
Abstract
Abstract
Purpose:
To compare the effects of straight, oblique, and double-plane tunnel scleral intravitreal injection techniques, on short-term intraocular pressure (IOP) changes, occurrence of vitreous reflux (VR), and/or other complications.
Methods:
A total of 105 patients were included in this prospective study. Patients were assigned randomly to one of the straight injection group (SI; n=35), oblique injection group (OI; n=35), or double-plane tunnel injection group (DPTI; n=35). The occurrence of VR and preinjection and postinjection IOP at 2 and 6 h were compared between groups, and complications were assessed.
Results:
The mean patient age was 71.1±6.6 years (range 58 to 86 years; 50 women and 55 men). In the SI, OI, and DPTI groups, VR occurred in 18 (51.4%), 12 (34.3%), and 6 patients (17.1%), respectively. Mean preinjection IOPs were 15.4, 14.8, and 15.6 mmHg, and changed to 17.3, 18.0, and 20.0 mmHg at the second hour, and 15.7, 16.2, and 16.1 mmHg at the sixth hour, respectively. No significant differences among the groups were found in terms of complications such as transient mild uveitis or subconjunctival hemorrhage.
Conclusion:
Double-plane tunnel injection prevents VR from the injection site and has no additional complications than other techniques.
Introduction
Age-related macular degeneration (AMD) is one of the leading causes of irreversible vision loss among the old population.7–9 Most of the patients with exudative AMD experience rapid loss of central vision in a short time period. 10 Several treatment modalities were used for the treatment of exudative AMD; however, a complete remission for this devastating disease has not been achieved.9,11–18 Since the introduction of anti-VEGF agents such as pegaptanib, bevacizumab, and ranibizumab, it has been possible to achieve a significant gain in visual acuity and to treat the exudative AMD.16–18 The use of these agents continues to become more widespread, as they provide beneficial results for diseases such as retinal vein occlusion, diabetic macular edema, and neovascular glaucoma.4–6
Intravitreal administration of these agents is accepted as a safe intervention; few complications have been reported despite the great number of injections.2–6 Short-term intraocular pressure (IOP) increases after injection of anti-VEGF agents and quickly normalizes within 30 min.19–23 Benz et al. 20 found an inverse correlation between the increase of postinjection IOP and the presence of reflux. Lopez-Guajardo et al. 24 demonstrated that the reflux at the site of injection contains not only vitreous but also injected intravitreal agent. Several strategies such as tunneled injection technique and Honan IOP reducer have been proposed to preserve the therapeutic effect of a small amount of intravitreally delivered agent while reducing or eliminating the reflux.19–21,24,25 Prevention of reflux may minimize the loss of injected intravitreal agent, as well as the risk of endophthalmitis. In this study, we compared the reflux rates and changes in IOP after the administration of 0.05 mL anti-VEGF treatment for 3 injection techniques: straight injection (SI), oblique injection (OI), and double-plane tunnel injection (DPTI).
Methods
This is a prospective, interventional, randomized study that evaluates the 105 eyes of 105 consecutive patients who were previously found to have AMD. The study was approved by the local ethics committee and was conducted in accordance with the ethical standards set in the 1964 Declaration of Helsinki, as renewed in 2000. Written informed consent was received from all patients after explaining the application, potential risks, and benefits of the 3 different procedures. Eligible patients were randomly assigned to one of the injection groups. All injections were performed by the same surgeon (A.O.). Patients with a history of glaucoma, intraocular hypertension, or previous vitreoretinal surgery were not included. IOP was measured by slit-lamp-mounted Goldmann applanation tonometry in a sitting position. Baseline IOP measurements were performed between 8:00 and 9:30 AM. The interval between baseline IOP measurement and injection was from 0 to 15 min. The second- and sixth-hour IOP measurements were performed 2 and 6 h after the injection for each patient.
All injections were performed under the same sterile condition. The injection was performed in an outpatient operation room via operation microscope. After application of 0.05% proparacaine hydrochloride eye drops topically 3 times every 5 min for anesthesia, the periocular skin was cleaned with 10% povidone iodine; the eye was draped with an eye towel and plastic adhesive drape; the conjunctival sac was irrigated with 5% povidone iodine; the eye was opened with a lid retractor; and the drug was injected through pars plana (3.5 mm posterior to the limbus) via a 30-gauge needle on a 1-mL syringe. All patients received 0.05 mL anti-VEGF (Ranibizumab, Lucentis©; Genentech/Novartis) treatment.
In the SI, after mobilization of the conjunctiva, a 30-gauge needle was inserted into the vitreous cavity; the sclera was penetrated at an angle of 90° 3.5 mm behind the limbus through temporal the pars plana; and the needle was withdrawn at the same angle (Fig. 1A). In the OI, after mobilization of the conjunctiva, a 30-gauge needle was inserted into the vitreous cavity; the sclera was penetrated at an angle of 45°–60° 3.5 mm behind the limbus through temporal the pars plana; and the needle was withdrawn at the same angle (Fig. 1B). In the DPTI, after mobilization of the conjunctiva, a 30-gauge needle was inserted into the vitreous cavity; the sclera was penetrated at an angle of 15°–30°, and then the needle was repositioned at an angle of 45°–60° toward the center of the globe 3.5 mm behind the limbus through temporal the pars plana, and followed by injection of the drug, the needle was withdrawn at an angle of 90° (Fig. 1C).
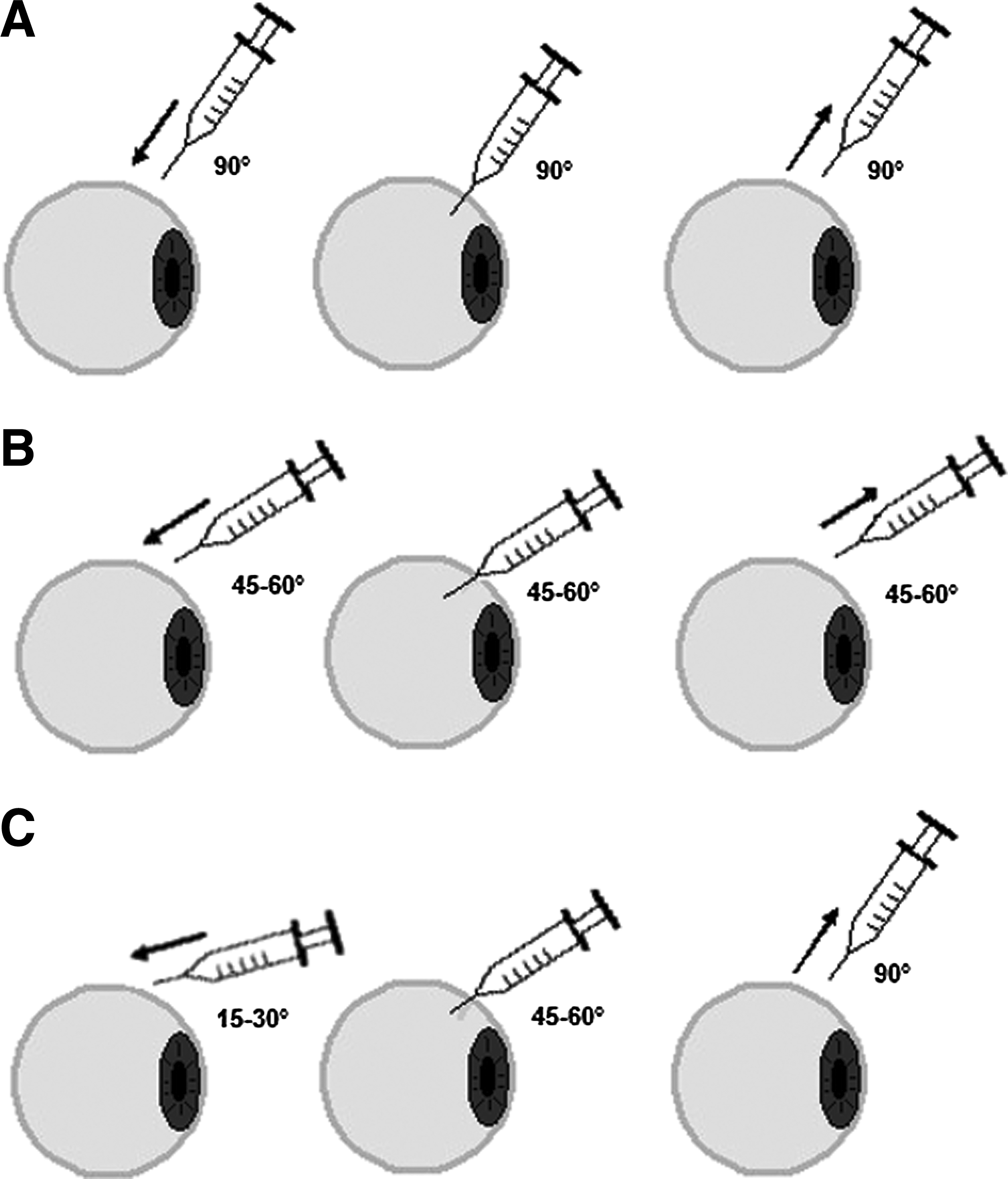
Demonstration of there intravitreal injections; straight injection group
For all injections, a cotton tip was placed over the sclera for 10 s immediately after needle removal. Subsequently, the cotton tip was removed, and the incision site was observed for reflux via operation microscope. If any subconjunctival bleb was observed, the injection was determined as reflux positive. After the procedure, an ophthalmic solution of moxifloxacin was administered 5 times a day for 1 week.
The main outcome measures were the occurrence rate of vitreous reflux (VR) after the injection, the IOP change between baseline, second and sixth hours after injection, and complication rates.
Statistical analyses were performed via SPSS 16.0 software (SPSS, Inc., Chicago, IL). Comparisons between baseline, second-, and sixth-hour IOPs for each group were analyzed using the Wilcoxon test. Chi-square test was performed to test the significance of the differences between baseline and second-hour or sixth-hour IOP measurements among the groups. A P value <0.05 was considered statistically significant. The chi-square test was used to compare the reflux rates among the groups. Correlations between postinjection IOP changes and reflux rates were assessed via Spearman’s test.
Results
A total of 105 patients were enrolled for this study. None of the patients were excluded during the study period. The overall mean age was 71.1±6.6 (between 58 to 86 years); 55 patients were (52.4%) men, and 50 patients were (47.6%) women. All of the patients received intravitreal ranibizumab for the treatment of exudative AMD. Table 1 shows the general characteristics of the patients in the 3 injection groups. Mean baseline IOP was 15.4±2.7 mmHg (between 10–20 mmHg) in the SI group, 14.8±2.9 mmHg (between 8–20 mmHg) in the OI group, and 15.6±2.6 mmHg (between 10–20 mmHg) in the DPTI group. There was no statistically significant difference between the groups (P=0.555). IOP differences in the SI, OI, and DPTI groups between baseline and the second hour after the injection were 1.8±1.9 mmHg (P<0.001), 3.17±2.5 mmHg (P<0.001), and 4.3±2.5 mmHg (P<0.001), respectively. Although statistical analysis revealed a significant difference between the SI and DPTI groups (P=0.001), there was neither significant difference between the SI and OI groups (P=0.383), nor between the OI and DPTI groups (P=0.222). IOP differences between baseline and the sixth hour in the SI, OI, and DPTI groups were 0.3±1.2 mmHg (P=0.368), 1.4±1.5 mmHg (P<0.001), and 0.4±1.5 mmHg (P=0.038), respectively. There was no statistically significant difference between the groups (SI-OI, P=0.201; SI-DPTI, P=0.703; and OI-DPTI, P=0.154).
SI, straight injection group; OI, oblique injection group; DPTI, double-plane-beveled tunnel injection group.
Overall reflux rate was 34.3% (36 of 105 patients). In the SI, OI, and DPTI groups, the reflux rates were 51.4%, 34.3%, and 17.1%, respectively. There was a statistically significant difference between the SI and DPTI groups (P=0.004) and, the OI and DPTI groups (P=0.044). However, there was no statistically significant difference between the SI and OI groups (P=0.304). There was a strong correlation between IOP differences from baseline to the second hour and reflux rates in the DPTI group (r=0.387, P=0.002). Table 2 shows IOP measurements and reflux rates of the patients.
Chi-square test, P value <0.05 was considered statistically significant.
Wilcoxon test, P value <0.05 was considered statistically significant.
IOP, intraocular pressure.
The complication rates between the groups were similar, and no severe complications were diagnosed. Mild-persistent anterior uveitis and subconjunctival hemorrhage were detected in the groups (Table 1).
Discussion
Several factors may be involved in VR, such as patient-related factors, including baseline IOP, scleral thickness, and degree of vitreous liquefaction, as well as injection-related factors, including injection volume, speed, and technique.19–28 Saeed et al. 26 showed that reflux is not related with phakic status or posterior vitreous detachment, but appears to be affected by age. Rodrigues et al. 27 found that the size of the needle has a significant impact on reflux when performing a straight injection. This result suggests that injection technique has a major influence on reflux rates.
Rodrigues et al. 27 found that 44.4% of the patients showed reflux after the intravitreal injection of bevacizumab via 26-, 27-, 29-, and 30-gauge needles. Total or partial straight incisions caused greater reflux compared to tunneled incisions. There was no difference in reflux rates between the 3 different tunneled incisions among the groups that were used in the study. Höhn et al. 21 reported that 46.5% of the patients had some degrees of reflux after the intravitreal injection of 0.05 mL ranibizumab; however, in our study, 34.2% of the patients experienced reflux. Reflux was noted in only 7.1% of the eyes in the tunneled injection group, whereas the rate was 61.2% in the SI group. In our study, reflux was less frequent in tunneled injection than both in straight and oblique injections. The source of the difference in the reflux rates between the studies may be explained by differences in the composition, in the injection techniques, and the size of the subgroups.
Previous studies that examined IOP after the injection demonstrated that IOP increases quickly immediately after injection, followed by a slow decrease.19,20 IOP returns to normal values within 15–30 min after the injection. However, the relationship between VR and IOP levels 2 h after injection was not mentioned in previous studies. This study is the first to show an inverse relationship between second-hour IOP levels and reflux rates. Hollands et al. 19 demonstrated that differences in IOP normalization time were dependent on the highest IOP values that reached immediately after intravitreal injection. In addition, Höhn et al. 21 found that the postinjection IOP level was related to intravitreal injection technique and was higher in tunneled injection technique. Höhn et al. 21 also revealed that the normalization of IOP after injection required more time in patients who underwent tunneled intravitreal injection. We found similar results to those in previous studies: the IOP increase was statistically higher in the DPTI group than both of the SI and OI groups. Unlike in most previous studies, IOP levels in the DPTI group remained elevated until 2 h after injection. In addition, all patients showed normalization of IOP at the sixth hour after the injection.
It still remains to be determined whether reflux clinically impacts drug efficacy or the safety of intravitreal injections. The relationship between the VR bleb and the volume of the drug loss after intravitreal injections should be determined as well. Moreover, the VR itself may carry a low risk of retinal complications such as retinal tears or detachments resulting from vitreoretinal traction formation. In an anterior segment optical coherence study, it was showed that fine channels persisted at the injection site for 20 min after injection in patients who underwent a straight injection. 28 Theoretically, vitreous incarceration within a scleral wound may act as a conduit for the entry of bacteria into the globe.
No serious complications such as endophthalmitis, vitreous hemorrhage, severe uveitis, or retinal detachment were detected related to injection in this study. Self-limiting complications such as mild anterior chamber reactions and subconjunctival hemorrhages were observed.
In this study, age, baseline IOP level, injection volume, injected drug, and needle size were similar between the groups. However, scleral thickness, degree of vitreous liquefaction, and injection speed were not evaluated. In addition, we did not quantify the VR and contents of the reflux (drug/vitreus ratio), and these factors were the limitations of this study.
In conclusion, DPTI provides significantly lower VR rates when compared with the SI and OI techniques. Higher postinjection IOP levels in the DPTI group were explained by lower incidence of VR. It seems that preventing the VR is an important issue, to deliver the maximum amount of drug into the eye, and DPTI may be an ideal technique. However, further studies are needed with larger groups on intravitreal injected drug efficacy.
Footnotes
Acknowledgments
This prospective study was not supported by any of the company. None of the other authors has financial or proprietary interests in any material or method mentioned. These data have not been previously published. Institutional review board approval from Beyoglu Training and Research Eye Hospital, Istanbul, was obtained for this study.
Authors' Contributions
A.O. and Z.A.: Involved in design and conduct of the study; A.O., Z.A., and U.C.: preparation and review of the study; A.O. and Z.A.: data collection; and Z.A.: statistical analysis.
Author Disclosure Statement
No competing financial interests exist.