produced by a fermentation process, such as organic acids observed in wine, may contribute to these beneficial effects. Hence, although the exact reason for the improvement of visual function still remains unclear, the process of fermentation may have also added to the positive effects of this supplement in the current study. Nevertheless, we did not directly compare the effect of natural and fermented bilberry extracts on visual outcomes in this study, and thus, further studies are necessary to confirm the effect of fermentation alone.
There are at least 2 limitations to the present study. First, the sample data are comparatively limited, and, thus, offered 82% to 84% statistical power at the 5% level; so, a larger number of subjects are necessary for confirming the authenticity of the results. Second, we did not quantify the individual anthocyanin glycosides in the fermented bilberry extracts by high-performance liquid chromatography. However, it has already been demonstrated that the bilberry extract used in this study contains 15 different anthocyanins, derived from 5 aglycones (cyanidin, delphinidin, malvidin, peonidin, and petunidin); whereas almost no native anthocyanins were detected in fermented bilberry extracts. 11 In addition, high-performance liquid chromatography demonstrated that fermented bilberry extracts largely retained on the column show a large peak with a maximum wavelength absorption similar to those obtained with native anthocyanins (508 nm), indicating that the anthocyanins in fermented bilberry extracts are largely condensed into complex polymers. Further studies are required to identify the compounds responsible for these effects and to clarify the possible mechanism underlying such effects.
In conclusion, our study revealed that yeast-fermented bilberry extracts were effective for the improvement of subjective accommodation or mesopic CS in myopic eyes, although no possible mechanism of this effect could be offered. In the authors' experience, fermented bilberry extracts appear to be a good treatment option for middle-aged subjects, who tend to have difficulty in accommodation and nocturnal vision, and to use these nutritional supplements often in daily life. Further studies are necessary for the clarification of these aspects.
Footnotes
Acknowledgments
The authors are grateful to C.W.P. Reynolds for his careful linguistic assistance with this article.
Author Disclosure Statement
Dr. Kamiya is a consultant to Ajinomoto Co., Inc. The remaining authors have no commercial or propriety interest in the product or company described in the current article.