
Abstract
Abstract
Purpose:
The development of endophthalmitis after cataract surgery often results in significant vision loss. Inhibition of bacterial proliferation in the anterior chamber using antibiotic eye drops is important to prevent endophthalmitis after cataract surgery. We aimed to determine the sensitivity of fluoroquinolones against Enterococcus faecalis ocular isolates and the efficacy of fluoroquinolones to prevent E. faecalis-induced endophthalmitis in aphakic rabbits.
Methods:
The minimum inhibitory concentrations (MICs) of moxifloxacin (MFLX) and levofloxacin (LVFX) used in ophthalmic solutions for 13 E. faecalis isolates obtained from the conjunctival sac or endophthalmitis cases were determined. Eye drops containing MFLX (0.5%), LVFX (0.5%), or saline were administered to aphakic rabbits with endophthalmitis induced by E. faecalis. The eye drops were administered immediately after lensectomy and at 3 and 6 h after cataract surgery (early instillation group) or immediately after lensectomy and at 12 and 15 h after cataract surgery (delayed instillation group). Bacterial growth, electroretinography (ERG), and slit-lamp examination (SLE) were determined throughout the course of infection.
Results:
In vitro susceptibility testing revealed that the MICs of MFLX for E. faecalis isolates were lower than those of LVFX. In the early ocular instillation groups, MFLX significantly improved SLE scores, ERG, and viable bacterial counts compared with LVFX and saline (all, P<0.05). There were no significant differences in any parameter between MFLX and saline in the delayed ocular instillation groups.
Conclusions:
Early ocular instillation of MFLX delays retinal damage compared with LVFX when used to treat E. faecalis-induced endophthalmitis after cataract surgery.
Introduction
Pre- and postoperative prophylaxis is widely performed to prevent endophthalmitis. 3 Antibiotics could inhibit bacterial proliferation after cataract surgery and prevent endophthalmitis. Several reports have shown that intracameral antibiotics are effective for the prevention of endophthalmitis.4,5 Antibiotic eye drops and intracameral antibiotics are often used for the prevention of endophthalmitis. Generally, antibiotics are administered immediately after surgery and on the following day as postoperative prophylaxis for endophthalmitis. Wallin et al. reported that starting topical antibiotic administration on the day after surgery, rather than on the day of surgery, was associated with increased risk of endophthalmitis. 6 These results suggest that bacteria proliferate and express virulence factors as early as 1 day after surgery. Indeed, Wada et al. reported that immediate postoperative prophylaxis reduced the risk of Enterococcus faecalis endophthalmitis. 7 To date, however, no study has examined the effects of antibiotic administration on tissue damage associated with endophthalmitis, or the optimal timing of administration.
In our previous study, we established an aphakic rabbit model of endophthalmitis that accurately reflects postoperative endophthalmitis in clinical settings. 8 The model is established by inoculating pathogens into the lens capsule and anterior chamber after lensectomy. In this model, E. faecalis shows a high growth rate in the eye (1×109 colony forming unit [CFU]/mL within 3–7 h). The infected iris is partially covered with fibrin and/or hypopyon after 12 h, and none of the pupil is visible after 24 h because of inflammation. Microscopic analysis confirmed the presence of bacteria on the lens and bacterial migration to the vitreous, while electroretinographic (ERG) analysis confirmed the development of severe functional damage to the eye at 48 h because of the bacterial infection. Thus, this model is consistent with clinical postoperative endophthalmitis, and allows us to evaluate the efficacy of various treatments/procedures.
In this context, the first aim of this study was to compare the antimicrobial activities of 2 antibiotic fluoroquinolones [moxifloxacin (MLFX) and levofloxacin (LVFX)] against E. faecalis isolates. Our second aim was to examine, in vivo, the efficacy of MLFX and LVFX against E. faecalis in terms of visual outcomes. Our third aim was to compare the effects of different starting times of antibiotic administration on retinal damage.
Methods
Bacteria
We obtained a laboratory strain of E. faecalis OG1S, which produces a secretory protease, and 13 clinical isolates (10 isolates from conjunctivitis cases and 3 isolates from endophthalmitis cases from Ehime University Hospital). The bacteria were grown in a brain–heart infusion broth (Difco Laboratories, Detroit, MI) for 18 h at 37°C, and then washed twice with and resuspended in sterile physiological saline. The concentration of bacteria in the suspension was determined spectrophotometrically and adjusted to ∼2×105 CFU/mL with sterile physiological saline.
Antibiotics
MFLX 0.5% ophthalmic solution (Vigamox®; Alcon Japan Ltd., Tokyo, Japan) and LVFX 0.5% ophthalmic solution (Cravit®; Santen Pharmaceutical Co. Ltd., Osaka, Japan) were purchased from their respective manufacturers.
Susceptibility tests
In vitro susceptibility tests were conducted by a commercial laboratory (Mitsubishi Chemical Medience Corp., Tokyo, Japan) to determine the minimum inhibitory concentration (MIC) of each antibiotic in accordance with the Clinical and Laboratory Standards Institute (CLSI) recommendations for antimicrobial susceptibility testing. 9 All strains were tested for antimicrobial susceptibility by the broth microdilution method using microdilution panels and broth reagents from Eiken Chemical Co. Ltd. (Tokyo, Japan). Cation-adjusted Mueller Hinton broth was used in these experiments. The MICs were recorded as the lowest concentration that inhibited visible growth. The range of MICs and the MICs at which 50% or 90% of the isolates are inhibited (MIC50 and MIC90, respectively) are shown.
Animal model and drug administration
Experimental endophthalmitis was induced in Japanese albino rabbits (1.6–2.4 kg; Kitayama Labs Co. Ltd., Ina, Japan) by inoculating E. faecalis, as previously described. 8 Briefly, lensectomy was performed on the rabbit's left eye by phacoemulsification (Black Max, Advanced Medical Optics, Santa Ana, CA). After lensectomy, the corneal incision was closed with 10-0 nylon sutures to prevent any leakage. Then, using a 27-gauge blunt needle, the eyes were inoculated from a capsular bag containing 0.1 mL of the E. faecalis OG1S strain (5.21±0.29 log10 CFU/mL) or sterile physiological saline as a control. The rabbits (n=50) were then divided into 5 groups and treated with MFLX, LVFX, or saline, as described in Table 1. To compare in vivo antimicrobial activities between fluoroquinolones, we used commercially available eye drops containing the same concentrations of active drug (i.e., 0.5% MFLX and 0.5% LVFX). To limit the number of animals used and considering the limited efficacy of LVFX, we did not establish a delayed LVFX group. Animals in which the study drug was not administered correctly were excluded from the analysis.
MFLX, moxifloxacin; LVFX, levofloxacin.
The study protocols conformed to the Institutional Animal Care and Use Committee guidelines and the Association for Research in Vision and Ophthalmology Statement for the Use of Laboratory Animals in Ophthalmic and Vision Research. All procedures involving rabbits were approved by the Committee of Animal Experimentation, Ehime University School of Medicine.
Intraocular inflammation score
Inoculated eyes were evaluated at 6, 12, 24, and 48 h after surgery by slit-lamp biomicroscopy (Topcon SL-14; Kogaku Kikai, Tokyo, Japan). The investigators, who were blinded to the treatment, graded intraocular inflammation using the following scores: 0, normal; 1, a small amount of fibrin on the pupil; 2, the iris is partially covered with fibrin and/or hypopyon; 3, the iris is covered with fibrin and/or hypopyon; 4, the pupil is not visible.
Bacterial counts
The eyes were removed at 48 h after inoculation, and the E. faecalis bacterial counts in ocular tissues were determined. The surface of the enucleated globe was cleaned with ethanol using a cotton swab and then rinsed with sterile physiological saline. The aqueous humor was collected with a 23-gauge needle. The cornea was removed aseptically, and the contents of the anterior chamber (fibrin and hypopyon) were collected and mixed with the aqueous humor. The iris and lens were dissected away, and the surface of the vitreous body was rinsed with sterile physiological saline. The vitreous was then collected. Bacterial counts in the anterior chamber or the vitreous were determined by plating serial dilutions on a brain–heart infusion agar. 8
Retinal responsiveness
The degree of postoperative retinal function was evaluated by recording the scotopic b-wave amplitude for each eye by flash ERG (LE-3000; Tomey Corp., Nagoya, Japan) at 12, 24, and 48 h postinoculation. 8 Acute and permanent damage was assessed at each of these times. Retinal function was determined as the b-wave amplitude for the experimental eye, expressed as a percentage of that in the contralateral control eye.
Histology
Both eyes of each rabbit were removed at 48 h. Globes were fixed in phosphate-buffered 10% formalin solution for 24 h. Eyes (n=4 per group) were sectioned and stained with hematoxylin and eosin. 8 Retinal damage was examined by light microscopy (BX50; Olympus, Tokyo, Japan). Each eye was checked to confirm whether the 5 retinal layers were intact.
Statistical analysis
Mann–Whitney tests were used to compare intraocular inflammation scores and changes in retinal responsiveness between the MFLX and control groups in both regimens. Tukey–Kramer tests were used to compare outcomes between the 2 ocular formulations and the control group. Values of P<0.05 were considered statistically significant. Values are shown as means±standard deviation of 6–10 eyes per group.
Results
In vitro antibacterial activity
The 50% and 90% MICs of MFLX and LVFX against E. faecalis isolates are shown in Table 2. Because the MICs of MFLX and LVFX against some strains were high, the ranges of MIC values were wide. However, MFLX showed excellent activity against most of the strains, except for the highly resistant strains. Based on the 50% MICs, MFLX was the most active agent against E. faecalis isolates, being 8-fold more active than LVFX. The MICs of MFLX and LVFX against OG1S were 0.5 and 2.0 μg/mL, respectively.
50% and 90%, MICs for 50% and 90% of the isolates tested, respectively.
MICs, minimum inhibitory concentrations.
Intraocular inflammation score
Using our established endophthalmitis rabbit model, we infected the lenses of the rabbits with E. faecalis and then treated them with 1 of 5 eye drop regimens: early MFLX, delayed MFLX, early LVFX, early saline (control), or delayed saline (control) (Table 1). The eyes were then examined at the designated times to assess intraocular inflammation scores (Fig. 1 and Table 3). At endpoint (i.e., 48 h), the mean score in the early MFLX group (2.3±0.95) was significantly lower than those in the control groups (early control: 3.6±0.52, P<0.01; delayed control: 3.4±0.97, P<0.01) and the delayed MFLX group (3.5±0.76; P<0.05). The intraocular inflammation score in the early MFLX group was also significantly lower than that in the LVFX group (3.3±0.95; P<0.05). There were no differences between the LVFX and control groups.
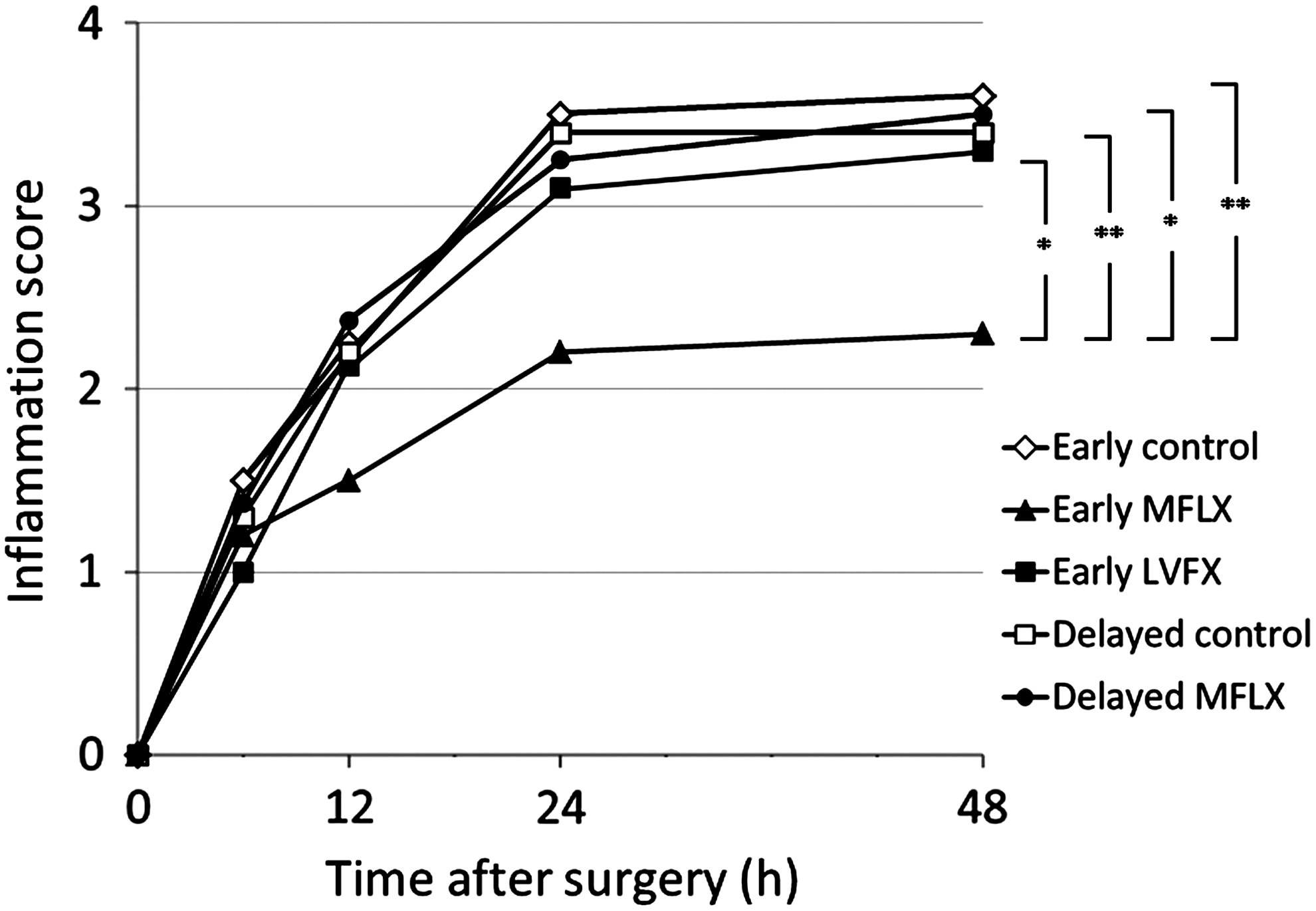
Intraocular inflammation scores at the specified times after surgery and inducing Enterococcus faecalis endophthalmitis. Data are means (n=10). MFLX, moxifloxacin; LVFX, levofloxacin; *P<0.05; **P<0.01.
Bacterial counts
Inhibition of bacterial growth in the anterior chamber was assessed. Inhibition of bacterial growth was not significantly different between the early MFLX group (3.4±2.2 log10 CFU/mL; n=6) and the control (5.3±1.2 log10 CFU/mL; n=6; P=0.17) or early LVFX (4.9±0.6 log10 CFU/mL; n=6; P=0.23) groups (Fig. 2). The bacterial count in the delayed MFLX group (3.2±2.2 log10 CFU/mL; n=8; P=1.0) was similar to that in the early MFLX group.

Effects of topical MFLX and LVFX on the bacterial count in the anterior chamber (left) and vitreous (right). Data are means±standard deviation (n=6–8). *P<0.05.
In the vitreous, bacterial growth in the early MFLX group (5.3±2.0 log10 CFU/mL; n=6) was significantly reduced compared with that in the control group (7.3±0.8 log10 CFU/mL; n=6; P<0.05). Bacterial counts were also lower in the early MFLX group compared with those in the delayed MFLX (6.4±1.5 log10 CFU/mL; n=8; P=0.40) and early LVFX (7.1±0.7 log10 CFU/mL; n=6; P=0.09) groups, although these differences were not statistically significant.
Retinal responsiveness
The retinal responsiveness of eyes infected with E. faecalis was determined by ERG analysis (Fig. 3). Retinal function at 48 h was significantly greater in the early MFLX group (responsiveness level 89.3%±40.3%) compared with the early control (16.7%±8.6%; P<0.001), delayed MFLX (52.2%±42.8%; P<0.05), and early LVFX (41.1%±41.7%; P<0.05) groups.

Effects of topical MFLX and LVFX on electroretinographic measurements of retinal responsiveness at the specified times after surgery and inducing E. faecalis endophthalmitis. Data are means (n=10). *P<0.05; **P<0.001.
Histological examination
Stained retinas from the eyes of rabbits infected with E. faecalis were examined by light microscopy. Samples from the control group showed disruption of the retinal layers with abundant inflammatory cells, and that the photoreceptors could not be observed (Fig. 4A). The retinal layers in the early MFLX groups were intact and had a normal appearance (Fig. 4B). Although the retinal layers in the early LVFX group were almost intact, the photoreceptors were destroyed, and there were fewer cells in the outer nuclear layer (Fig. 4C). Similar observations were found in all of the samples from each group.
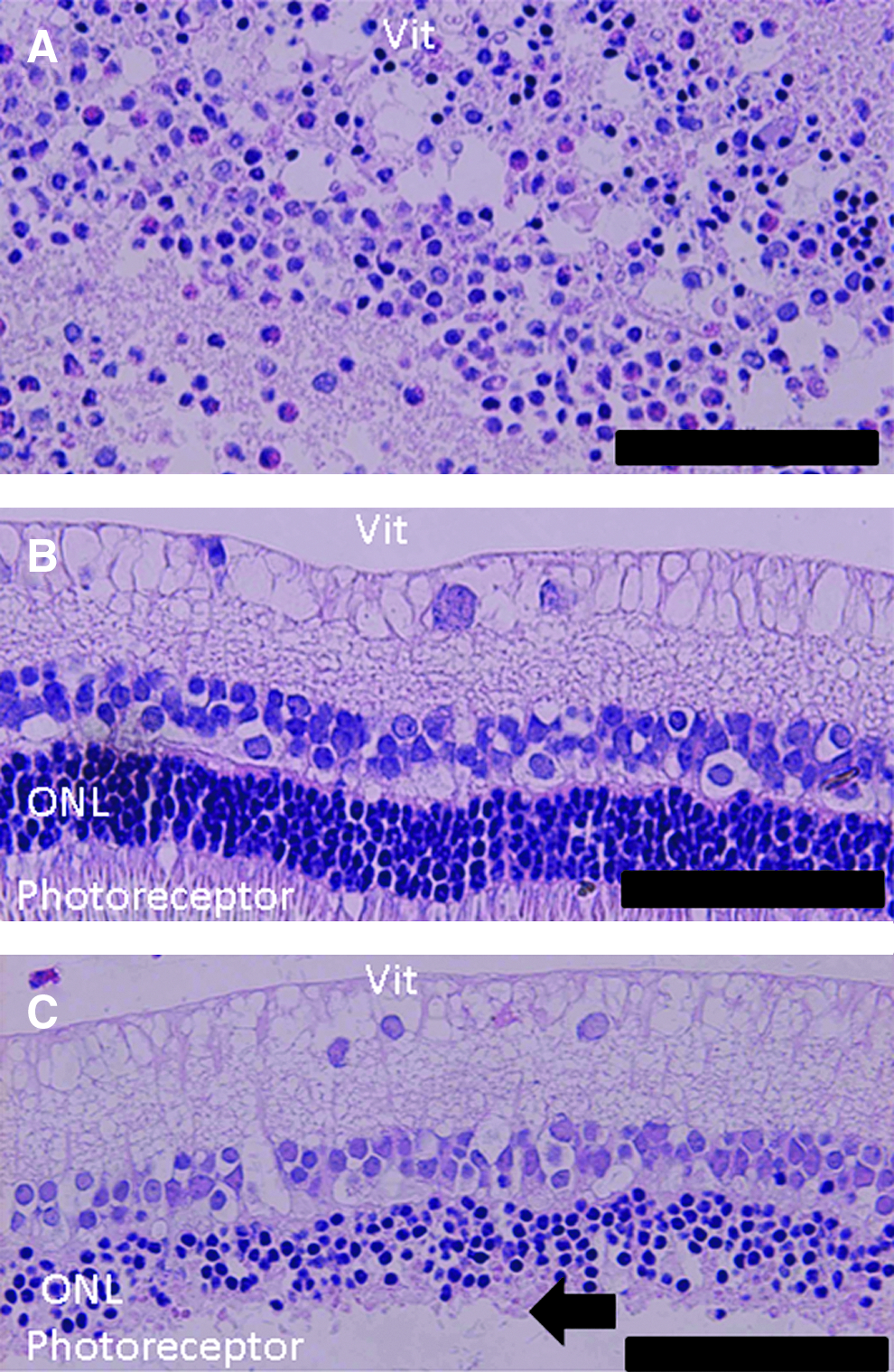
Representative hematoxylin-and-eosin-stained retina tissue sections in the early saline
Discussion
The causative agents of endophthalmitis and their pathogenic potentials need to be identified to determine visual prognosis, and to guide treatment decisions. The Endophthalmitis Vitrectomy Study Group identified several causative agents, the most common being gram-positive, coagulase-negative staphylococci (CNS) (70.0%), Staphylococcus aureus (9.9%), Streptococcus species (9.0%), and Enterococcus species (2.2%), as well as other gram-negative (5.9%) and gram-positive (3.1%) species.10,11
Although CNS are among the most common causative bacteria, they do not produce strong toxins or proteases that damage ocular tissue, offering good visual prognosis. These properties of CNS may explain the significantly better visual outcomes in patients with CNS infection than in patients infected with other organisms.10,12
E. faecalis is a commensal bacterium present in the gastrointestinal flora and causes many infectious diseases, including endocarditis. 13 It can rapidly induce postoperative endophthalmitis, often within 2–4 days, 14 and can cause substantial vision loss upon infection.13,15,16 Notably, patients with E. faecalis-related endophthalmitis had the worst visual outcome in the Endophthalmitis Vitrectomy Study. 10
Several studies have since examined the contribution of enterococcal virulence factors to the pathogenesis of E. faecalis endophthalmitis.17–19 We recently demonstrated that proteases secreted from E. faecalis, such as gelatinase and serine protease, play important roles in the development of endophthalmitis in aphakic eyes after cataract surgery. 8 These proteases seem to promote the spread of organisms by penetrating the posterior lens capsule, allowing the bacteria to migrate from the anterior chamber to the posterior chamber. This migration is a key event in the progression of postoperative endophthalmitis and the consequent severe retinal damage. In Japan, E. faecalis is the causative agent in 12.2% of all ocular infections, 20 which is more than 6-fold higher than the rate reported in the United States. 11 E. faecalis also has a high growth rate in vitro (1×109 CFU/mL within 3–7 h). 14
Considering these properties of E. faecalis, particularly its potent enzymatic activity, infection with this pathogen could rapidly progress to severe visual complications if the infection is not treated promptly and efficiently. Administration of antibiotic eye drops early in the infective course, or even prophylactically before infection develops, may help prevent E. faecalis infection and its complications, thereby reducing the risk of postoperative vision loss.
In this study, early postoperative MFLX administration (i.e., at 0, 3, and 6 h after surgery) achieved greater reductions in the inflammation score and bacterial count in the vitreous compared with delayed administration (i.e., at 0, 12, and 15 h after surgery). We also found that postoperative MFLX at the standard topical dose used in humans significantly reduced eye inflammation and maintained retinal function in our rabbit model as compared with LVFX. The standard errors for intraocular inflammation scores were quite large in many of the groups. However, this is unsurprising, as the extent of intraocular inflammation, including the abundance of fibrin and hypopyon, is highly variable in this model. This was to be expected based on the results of our earlier study. 8 In other studies using staphylococci, 0.5% MFLX provided effective prophylaxis to prevent endophthalmitis.21,22 Interestingly, in those studies, MFLX was more effective than LVFX in preventing experimental fluoroquinolone-resistant methicillin-resistant Staphylococcus aureus in an endophthalmitis model, consistent with our findings.
The timing of antibiotic administration is important to reduce the risk of vision loss caused by postoperative E. faecalis endophthalmitis. E. faecalis has a high bacterial activity that may result in poor visual outcomes after cataract surgery. Therefore, immediate postoperative antibiotic administration is essential to improve bacterial killing and prevent infection by blocking the rapid penetration of E. faecalis to the anterior chamber. Antibiotic eye drops are generally administered immediately after cataract surgery, and the eye is patched. Additional antibiotic eye drops are then administered 1 day after surgery. However, one study found a significantly higher risk of endophthalmitis when antibiotics were administered 1 day after surgery than when administered on the day of surgery. 6 Their findings suggest that antibiotic eye drops should be administered starting on the day of surgery, consistent with our findings.
There are several possible reasons to explain why MFLX showed superior effects to LVFX in this study. First, MFLX was reported to achieve higher concentrations in ocular tissue.23,24 For example, Fukuda and Sasaki reported that the maximum concentrations of MFLX in all rabbit eye tissues tested (cornea, aqueous humor, iris/ciliary body, and vitreous body) were highest of 5 ophthalmic fluoroquinolone solutions administered. 23 Moreover, topical preoperative administration of 0.5% MFLX achieved greater corneal and aqueous penetration in humans than did 0.3% gatifloxacin. 24 Second, the available formulations of MFLX can exceed the MIC of many pathogens in ocular fluids and tissues in animal models25,26 and in humans, 27 which is particularly important for effective postoperative endophthalmitis prophylaxis. In this study, we determined the MICs of MFLX and LVFX against 13 E. faecalis isolates using the methods recommended by the CLSI. 9 In vitro susceptibility testing revealed that MFLX (50% MIC: 0.25 μg/mL) was more potent than LVFX (2 μg/mL). MFLX was reported to achieve anterior chamber concentrations of 2 μg/mL, and by achieving concentrations in excess of the 50% MIC, MFLX could prevent the development of less-susceptible pathogens.28,29 Both the low MIC and good ocular penetration of MFLX are characteristics essential for effective prophylactic therapy.21,22 However, several strains, including some that cause endophthalmitis, showed resistance to MFLX and LVFX. Thus, we need other antibiotics to target fluoroquinolone-resistant E. faecalis. Third, MFLX, a fourth-generation 8-methoxyfluoroquinolone broad-spectrum antibiotic, shows very broad antibacterial activity.28,30,31 MFLX also shows superior antibiotic activity and sensitivity for gram-positive and gram-negative ocular pathogens compared with earlier-generation fluoroquinolones.30,32,33
The results of our study should be interpreted with care, considering the limitations. First, this study was conducted in a rabbit model with experimentally induced E. faecalis endophthalmitis. Although this closely resembles the clinical situation, it is not identical to it. For example, endophthalmitis can be caused by other bacteria, although E. faecalis is potentially the most severe causative bacteria in terms of visual outcomes. Second, the formulations of MFLX and LVFX used in vivo were the same as those used in clinical practice. Therefore, the effective intraocular concentration in this animal model may exceed that achieved in humans, considering the differences in the eye size.
In conclusion, the results of this study indicate that MFLX delays retinal damage compared with LVFX when used to treat endophthalmitis induced by E. faecalis after cataract surgery. Prospective clinical studies are needed to confirm the potency, efficacy, and safety of early postoperative MFLX prophylaxis for the prevention and treatment of bacterial endophthalmitis.
Footnotes
Acknowledgments
This study was supported in part by research grants from the Japanese Ministry of Education, Culture, Sports, Science and Technology, Tokyo, Japan.
Author Disclosure Statement
The authors have no commercial or financial interests associated with this article.