
Abstract
Abstract
Purpose:
To evaluate the toxicokinetics and tolerability (local ocular and general toxicity) of the anti-inflammatory agent, dexamethasone phosphate (a prodrug of dexamethasone) delivered to the eye in rabbits by transscleral iontophoresis.
Methods:
Female rabbits (n=6/group) received dexamethasone phosphate (40 mg/mL ophthalmic solution, EGP-437) transsclerally to the right eye (OD) using the Eyegate® II ocular iontophoresis delivery system once biweekly for 24 consecutive weeks at current doses of 10, 14, and 20 mA-min and current levels up to, and including −4 mA for 3.5–5 min. The study included 2 control groups (n=6/group): (1) a noniontophoresis control [an ocular applicator-loaded citrate buffer (placebo) without current] and (2) an iontophoresis control (a citrate buffer plus cathode iontophoresis at 20 mA-min, −4 mA for 5 min). Recoverability was evaluated 4 weeks following the last dose in 2 animals per group. The left eye (OS) was untreated and served as an internal control for each animal. Ocular and general safety of dexamethasone phosphate and dexamethasone were assessed. Other evaluations included toxicokinetics, ophthalmic examinations, intraocular pressure (IOP) measurements, electroretinographs, clinical observations, body weight, hematology and serum chemistry, gross necropsy, organ weight, and microscopic histopathology.
Results:
The biweekly transscleral iontophoresis with either the citrate buffer or dexamethasone phosphate at cathodic doses up to, and including 20 mA-min and currents up to, and including −4 mA for 24 weeks was well-tolerated. Transient signs of conjunctival hyperemia and chemosis, mild corneal opacity, and fluorescein staining of the cornea were noted and attributed to expected ocular reactions to the temporary placement of the ocular applicator and application of iontophoresis. There were no dexamethasone phosphate-, dexamethasone-, or iontophoresis-related effects on IOP, electroretinography, or histopathology.
Reductions in body weight gain, anemia, decreased leukocyte and lymphocyte counts, compromised liver function, enlarged liver, and reduced spleen weight were consistent with systemic corticosteroid-mediated pharmacology, repeated use of anesthesia, stress, and sedentariness, and unlikely to be related to iontophoresis application.
Conclusions:
The results of this investigation suggest that repeated transscleral iontophoresis with dexamethasone phosphate may be safe for use as a treatment for inflammatory ocular disorders that require prolonged and/or repeated corticosteroid therapy.
Introduction
Researchers have studied many strategies to overcome the aforementioned shortcomings of existing drug dosing options. One example, ocular iontophoresis employs the principle that when a current is applied in a coulomb-controlled manner, like charges repel and unlike charges attract. 7 Investigators have explored the feasibility of utilizing ocular iontophoresis to deliver corticosteroids to both the anterior and posterior ocular regions. Lam et al. 8 measured significant vitreal dexamethasone concentrations following the transscleral iontophoresis delivery of dexamethasone phosphate, although using high current density and a long treatment time (25 min). Eljarrat-Binstock 9 used a dexamethasone-loaded hydrogel and a portable iontophoretic device to achieve therapeutic concentrations of dexamethasone using a lower current density (5.1 mA/cm2) and a shorter treatment time (4 min).
The EyeGate® II Delivery System (EGDS, Eyegate Pharmaceuticals, Inc., Waltham, MA) is a novel ocular iontophoresis system designed to noninvasively deliver substantial levels of drug into the anterior and posterior segments of the eye, while minimizing systemic distribution. 10 The EGDS employs an annular ocular applicator that houses an inert chemical electrode, which produces ions (hydroxide or hydronium via electrolysis of water) that primarily drive ionized drug molecules into and through the conjunctiva and sclera via electrochemical repulsions. The current applied to the ocular applicator is the same charge as the drug that facilitates molecular movements (via electrochemical repulsion). A return electrode that is connected to the opposite electrical pole is attached to the patient or study animal, which completes the circuit.
Using the EGDS, it was recently demonstrated 10 that a single transscleral iontophoretic dose of a dexamethasone phosphate acidic solution (40 mg/mL at 10, 20, or 30 mA-min) to the rabbit eye effectively delivered dexamethasone phosphate and dexamethasone (dexamethasone phosphate is a prodrug that is converted to dexamethasone) to both the anterior and posterior ocular regions (retinal, choroid, aqueous humor, and vitreous humor) at 15 min postdose. The measured concentrations were directly proportional to the current applied and the dexamethasone phosphate concentration utilized.
The EGDS has been studied in multiple human clinical trials that have examined the safety and efficacy of transscleral iontophoresis with dexamethasone phosphate (EGP 437; a 40 mg/mL solution designed for specific use with the EGDS). In patients with moderate to severe dry eye, 2 EGP-437 treatments at 7.5 mA-min significantly improved signs and symptoms of their condition. 11 In patients with noninfectious anterior segment uveitis, a single EGP-437 application at 1.6, 4.8, 10.0, or 14.0 mA-min significantly reduced anterior chamber cell counts without causing any noteworthy systemic exposure or irreversible adverse events. 12
There is a paucity of published data examining the safety of repeated transscleral iontophoresis exposure (without drug) and repeated transscleral iontophoresis of dexamethasone phosphate (ultimately dexamethasone). The primary aim of this investigation was to examine the safety of repeated ocular iontophoresis with the citrate buffer (placebo) and the toxicokinetics and safety of dexamethasone phosphate (ultimately dexamethasone) delivered transsclerally biweekly for 24 weeks in female New Zealand albino rabbits using the EGDS: (1) each animal was treated in the right eye (OD) and the fellow eye (the left eye, OS) was untreated and served as an internal control for each animal and (2) one-third of the animals had a 4-week recovery period (Recovery animals) to assess any persistent, delayed occurrence, and/or recovery from study-related effects. The parameters monitored included toxicokinetics, ophthalmic examinations, IOP, electroretinography (ERG), clinical observations, body weight, clinical pathology (hematology and serum chemistry), organ weights, and necropsy/histopathology.
Methods
Materials
About 100 mM of the sodium citrate buffer solution at pH 5.7 was prepared by combining appropriate amounts of 100 mM sodium citrate, dihydrate (Avantor Performance Materials, Center Valley, PA) with 100 mM citric acid, and monohydrate (Avantor Performance Materials). The solution was sterile filtered using a 0.22-micron filter (Nalgene; Thermo Fisher Scientific, West Chester, PA), divided into aliquots, and stored at ∼4°C.
Dexamethasone phosphate acid (Dalton Pharma Services, Toronto, ON, Canada.) was suspended in sterile water for injection (WFI). The pH of the solution was adjusted to 5.7–5.8 with 1.0 M sodium hydroxide in sterile WFI. The final volume was adjusted to 100 mL with WFI for a final concentration of 40 mg/mL and sterile filtered using a 0.2 micron filter (Acrodisc; Pall Corporation, Port Washington, NY). Aliquots were stored at ∼4°C and protected from light. All dosing solutions were stable throughout the study.
Animals
All animals utilized in this study were treated according to the guidelines established by the Association for Research in Vision Ophthalmology (ARVO) for design and conduct of animal experimentation. The study protocol was also reviewed and approved by the Eyegate Institutional Animal Care and Use Committee.
Animals were housed individually in standard cages under controlled conditions (7–10 air exchanges per hour; 12-h light/12-h dark cycle; temperature between 67°F–70°F; relative humidity; 30%–63%) and treated according to the Institute of Laboratory Animals Guide for the Care and Use of Laboratory Animals (2011). Animals had access to food (Hi-Fiber Rabbit Pellets, Lab Diet) and water available ad libitum throughout the study.
Animals were anesthetized before iontophoresis dosing, ERG recording, blood collection, and euthanized by intramuscular injection of 2.5–5.0 mg/kg of xylazine (IVX Animal Health, Inc., St. Joseph, MO) and 25.0–35.0 mg/kg of ketamine (Fort Dodge Animal Health, Overland Park, KS). In addition, animals were sedated with acepromazine (Fermenta Animal Health Co., Kansas City, MO) for toxicokinetic blood collections.
Experimental design
Thirty female adult albino New Zealand rabbits (Millbrook Breeding Laboratories, Amherst, MA; weighing 3.4 to 4.4 kg) were assigned to 1 of 5 groups (Groups A–E; 6 animals/group) that received the following transscleral iontophoresis treatments to the right eye only biweekly for 24 consecutive weeks (12 doses in total): (1) Group A (Noniontophoresis Control; iontophoresis applicator+citrate buffer placed on the eye for ∼5 min, no current applied); (2) Group B [(Iontophoresis Control; citrate buffer administered for 20 mA-min at −4 mA (∼5 min)]; (3) Group C [dexamethasone phosphate Low Iontophoresis; dose administered for 10 mA-min at −3 mA (∼3.5 min)]; (4) Group D [dexamethasone phosphate Mid Iontophoresis; dose administered for 14 mA-min at −4 mA (∼3.5 min)]; and (5) Group E [dexamethasone phosphate High Iontophoresis; dose administered for 20 mA-min at −4 mA (∼5 min)].
On dosing days, animals underwent both ocular and general evaluations, including body weight measurements, clinical observations, clinical pathology (hematology and serum chemistry), ocular examinations, IOP measurements, ERG, as well as toxicokinetic assessment. Four animals from each treatment group were euthanized 1–2 days after the last dose of dexamethasone phosphate (Main Study animals). The remaining 2 animals from each treatment group were euthanized 4 weeks following the last dose (Recovery animals). Gross necropsy, organ weight, and histological evaluation of eyes, brains, and any abnormal tissue or organ were performed on the Main Study and Recovery animals.
Transscleral iontophoresis
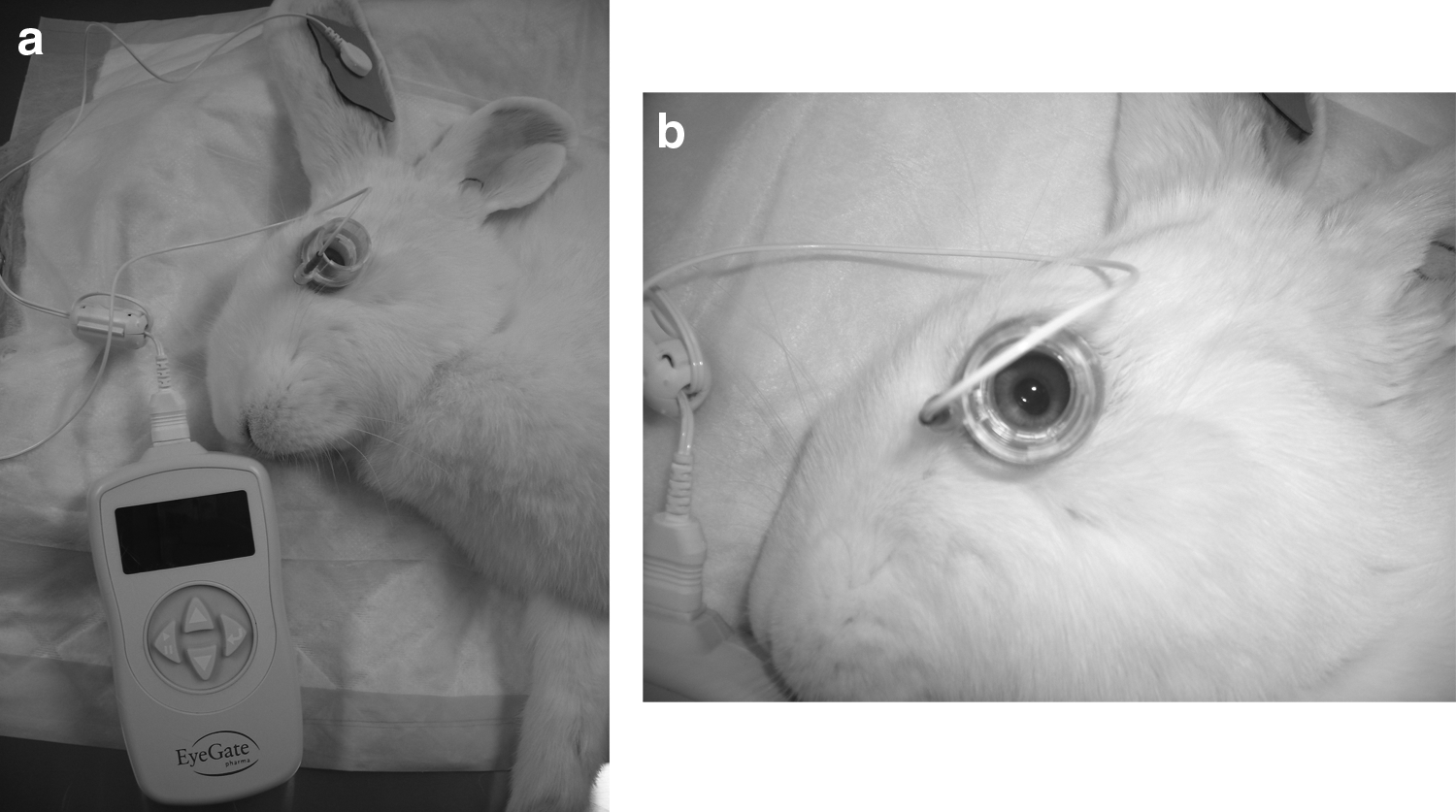
The transscleral iontophoresis applicator system consisted of a novel, sterile single-use disposable Eyegate II Iontophoresis Device (Lot #092314), disposable single-use Eyegate Return Electrodes (Ref #SA-0006-01), and a Yokogawa model GS610/765502 generator. Briefly, the biweekly transscleral iontophoresis procedure consisted of the following: subsequent to removing the hair from each ear, a return electrode was placed on each ear and connected to the generator (as shown in Fig. 1). The Eyegate II applicator was loaded with ∼0.5 mL of either the citrate buffer or dexamethasone phosphate. Anesthetized animals were placed in a left lateral recumbent position and 1 to 2 drops of Proparacaine Hydrochloride Ophthalmic Solution USP 0.5% (Bausch and Lomb, Rochester, NY) were applied topically to the right eye. The drug or citrate buffer loaded Eyegate II applicator was then connected to the generator and carefully placed on the right eye. At the end of each treatment, both the ocular applicator and return electrodes were removed from the animal.
Pharmacokinetics
Blood was collected for analysis 24 h before dosing, and at 1, 2, 5, and 24 h postdosing for doses 1 (week 1), 6 (week 11), and 12 (week 23). Plasma was obtained and stored at approximately −80°C until analyzed for dexamethasone phosphate and dexamethasone concentrations by LC-MS/MS using an Agilent G6410A Mass Spectrometer (Santa Clara, CA) in a positive ion mode. Systemic exposure was analyzed at multiple time points to determine the peak plasma concentration, time to peak concentration, the half-life, and the area under the plasma concentration curve (Cmax, Tmax, t1/2, and AUC, respectively), with WinNonlin version 4.1 (Pharsight Corp., Sunnyvale, CA) using an appropriate noncompartmental model.
Nonclinical safety
Ophthalmic examinations were performed on both eyes of all anesthetized animals immediately before (direct ophthalmoscopy) and after (direct ophthalmoscopy and fluorescein staining) treatment on iontophoresis dosing days. Direct ophthalmoscopy and fluorescein staining were also performed on all nonanesthetized animals once a week on nondosing weeks. On the day of euthanasia, Main Study and Recovery animals also received a final direct ophthalmoscopy examination. Eyes were examined under white light using a hand-held slit lamp (Nikon FS-2, Tokyo, Japan). One to 2 drops of a fluorescein solution prepared from fluorescein strips (Akorn, Lake Forest, IL) were then placed on the eye and the examination was repeated under cobalt blue-filtered light.
IOP was measured in both eyes of all animals twice a week during all dosing and nondosing weeks until the animals were euthanized in both Main Study and Recovery groups. One to 2 drops of Proparacaine Hydrochloride Ophthalmic Solution 0.5% (Bausch & Lomb, Rochester, NY) were applied to each eye and IOP was measured using a calibrated pneumatonometer (Model 30 classic, Reichert; Depew, NY).
ERG was performed on both eyes of all animals after 3 and 6 months of dosing (Main Study animals). The Recovery animals received final ERGs after the 4 nondosing weeks. All ERGs were completed using a handheld multispecies electroretinograph unit (RetVet Corporation, Inc., Columbia, MO) according to guidelines outlined by the International Society for Clinical Electrophysiology of Vision (ISCEV). Rabbits were dark adapted for at least 1 h before testing. One to 2 drops of a mydriatic agent (Atropine Sulfate Ophthalmic Solution USP 1%; Bausch and Lomb, Rochester, NY) were applied to the eye 10–15 min before performing ERG measurements in anesthetized animals.
Ground and reference electrodes in the electroretinograph unit were placed subcutaneously in the ear and on the occipital area halfway between the base of the ear and eye, respectively. The corneal contact electrode was filled with 1% carboxymethylcellulose (CelluVisc; Allergan, Irvine, CA) and centered on the cornea. If baseline resistance was >2,000 Ω, all electrodes were checked and repositioned or replaced until the appropriate baseline resistance was obtained. The following testing steps were carried out for each eye: (1) Rod ERG, (2) Standard Combined ERG (rod and cone), (3) High-intensity Combined ERG (rod and cone), (4) Single-flash cone ERG, (5) High-intensity cone ERG, (6) Low-intensity Flicker ERG, and (7) High-intensity Flicker ERG. ERG data were analyzed using ERGVIEW version 2.5 software (RetVet Corporation, Inc., Columbia, MO).
Clinical observations were performed daily during the study and included assessment of general appearance, stool characteristics, appetite, and symptoms of overt toxicity. Attention was paid to ocular inflammation, discharge, and blepharospasm as well as corticosteroid-related systemic toxicity (including, but not limited to, lethargy or aggressiveness, decreased appetite, coat appearance, and skin lesions).
Body weights were measured twice a week using scales with a capacity of 2 g–34 Kg (Sartorius Model EB6DCE and CB34EDX-N, Goettingen, Germany) during all dosing (Main Study) and nondosing (Recovery) weeks.
Clinical pathology (hematology and serum chemistry) was assessed in all animals 8–12 days before initial dosing (predose), during week 11 (postdose 6) and 23 (postdose 12) of the Main Study, and at the end of recovery (week 28). Blood was collected from anesthetized animals via the ear or jugular vein into tubes containing EDTA (hematology assessment; 1 mL; Becton Dickinson Microtainers, Franklin Lakes, NJ) or without any anticoagulant (serum chemistry assessment; 3 mL; Eppendorf Safe Lock, Hamburg, Germany). Serum was obtained by centrifugation at ∼10,000 rpm for ∼5 min. Refrigerated whole blood and serum samples were shipped to IDEXX Laboratories, Inc. (Westbrook, ME) for analysis within 24–48 h of blood collection. Hematology and serum chemistry were analyzed.
Complete gross necropsy was conducted on all animals and included the carcass and musculoskeletal system, all external surfaces and orifices, cranial cavity and external surface of the brain, and all thoracic, abdominal, and pelvic cavities with their associated organs and tissues. The heart, liver, lung, kidneys, spleen, thymus, and brain from all animals were weighted. Both ocular globes (including adnexa and optic nerves) from all animals were enucleated, rinsed in phosphate-buffered saline (Gibco, Grand Island, NY), and fixed in Davidson's fixative. Brains were stored in 10% neutral-buffered formalin (Fisher Scientific, Pittsburgh, PA). Organs and/or tissues with suspected abnormalities were collected and stored in 10% neutral-buffered formalin.
A histopathology examination of fixed ocular globes, brains, and abnormal organs/tissues was performed by Charter Preclinical Services (Hudson, MA). Samples were paraffin embedded, sectioned, stained with hematoxylin and eosin, and examined for any signs of morphological changes or tissue damage by a veterinary pathologist masked to the samples identity.
Results
Pharmacokinetics
Plasma concentrations of dexamethasone phosphate (the parent or prodrug) and dexamethasone (the drug) were monitored after ocular iontophoresis administration of dexamethasone phosphate on week 1 (dose 1), week 11 (dose 6), and week 23 (dose 12) from samples collected within 24 h before dosing, and at 1, 2, 5, and 24 h postdosing. The mean plasma concentrations of dexamethasone phosphate and dexamethasone per dosing group (Groups C–E) are shown in Fig. 2, while mean Tmax, Cmax, and AUC0–24h values are summarized in Tables 1–3, respectively. In general, the exposure profiles were similar for all iontophoresis groups and doses.
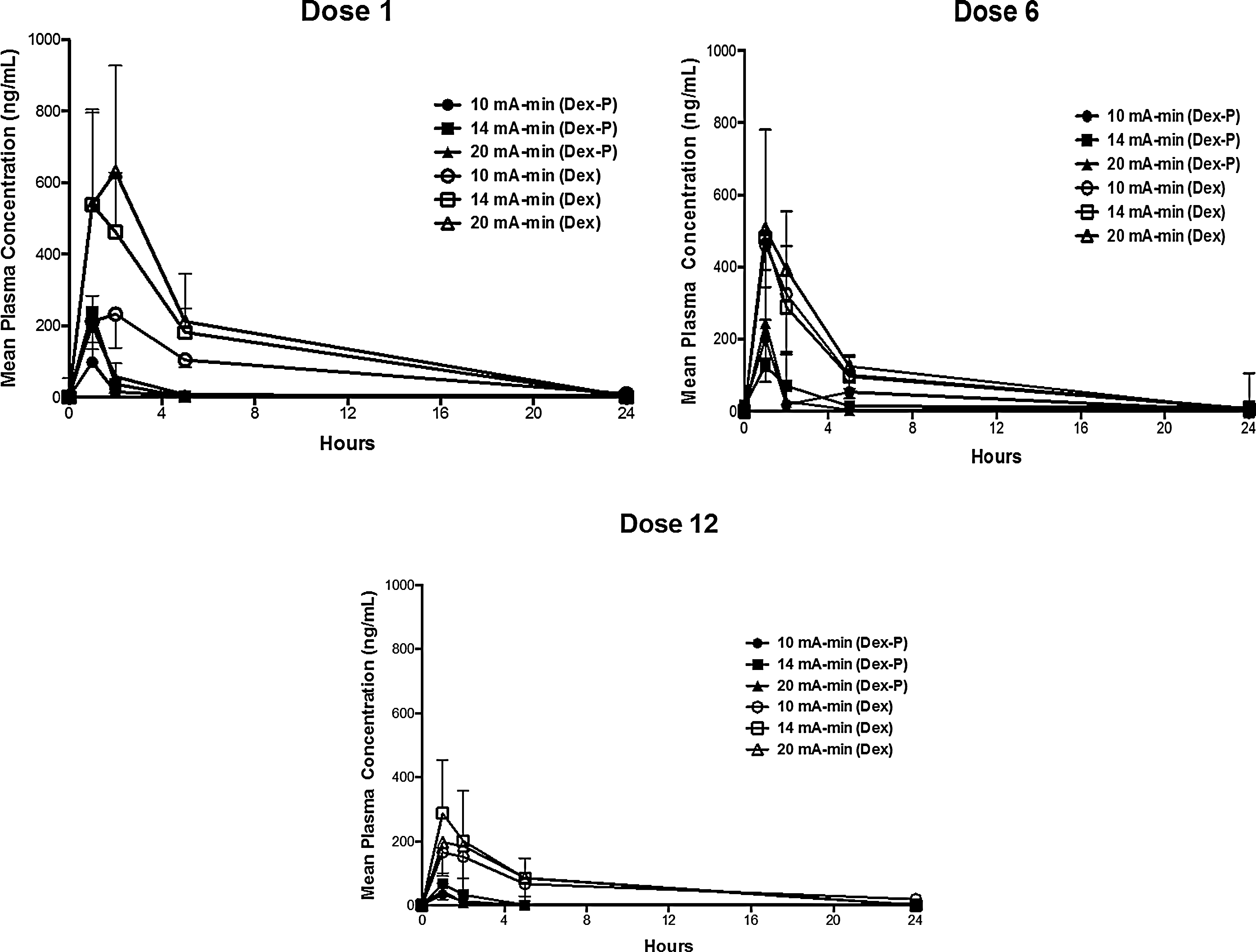
Mean plasma concentrations of dexamethasone phosphate (prodrug) and dexamethasone (drug) following ocular iontophoresis delivery of dexamethasone at 10, 14, and 20 mA-min for dose 1 (week 1), dose 6 (week 11), and dose 12 (week 23) (n=6/dosing group).
n=6/group; values in parentheses are standard deviations.
Plasma Cmax and AUC0–24h values for dexamethasone were larger than the corresponding values for dexamethasone phosphate after ocular iontophoresis administration of dexamethasone phosphate. Plasma Cmax and AUC0–24h values were lower following dose 12 when compared to dose 1 and dose 6. Tmax values for dexamethasone phosphate occurred earlier than or at the same time as those for dexamethasone. There was no remarkable accumulation of either dexamethasone phosphate or dexamethasone following multiple dosing of parent dexamethasone phosphate. Exposure to both dexamethasone phosphate and dexamethasone increased with the iontophoresis dose for the first iontophoresis treatment only (dose 1 during week 1).
Ocular assessments
Ocular findings were noted immediately following dosing in all Groups A–E due to placement of the iontophoresis applicator on the eye; they included transient hyperemia, slight, mild, or moderate conjunctival congestion, swelling, and chemosis.
Treatment in all iontophoresis Groups B–E was associated with transient inferior corneal opacity as well as mild to moderate corneal opacities periodically observed following dosing ranging from spots on the inferior cornea to a large semicircular band affecting both the inferior and central cornea. Opacities were noted more frequently and affected a larger area in dexamethasone phosphate-treated iontophoresis groups (Groups C–E) compared to the placebo iontophoresis control group (Group B). Within the dexamethasone phosphate iontophoresis groups, a positive correlation between the number of corneal opacities and iontophoresis dose was observed. These corneal opacities were transient and not present during either predosing, nondosing weeks, or in Recovery animals. It should be noted that the iontophoresis applicator (designed to fit the human eye) sits over a larger surface area of the rabbit cornea than the human cornea.
Sedating the animals, placing the iontophoresis applicator, and the iontophoresis treatments of dexamethasone phosphate all resulted in transient corneal fluorescein staining as an indicator of corneal damage or lesions. Mild to moderate fluorescein staining of the superior, central, and inferior corneal regions was noted for the majority of treated and fellow (untreated) eyes in anesthetized animals following dosing. Enhanced staining was observed in fellow compared to treated eyes and was more frequently noted toward the completion of the dosing period (Main Study). For treated and fellow eyes, there was no correlation between fluorescein staining in superior or central corneal regions and superior, central, or inferior corneal regions and treatment groups, respectively; staining was likely related to an anesthesia-induced lack of blinking. In contrast, fluorescein staining of the inferior corneal region of treated eyes appeared to be related to the iontophoresis treatment since it was present in the area where the applicator was positioned during treatment, had a shape reminiscent of the applicator, and was more frequently noted in the dexamethasone phosphate-treated animals compared to the controls.
Transscleral iontophoretic dexamethasone phosphate treatment had no effect on IOP in treated (OD) and fellow (OS) eyes. As illustrated in Fig. 3, mean IOP in the treated right eye fluctuated within normal limits (10 to 25 mmHg) for all treatment groups; occasionally, IOP values higher than 25 mmHg were observed.
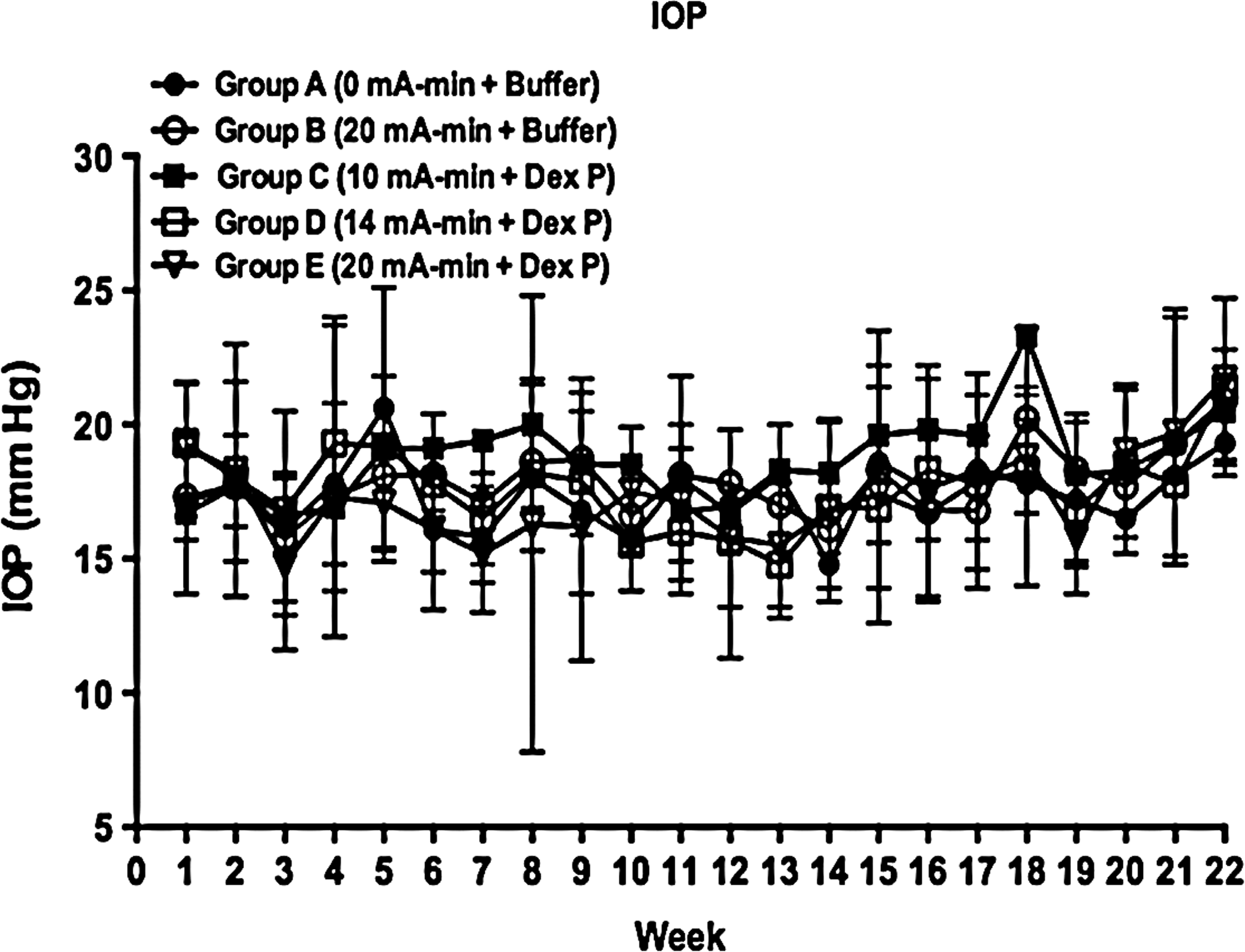
Mean intraocular pressure (IOP) measured weekly for 22 weeks following ocular iontophoresis delivery of dexamethasone phosphate at doses of 10, 14, and 20 mA-min. Group A (0 mA-min+buffer) and Group B (20 mA-min+buffer) provided as controls. (n=6/dosing group).
Applicator placement, iontophoresis treatment, and dexamethasone phosphate administration had no overall effect on the retinal rod and cone function in either treated or fellow eyes. Sporadic differences between baseline and postdose 6 or postdose 12 measurements were observed for some retinographic parameters in all iontophoresis groups and were considered incidental (observed in treated and fellow eyes and without a clear pattern). Similar to the above, sporadic differences between placebo noniontophoresis control, placebo iontophoresis control, and dexamethasone phosphate iontophoresis groups were also observed for some retinographic parameters and considered random effects (they occurred in both treated and fellow eyes and at pre- and postdose time points without a clear pattern).
Clinical observations
There were no major clinical observations related to transscleral iontophoresis treatment with dexamethasone phosphate. The most frequent observations were transient scabs on rear limbs and urine retention, which were likely related to technical procedures (e.g., scabs on rear limbs due to frequency of animals receiving IM injections for extended periods), sedentariness of the animals, and potentially systemic dexamethasone pharmacology.
Body weight
Dexamethasone phosphate delivered by transscleral iontophoresis affected body weight over the course of the study. Average body weight gain was similar between placebo noniontophoresis (Group A) and placebo iontophoresis (Group B) controls. Administration of dexamethasone phosphate (Groups C–E) resulted in lower average body weight gain when compared to corresponding controls. Within the dexamethasone phosphate-treated groups, there appeared to be a negative correlation between iontophoresis dose and mean body weight gain (Fig. 4), suggestive of a relationship to systemic corticosteroid pharmacology or repeated induction of anesthesia.
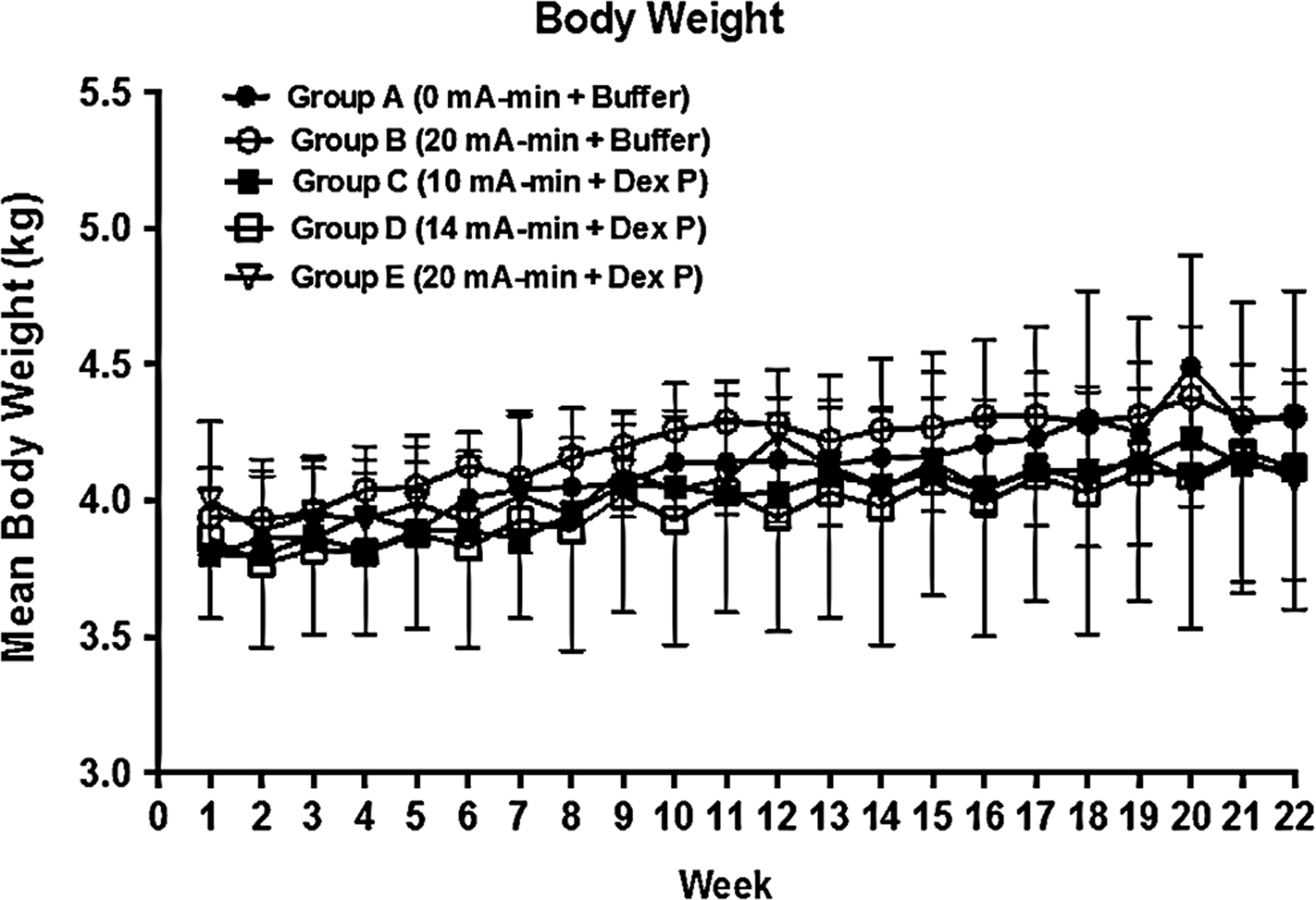
Mean body weight measured weekly for 22 weeks following ocular iontophoresis delivery of dexamethasone phosphate at doses of 10, 14, and 20 mA-min. Group A (0 mA-min+buffer) and Group B (20 mA-min+buffer) provided as controls. (n=6/dosing group).
Clinical pathology
The changes observed in the clinical chemistry parameters (hematology and serum chemistry) in the Main study phase were consistent with systemic corticosteroid pharmacology and/or repeated administration of anesthesia, but not iontophoresis treatment. Animals from all groups (Groups A–E) showed evidence of anemia and compromised liver function as the study progressed. Mean red blood cell counts (RBC), hemoglobin concentration (HGB), and hematocrit (HCT) decreased in dexamethasone phosphate iontophoresis groups (Groups C–E) when compared to controls (Groups A–B) (Table 4). Mean corpuscular hemoglobin concentration (MCHC) decreased in all groups (Groups A–E) over time. RBC, HGB, HCT, and MCHC returned toward predose levels in all groups during the recovery period with the exception of dexamethasone phosphate high-dose iontophoresis Group E, where RBC, HGB, and HCT remained reduced (Table 4).
n=6/group; values in parentheses are standard deviations.
Reductions in mean white blood cells (WBC) and lymphocytes were observed in all treatment groups as the study progressed (Table 5). Decreases in WBC were more substantial for dexamethasone phosphate-treated iontophoresis groups (Groups C–E) when compared to controls (Groups A–B) (Table 5). During the recovery period, the remaining WBC values in Groups A–D were maintained or increased toward predose levels, but the WBC values continued decreasing in Group E. Decreases in% lymphocytes were more pronounced in dexamethasone phosphate-treated iontophoresis groups (Groups C–E) when compared to controls (Groups A–B) (Table 5). Lymphocyte reductions (both absolute cell counts and percentages) were generally reversible in Groups A and B, but not in Groups C–E.
n=6/group; values in parentheses are standard deviations.
Increases in total protein and globulin concentrations were noted only in the dexamethasone phosphate-treated iontophoresis groups (Groups C–E). Alkaline phosphate concentrations decreased in all groups (Groups A–E) (Table 6). Increases in glucose concentrations and creatine phosphokinase as well as decreases in cholesterol were observed in all groups (Groups A–E) as the study progressed (data not shown); these changes were likely related to changes in food intake and/or sedentariness (changes in glucose and cholesterol) as well as repeated intramuscular injections of anesthetics (creatine phosphokinase).
n=6/group; values in parentheses are standard deviations.
Organ weights and histopathology
Reversible increases in liver weight were observed in dexamethasone phosphate-treated iontophoresis groups (Groups C–E) when compared to placebo controls (Groups A–B). Decreased spleen weights were observed in dexamethasone phosphate-treated iontophoresis groups (Groups C–E) when compared to placebo controls (Groups A–B). Spleen weights in Recovery animals were similar in all treatment groups except for dexamethasone phosphate high iontophoresis-treated animals (Group E), which remained low. Reduced spleen weights and enlarged livers are consistent with systemic corticosteroid pharmacology, and unlikely related to iontophoresis application. Histological abnormalities or microscopic lesions were not detected in any of the organs (brains or treated eyes) examined.
Discussion
Corticosteroids, such as dexamethasone, are mainstay treatments for various ocular inflammatory conditions. Their use typically requires achieving significant drug levels in the anterior and/or posterior segments of the eye.1,2 Traditional methods for administering drugs, including topical, oral, intravenous, and periocular delivery, can be inadequate due to low ocular bioavailability and/or the blood–retinal barrier. 3 Although effective, the invasive nature of intravitreal injections makes this route of dosing somewhat undesirable. The risks or side effects associated with local or periocular injection of corticosteroids include bulbar perforation, choroidal injection, central retinal artery occlusion, muscle imbalance, and elevations in IOP. 13 Systemic absorption of periocular corticosteroids leads to a reduction in total white cells and circulating lymphocytes. 5 General corticosteroid-mediated side effects or toxicity have been characterized in various species and include metabolic disturbances (hyperglycemia, insulin resistance, and diabetes), osteoporosis, cataract formation, and retinopathy. 5
The development of transscleral iontophoresis as a noninvasive method to increase both anterior and posterior dexamethasone phosphate ocular drug permeability has been successfully applied preclinically in rabbits9,10 and clinically to treat dry eye and noninfectious anterior segment uveitis in humans.11,12 In these studies, subjects received 1 single or 2 repeat iontophoretic treatment doses of a specially formulated 40 mg/mL dexamethasone phosphate solution to assess pharmacokinetics, efficacy, and/or safety. The results of the present investigation in which rabbits received ocular iontophoresis with the citrate buffer or 40 mg/mL dexamethasone phosphate biweekly via for 24 weeks at doses up to, and including 20 mA-min to assess tolerability and safety as well as systemic plasma toxicokinetics extend the finding of previous studies. The doses utilized in this study are noteworthy. The rabbits received the same concentration of drug product (40 mg/mL dexamethasone phosphate) as humans at iontophoretic dose levels at or above those used in humans. Since the rabbit eye is significantly smaller than the human eye and the rabbit body weights (3.5 kg) are about 5% that of the average human's weight (70 kg), the local and systemic exposures achieved in the rabbits are substantially higher than those realized in humans. 12 In addition, the systemic exposures achieved in the rabbit studies are exaggerated because rabbits have about 50% the blood volume per unit mass of that found in humans. Additionally, treating humans with the EGDS does not require intramuscular anesthesia (which may lead to or amplify untoward effects, as observed in the present investigation).
Ocular toxicity associated with the delivery of corticosteroids such as dexamethasone by various routes of administration has been extensively studied. Kwak and D'Amico 14 demonstrated that intravitreal injection of dexamethasone sodium phosphate at doses from 0.4 to 4.0 mg in rabbit eyes produced dose-dependent disruption of Muller cells indicative of retinal toxicity. Shimada and Matsui 15 also showed evidence of histopathological retinal degeneration and vitreous inflammation following intravitreal injection of up to 80 mg of dexamethasone in rabbit eyes. Using biomarkers of retinal degeneration, retinal malondialdehyde (MDA) and glutathione (GSH), Citirik et al. 16 demonstrated that intravitreal injection of high-dose dexamethasone (0.2 mg) in rats increased MDA and GSH in the retina. There were no histopathological changes noted in the present investigation following iontophoretic delivery of dexamethasone phosphate to the eyes of rabbits.
As noted above, chronic use of corticosteroids such as dexamethasone by various routes of delivery may also lead to ocular side effects such as increases in IOP and cataracts. Rabbits treated with 0.1% dexamethasone phosphate topically (1 drop 3 times a day for 5 weeks) exhibited increases in IOP as early as a few days after treatment, peaked as early as 2 weeks after commencing daily dosing (week 0 and week 2 values of 9.8+0.6 and 27.8+10.0 mm Hg, respectively), and remained elevated until the end of treatment. 17 C57BL/6.129 F2 hybrid mice treated with dexamethasone dosed systemically at 0.09 mg/day using micro-osmotic pumps demonstrated clear evidence of ocular hypertension (increases in ocular pressure of ∼23%–28%) compared to corresponding vehicle controls after 21 days of treatment. 18 At the doses tested in the present study, there were no demonstrable effects on IOP or evidence of cataract formation.
In the present investigation, only minor, generally reversible alterations in clinical pathology, including hematology (reductions in red blood cells and leukocytes and related parameters) and serum chemistry (decreases in alkaline phosphatase and increases in total protein and globulin) attributed to expected systemic corticosteroid pharmacology and not overt toxicities were noted. Similarly, clinical observations were limited to minimal reductions in weight gain.
Using the EGDS loaded with a 40 mg/mL aqueous formulation of dexamethasone phosphate, Gungor et al. 10 measured the ocular exposure of the prodrug, dexamethasone phosphate, and its active metabolite, dexamethasone, in rabbits that received a single iontophoretic treatment at doses of 2, 4, or 6 mA for 5 min (10, 20, and 30 mA-min, respectively). Concentrations of dexamethasone phosphate at 15 min postapplication were dose dependently greater than dexamethasone in total tissue as well as aqueous and vitreous humor and calculated to be anti-inflammatory based on data in the literature.
Plasma, but not ocular concentrations of dexamethasone phosphate and dexamethasone were measured in the present investigation. Plasma concentrations of dexamethasone were higher than dexamethasone phosphate following iontophoretic dosing of dexamethasone phosphate on week 1, 11, and 23 suggesting rapid conversion somewhere between the ocular and the vascular compartment (most likely in the blood). This phenomenon was not evident in a study in rabbits that examined the pharmacokinetics of dexamethasone phosphate (25 and 250 μg/kg) and the metabolite, dexamethasone, using intravenous, subconjunctival, and intravitreal routes of administration. 2
The toxicokinetics of dexamethasone phosphate and dexamethasone were less than dose proportional with repeated dosing over time (weeks 11 and 23) in the current investigation. That is, exposure to dexamethasone phosphate and dexamethasone increased with increasing iontophoresis dose only after the initial iontophoresis dose (week 1). The cause of this reduction is unknown.
Conclusions
Biweekly ocular administration of a specially formulated dexamethasone phosphate solution using a novel iontophoresis delivery device, EGDS, was well-tolerated. Transient ocular effects were noted and attributed to expected ocular reactions to the temporary placement of the applicator and use of iontophoresis. There were no dexamethasone phosphate- or iontophoresis-related effects on IOP, ERG, or ocular histopathology. These data support and expand preclinical findings that repeated iontophoretic delivery of dexamethasone phosphate is safe up to, and including the maximum dose tested in the present investigation.
Footnotes
Author Disclosure Statement
M.P. is an employee of Eyegate Pharmaceuticals, Inc. (EGP); B.R.-P, T.S., R.G., and M.B. are former employees of EGP. No competing financial interests exist.