
Abstract
Abstract
Purpose:
The aim of this study was to evaluate the association between different intraocular pressure (IOP)-lowering medications and IOP measurements by dynamic contour tonometry (DCT) and Goldmann applanation tonometry (GAT) in a glaucoma and ocular hypertensive population.
Methods:
In a prospective, observational case series study, 410 eyes from 410 consecutive patients with open-angle glaucoma (OAG) or ocular hypertension (OHT), were enrolled. All eyes included in the study received unaltered ocular hypotensive medication for at least 6 months before IOP measurement. All eyes underwent 2 GAT and 3 DCT measurements, and their means were used for the analysis.
Results:
DCT-GAT IOP difference (ΔIOP) did not differ statistically significantly (P=0.49) between OAG and OHT group yielding a mean±SD of 4.26±2.02 mmHg and 4.41±2.25 mmHg, respectively. The number of IOP-lowering agents did not have any statistically significant influence on ΔIOP (p=0.177), DCT (P=0.28) and GAT (P=0.13) measurements. A statistically higher ΔIOP was revealed in monotherapy patients receiving Carbonic Anhydrase Inhibitors (CAIs) (ΔIOP=5.75 mmHg) in comparison to patients receiving Prostaglandin Analogs (ΔIOP=4.09 mm Hg) or beta Blockers (ΔIOP=3.78 mmHg) as single topical therapy (F=4.373, P=0.005). Eyes treated with CAIs as a part of the ocular hypotensive therapy yielded a significantly greater ΔIOP (P=0.0035) than those without CAIs in the therapeutic schema.
Conclusions:
The difference between DCT and GAT IOP measurements is found to be statistically significantly higher in patients receiving CAIs either as monotherapy or as a part of a combined ocular hypotensive treatment, while DCT and GAT readings remain unaffected. The type of diagnosis and the number of ocular hypotensive medications had no statistically significant influence on ΔIOP.
Introduction
To our knowledge, no study has been published till date that compares the effect of different types of anti-glaucoma agents on DCT and GAT. The aim of this prospective cross-sectional study was to investigate the possible association between different IOP-lowering medication types and differences in DCT and GAT measurements in a glaucoma and ocular hypertensive population.
Methods
In a randomized cross-sectional study, 410 eyes from 410 consecutive patients with the diagnosis of open-angle glaucoma (OAG) or ocular hypertension (OHT) were enrolled, recruited from the outpatient glaucoma unit of the Clinic Pallas Ophthalmology Department in Olten, Switzerland. This prospective study was performed in adherence with the Declaration of Helsinki for research involving human subjects and after approval from the Institutional Review Board of the Pallas Eye Clinic. After informed consent had been obtained, participants underwent a complete ophthalmic examination, including a review of medical history, best-corrected visual acuity (BCVA) assessment, slit-lamp examination, fundus observation, gonioscopy, and measurement of IOP and CCT. In addition, a complete history of anti-glaucoma medication was obtained for each patient. All patients included in the study had received the same anti-glaucoma agents for at least 6 months before IOP measurement. For patients recorded to have no IOP-lowering treatment, a wash-out period of 3 months was demanded in case these subjects had been under treatment in a past time. Subjects of the OAG group included those with diagnoses of primary open-angle glaucoma (POAG), pseudoexfoliative glaucoma (PEXG), normal tension glaucoma, and pigmentary glaucoma (PG), characterized by typical glaucoma visual field loss and optic nerve abnormality. Specifically, structural damage required the presence of thinning or notching or a cup-to-disc ratio asymmetry of 0.2, and functional damage required a confirmed threshold glaucomatous visual field defect following definitions given by Topouzis et al. in previous reports. 29 In addition, subjects were classified as having glaucoma when the clinical judgment was strongly in favor of the presence of glaucoma, even though the strict criteria (requiring both visual field defect and optic disc abnormality) were not fulfilled. In the OHT group, patients with an elevated IOP (>21 mmHg at the diagnosis baseline without IOP-lowering medication) were classified, without any other functional or structural damage of the optic nerve. Other inclusion criteria for both glaucomatous and ocular hypertensive subjects were (1) subject age >18 years, (2) BCVA >20/40, (3) corneal astigmatism <3 diopters, and (4) no history of amblyopia or any ocular disease or surgery that might confound the recognition of a test result that is due solely to glaucoma. In addition, patients with poor cooperation or poor quality of DCT readings were excluded from the study. All subjects were in mental and physical capacity to undergo the tests and were willing to participate in the study.
CC was estimated with the Canon Full Auto RK-F1 Autorefractor Keratometer (Canon Europe NV); CCT was measured by noncontact optical low-coherence reflectometry (OLCR; Haag-Streit) before tonometry; and only measurements with a standard deviation of 0.8 μm and less were accepted. All eyes underwent 2 tonometry measurements with a Goldmann applanation tonometer made by the same experienced operator (M.K.) masked to the patient data and after a rest period of 10 min, in order to minimize as possible the tonographic effect of applanation tonometry; 3 DCT measurements were acquired from another operator (A.T.) masked to the GAT measurements. GAT and DCT measurements were always performed at the eye defined by the electronic randomization protocol; when both eyes fulfilled the inclusion criteria, the readings were recorded from an observer and then, the mean of these measurements was used for the data analysis. In case of IOP fluctuation during the cardiac pulse cycle by GAT measures, the measurement was recorded in the middle of the pulsation amplitude. All DCT measurements had to meet 2 significant criteria. First, corneal contact with the DCT was pertained so long as at least 8 consecutive pulsations were emitted by the audible regular flickering signal. Furthermore, out of the 5 quality levels provided by DCT, with 1 being the best and 5 being the poorest, only measurements of quality 3 or less were evaluated and included in the study, as recommended by the manufacturer.
Statistical analysis was performed with Medcalc statistical software (version 9.3.0.0; Medcalc) and SPSS (v. 17.0 for Windows; SPSS INC). In order to evaluate the agreement between measurements obtained by DCT and GAT, Bland–Altman plots were used, and the differences of measurements between the 2 techniques were plotted against their averages. Due to the fact that the data were not in all cases normally distributed, both parametric and nonparametric methods were used. For normally distributed sizes, Pearson correlation was used to analyze the degree of association between 2 continuous variables, and one-way analysis of variance (ANOVA) was utilized to study the influence of a qualitative factor on another continuous variable. The association of not normally distributed sizes was assessed through rank correlation by calculating Spearman's coefficient rho. Nonparametric Kruskal–Wallis and Mann–Whitney tests were also used to examine associations between categorical variables and continuous or ordered outcomes. A P-value of <0.05 was defined as being statistically significant for all statistical tests.
We certify that all applicable institutional and governmental regulations with regard to the ethical use of human volunteers were followed during this research.
Results
The study included 410 eyes of 410 Caucasian participants (184 women). From these patients, 287 patients of the OAG group and 123 of the OHT group met the selection criteria, and their data were used for the statistical analysis. The main demographic and clinical characteristics of the 2 groups are listed in Table 1. The group of OAG patients included eyes with primary OAG (n=173), PEXG (n=63), normal-tension glaucoma (n=39), and pigmentary glaucoma (n=12). The mean GAT IOP was 15.32±3.82 mm Hg (mean±SD), and the mean DCT IOP was 19.63±4.47 mm Hg. The mean DCT readings were 4.3±2.1 mm Hg higher than the GAT readings (P<0.0001). Figure 1 depicts a Bland & Altman plot of DCT and GAT readings. This method comparison graph displays a scatter diagram of the differences plotted against the averages of the 2 measurements. Horizontal lines are drawn at the mean difference, and at the mean difference plus and minus 1.96 times the standard deviation of the differences (dot lines). The particular diagram shows that the discrepancy (bias) between the 2 methods is 4.3 mm Hg, which could be interpreted as being clinically important when measuring IOP in OAG and OHT patients and, consequently, DCT and GAT methods could not be interchangeably used. With the exception of a few cases, DCT readings were higher than those of GAT and in 95% of subjects, the difference lies between 0.3 and 8.4 mm Hg. Furthermore, the Bland & Altman plot reveals a slight trend in the results, where the difference between methods tends to get larger as the average increases.
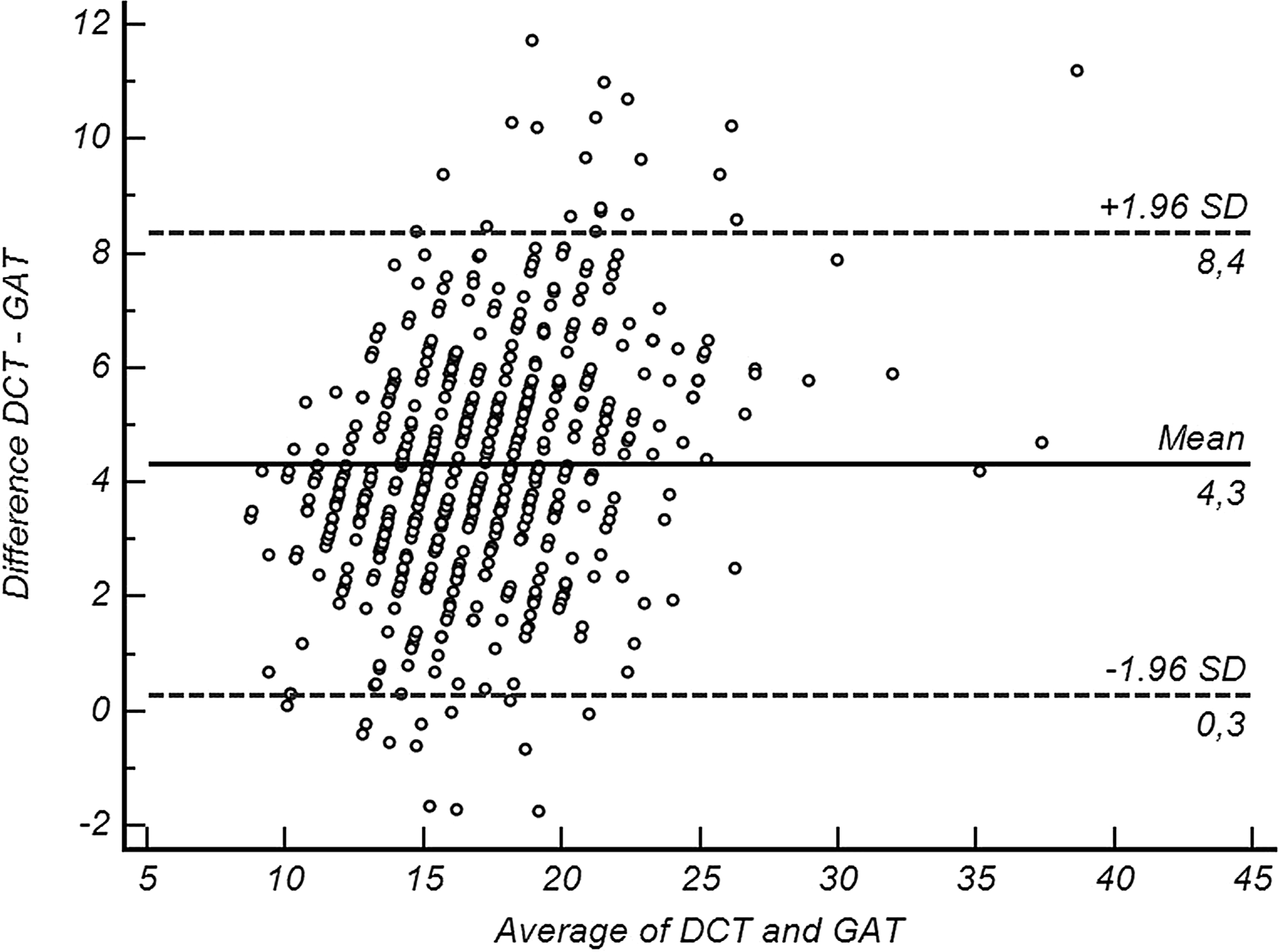
The Bland–Altman plot of the agreement between intraocular pressures (IOPs) measured using dynamic contour tonometry (DCT) and Goldmann applanation tonometry (GAT).
CCT, central cornea thickness; IOP, intraocular pressure; GAT, IOP measured by Goldmann applanation tonometry; DCT, IOP measured by dynamic contour tonometry; ΔIOP, DCT-GAT difference.
The DCT-GAT difference (ΔIOP) did not differ statistically significantly (P=0.49) between the 2 major groups of the study, yielding a mean of 4.26±2.02 mm Hg and 4.41±2.25 mm Hg in the OAG and OHT groups, respectively. The IOP difference between the 2 methods was strongly positively correlated with the DCT readings (r=0.52, P<0.0001) but not with the GAT measurements (r=0.06, P=0.19). From the other parameters measured, CCT (r=0.004 P=0.94), CC (r=0.086, P=0.11), cup-to-disc ratio (CDR, r=−0.016 P=0.75), and spherical equivalent (SEQ, r=−0.039, P=0.43) did not indicate any correlation with ΔIOP. In a multiple regression analysis, none of these factors were found to contribute significantly to the prediction of the DCT-GAT difference (R
2
=0.02, P=0.41). With the same kind of analysis, CDR proved to be the most important factor influencing both DCT (R
2
=0.09, r=−0.287, P<0.001) and GAT (R
2
=0.12, r=−0.336, P<0.001). A statistically significant correlation was proved to exist between the age of the patient and ΔIOP (Spearman's r=−0.125, P=0.011) as well as to DCT and GAT measurements itself. However, the multiple regression model showed that DCT had a much higher statistically significant contribution to the prediction of the DCT-GAT difference than the age of the patient (R
2
=0.27, r
Statistically significant correlations are marked in bold.
CC, corneal curvature; CDR, cup-to-disc ratio; SEQ, spherical equivalent.
Out of the 410 eyes included in the study, 68 received no IOP-lowering therapy, 176 were under eye-drop monotherapy, and 166 received a combined local therapy of 2 or more medications. One-way ANOVA showed that the number of IOP-lowering medications did not have any statistically significant influence on the difference between DCT and GAT measurements (F=1.738, P=0.177). Similar results revealed the nonparametric Kruskal–Wallis analysis of variance for the influence of medication number on DCT (P=0.28) and GAT (P=0.13), respectively. Focusing on the 176 eyes of the monotherapy group, 79 received a prostaglandin analogue (PG), 43 a beta-blocker (BB), 48 received a Carbonic Anhydrase Inhibitor (CAI), and 6 were treated with an a2-agonist (AA). The reason of uneven distribution of medication type is the cross-sectional nature of this particular study. Performing a one-way analysis of variance in a statistically higher ΔIOP was revealed in monotherapy patients receiving CAIs (ΔIOP=5.75 mm Hg) in comparison to patients receiving PGs (ΔIOP=4.09 mm Hg) or BBs (ΔIOP=3.78 mm Hg) as single topical therapy (ANOVA, F=4.373, P=0.005); while both DCT and GAT measurements were statistically significantly lower only in the group of patients receiving AA (F-ratio=3.005, P=0.032 and F-ratio=3.669, P=0.013 respectively). The means±SDs of DCT, GAT, and ΔIOP in each category of monotherapy are demonstrated in Table 3, where the statistical comparison and the respective P-values are also provided. One-way analysis of variance revealed no statistically significant difference in CCT measures between monotherapy patients (CCTPGs=548.7 μm; CCTBBs=542.1 μm; CCTCAIs=549.6 μm; CCTAAs=537.1 μm; p=0.32). In order to strengthen the hypothesis that patients receiving CAIs have a higher ΔIOP, all patients were categorized into 2 groups: those receiving local CAIs as monotherapy or combined therapy (99 eyes) and those not receiving any CAIs at all (311 eyes). Nonparametric Mann–Whitney independent samples test (P=0.0035) showed that eyes treated with CAIs had a significantly greater DCT-GAT difference (ΔIOP=4.83±2.39 mm Hg) than those without CAIs in the therapeutical schema (ΔIOP=4.14±1.96 mm Hg); while DCT and GAT remained unaffected (P=0.72 and P=0.26 respectively). CCT did not differ statistically significantly (Mann–Whitney test, P=0.74) between groups with (CCT=543.1±38.6 μm) and those without CAIs (CCT=544.5±38.2 μm) in topical antiglaucoma treatment.
ANOVA significance levels post-extracting values of AAs due to small sample size.
Statistically significant values (p<0.05) are marked in bold.
PGs, prostaglandin analogs; BBs, beta-blockers; CAIs, Carbonic Anhydrase Inhibitors; AAs, alpha adrenergic agonists; ns, not statistically significant; s, statistically significant.
As previously mentioned, out of all the factors and parameters tested, patients' age and DCT readings were found to have an influence on ΔIOP. DCT was already proved—as shown in Table 3—not to be statistically significantly affected by medication type. No statistically significant difference in patients' age was found between monotherapy groups (Kruskal-Wallis, P=0.13), while patients receiving CAIs were found to be statistically older (72.3±11.3 y.o, Kruskal–Wallis, P=0.003). Since a negative correlation was proved to exist between patients' age and ΔIOP, this result does not weaken our hypothesis and was considered clinically irrelevant.
Discussion
The accurate measurement of IOP is a fundamental parameter in every ophthalmic examination; what is more is the diagnosis and follow-up of glaucoma. Over the past decades, GAT has become the gold standard that is used for the routine measurement of IOP, as the method has proved to be robust and easy to use. However, the accuracy of GAT depends on many factors, including the biomechanical properties of the cornea and the bulbus in general.
Topical instillation of ocular hypotensive medications has been shown to have an effect on many ophthalmic properties other than their IOP-lowering effect. In the present study, we attempted to evaluate the association between various IOP-lowering agents and the difference of IOP measured by the means of DCT and GAT in a population of glaucomatous and hypertensive eyes. Our results imply the fact that CAIs when instilled topically can affect the difference in IOP reading acquired by DCT and GAT, which could be attributed to induced alterations in the ocular biomechanical properties.
In 2005, since Pascal Tonometer and the principles of DCT were introduced by Kanngiesser et al., 6 many studies have been published which compare IOP measurements between DCT and GAT investigating factors that may influence IOP measurement levels in each IOP evaluation technique. Recent studies have showed an established difference in IOP levels measured by DCT and GAT that varies between 0.8 and 4.9 mm Hg and exhibits, in most cases, statistically significantly higher IOP readings using the Pascal tonometer.8–10,13–23,26,27
In the present study, DCT readings were a mean±SD of 4.3±2.1 mm Hg higher than GAT readings (P<0.0001), a difference that is comparable to those reported by other authors.
Since an attempt was made by several authors to clarify the reasons of the difference just mentioned, CCT has been the most widely investigated factor that has been assumed to affect the relationship between DCT and GAT. A review of the literature shows variations from 0.11 mm Hg to 0.71 mm Hg for every 10 μm of CCT change using GAT. 19 According to its function, principle DCT could avoid these limitations, as it is supposed to provoke only minimal corneal distortion during the measurement. 6 Many authors tend to confirm that DCT measurements are independent of CCT.6–8,10,12,14,21 Recent studies claim a significantly lower correlation of CCT with DCT than with GAT.9,11,13,16,19,20,22 With regard to the difference between GAT and DCT in IOP measurements, increased CCT was found to correlate with decreased ΔIOP.13,16,22
While attempting to investigate the role of various factors in the IOP difference mentioned, we did not find any statistically significant effect of the diagnosis type (whether OHT or OAG), CCT, CC, or spherical equivalent on ΔIOP. However, while investigating the possible differences in DCT and GAT readings between OHT and OAG groups, one should always keep in mind that OHT patients of the study were found to be a mean of 5.2 years “older” than OAG patients, a fact that could affect the interpretation of the results as a statistically significant correlation was proved to exist between the age of the patient and ΔIOP in the present study. Similarly, the CCT was found to be almost 20 μm thinner in the OAG group as compared with the OHT one, as expected. It is well established that DCT readings are less dependent of CCT than GAT due to their principle of use. 6 However, in the particular study, alterations observed in CCT did not prove to influence the DCT-GAT difference.
Seven carbonic anhydrase (CA) isozymes have been identified in humans and types I, II, and IV have been detected in ocular tissues, such as the nonpigmented epithelial cells of the ciliary body, the cornea, the lens, the retina, and the choroid. By inhibiting the type II CA-dependent step of aqueous humor secretion by the ciliary body, CAIs suppress aqueous humor production, resulting in IOP decrease. Therefore, in the past decade, CAIs were widely used to lower IOP. Besides their IOP-regulating effect, CAIs have been proposed to affect other ocular functions as well, as CA II is present in many ocular tissues, and their influence on ocular rigidity still remains controversial. Ocular rigidity is mainly influenced by scleral and corneal properties and, to some extent, by the choroidal blood flow. High mean arterial pressure and ocular perfusion pressure have been linked to increased ocular rigidity. 28 Hence, treatment with CAIs could affect, to some degree, ocular rigidity by altering ocular perfusion pressure through lowering IOP and increasing the choroidal volume. The effect of dorzolamide on corneal endothelial function has been investigated by Egan et al., who demonstrated an increased endothelial permeability and lower endothelial cell density in eyes after the acute administration of the CAI mentioned earlier. 30
A different explanation of the results is the influence of CAIs, which may cause a significant decrease of tear production. Surface property may also lead to the underestimation of IOP with the Goldmann tonometer. Based on this hypothesis part of the IOP-lowering effect of CAIs, there could be a kind of “pseudo-IOP reduction,” which depends on the affecting ocular surface. 31
To our knowledge, this is the first study that assesses the association of various ocular hypotensive medication types and the DCT-GAT IOP difference. In previous studies that evaluated the effect of glaucoma on ocular rigidity, Hommer et al. reported increased ocular rigidity in patients with POAG based on measurements using pneumotonometry and laser interferometry, 32 and Ebneter et al. demonstrated increased ocular rigidity in patients with established glaucoma compared with control subjects, assessing the correlation between AL changes and IOP changes using DCT. 33 While investigating the effect of topical prostaglandine analogs on glaucoma and nonglaucoma subjects, Detorakis et al. showed a higher ΔIOP in glaucoma patients treated with latanoprost in comparison to normal controls and glaucoma patients receiving other IOP-lowering medication, a finding that was attributed by the authors to possible induced alterations in the biomechanical properties of the ocular walls. 27 However, the study did not differentiate between different ocular hypotensive agents that focused mostly on the effect of latanoprost on DCT-GAT difference. In a recently published study, Wang et al. investigated various factors that could affect the difference in IOP readings between DCT and GAT, reporting a positive correlation of ΔIOP to the axial length and a negative one to the corneal hysteresis. 34 Although normal, hypertensive, and glaucomatous eyes were included in the study, the authors do not mention whether glaucoma patients were under IOP-lowering treatment, a factor that was not included in the analysis.
The outcomes of the present study demonstrated that the topical instillation of CAIs resulted in higher differences in IOP readings between DCT and GAT in comparison to prostaglandin analogs and β-blockers. This statistically significantly higher ΔIOP was noted not only in eyes treated with a single ocular hypotensive agent but also in combined therapies, including a CAI; while DCT and GAT measurements remained unaffected by both treatment group and diagnosis. The combined therapies mentioned earlier, including CAIs, and used in the study are currently available in the Swiss market fixed combination of dorzolamide hydrochloride with timolol maleate (Cosopt®, Merck), the fixed combination of brinzolamide with timolol maleate (Azarga®, Alcon Laboratoires, Inc.), and the unfixed combination of each of the already mentioned or simple dorzolamide/brinzolamide (Trusopt®, Merck/Azopt®, Alcon Laboratoires, Inc.) to any other commercially available ocular hypotensive medication such as beta blockers, alpha agonists, or prostaglandin analogues. The only factors which tended to correlate to that higher difference were age and DCT. No statistically significant difference with regard to patients' age was found between monotherapy groups, while patients receiving CAIs in comparison to those not receiving any CAI were found to be statistically older. Since a negative correlation was proved to exist between patients' age and DCT-GAT difference, this result does not weaken our hypothesis. Taking into account the lack of intergroup differences in all the other parameters tested, we conclude that the differences found in ΔIOP could be mostly attributed to the effect of CAIs on the ocular rigidity and other biomechanical properties of the sclera and the cornea rather than to glaucomatous or other changes.
The cross-sectional nature of the study—resulting in an uneven distribution of ocular hypotensive medication type—reflects the major limitations of the study. Furthermore, we did not include axial length in our statistical analysis, a factor that has been previously shown to correlate with ΔIOP. In addition, the duration of ocular hypotensive treatment that could possibly induce changes in ocular rigidity was not available in the particular study to be used as an additional related factor. However, the prospective nature and the lack of inter-examiner variability due to all measurements being performed by a single experienced operator strengthen the power of the present study. Further randomized studies conducted on the treatment of naive eyes should be performed to investigate the influence of topical instillation of CAIs on ocular rigidity and the other ocular biomechanical properties in order to better understand the role of ocular hypotensive agents in the difference of IOP readings between DCT and GAT in glaucomatous and ocular hypertensive eyes.
Footnotes
Author Disclosure Statement
The authors have no proprietary interest in any of the products mentioned in the study. No financial grants or funds have been received in support of the study. The study was performed with informed consent and following all the guidelines for experimental investigations required by the Institutional Review Board of the Ethics Committee to which all the authors are affiliated.