
Abstract
Abstract
Purpose:
To evaluate the vitreous clearance and toxicological profile of commercially available lornoxicam (Xefo), after a single intravitreal injection in rabbits.
Methods:
Twenty-five male albino rabbits (10 rabbits were used for retinal toxicity evaluation, while 15 rabbits were used to evaluate vitreous clearance) were used in this study. Two concentrations of lornoxicam were tested for retinal toxicity: 250 μg/0.1 mL and 1,500 μg/0.1 mL. Each concentration was intravitreally injected randomly in 1 eye of each rabbit (group I received 250 μg/0.1 mL, n=5 and group II received 1,500 μg/0.1 mL, n=5), while in the other eye 0.1 mL of sterile balanced saline solution was injected. Slit-lamp and funduscopic examinations along with intraocular pressure measurements (IOP) were performed prior to injection and at days 1, 15, and 30 after the injection for signs of infection, inflammation, toxicity, and IOP changes. A baseline electroretinogram (ERG) was performed before the experiment and at days 1, 15, and 30 after the intravitreal injection. At the last follow-up day, the animals were sacrificed and the enucleated eyes were prepared for histological evaluation of the retina. Lornoxicam (concentration of intravitreal injection: 250 μg/0.1 mL) clearance from the vitreous was estimated using high-performance liquid chromatography in 30 rabbit eyes.
Results:
There were no statistical differences between the control and experimental eyes, concerning ERG amplitudes and IOP measurements for both groups (I and II), at all examinations. On the contrary, histological examination of the samples revealed extended retinal damage of group II experimental eyes (morphological alterations at the level of the inner nuclear and outer plexiform layers was evident along with disappearance of normal stratification of outer retina with vacuolization and thinning), whereas the morphology of group I experimental eyes did not differ from that of the control eyes. Lornoxicam is eliminated from the vitreous by a first-order kinetic process with a half-life of 1.7 h.
Conclusions:
Intravitreal lornoxicam causes dose-related toxic effect to the retina at a concentration of 1,500 μg. A dose of 250 μg does not seem to cause histological toxic effects at the level of the retina. Lornoxicam could be considered with interest for further research for the development of alternative treatments for ocular inflammatory conditions.
Introduction
Non-steroid anti-inflammatory drugs (NSAIDs) interfere with inflammatory cascades by inhibiting cyclooxygenase enzymes (COX), which catalyze the synthesis of prostaglandins. This group of drugs is used today (mainly topical administration) for the treatment of ophthalmic surface inflammation, and to reduce inflammation after cataract surgery; further, it is used as treatment for postcataract macular edema. Topical and oral administration of NSAIDs, although effective for ocular surface and anterior segment diseases, may not provide sufficient therapeutic levels of the drug to the posterior ocular segment (retina). Consequently, intravitreal delivery of NSAID may offer a more effective approach for their utilization in the treatment of several intraocular inflammatory entities. The lack of the well-known ocular adverse effects of steroids (cataract development and glaucoma),4,5 represent an additional reason for the evaluation of intravitreal NSAIDs as potential anti-inflammatory agents for posterior segment diseases.
Lornoxicam is an NSAID of the oxicam class, with analgesic, anti-inflammatory, and antipyretic properties, which is delivered systemically; further, it is a water-soluble agent appropriate for ophthalmic use. Lornoxicam is used for the treatment of various types of inflammatory diseases of the joints, osteoarthritis, surgery, and other inflammations. In this study we evaluated the vitreous clearance and possible retinal toxicity of intravitreal lornoxicam (XEFO).
Methods
Animals
Twenty-five male albino rabbits, weighing 2.5 to 3.5 kg each, were included in the study. Ten rabbits were used for retinal toxicity evaluation and 15 rabbits were used to evaluate vitreous clearance of lornoxicam. All the experimental procedures followed the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research and the institutional guidelines.
Procedure
Before every procedure or examination, the rabbits were anesthetized by an intramuscular injection of a mixture containing ketamine hydrochloride (50 mg/kg) and xylazine (5 mg/kg) solution. Additional topical anesthesia to the eyes was applied (1 drop of sodium chloride proxymetacain, Alcaine, ALCON Lab, Hellas AEBE).
Lornoxicam
For potential retinal toxicity evaluation 2 concentrations of commercially available lornoxicam (for intravenous/intramuscular use, Xefo® 8 IV/IM Injection, Nycomed Hellas S.A.) were prepared: 250 μg/0.1 mL and 1,500 μg/0.1 mL. The compound is approved for intravenous delivery and thereby is endotoxin- and pyrogen-free. The excipients of the commercially available lornoxicam are mannitol, trometamol (Tris), and disodium edentate (EDTA) as described by the manufacturer. The dilution was performed using water for injection. Extrapolating from the systemic dosage of Lornoxicam, the equivalent intravitreal levels of the drug are ∼0.008 mg (plasma volume ∼4Lt, ophthalmic volume ∼4 mL, and systemic dose of Xefo=8 mg). The 2 dosages we chose to evaluate for retinal toxicity in this study, are more than 30 times greater (250 μg/0.1 mL) and more than 185 times greater (1,500 μg/0.1 mL) respectively, when compared with the equivalent systemic dosage.
The rabbits were divided into 2 groups (Group I and Group II) according to the concentration of the injected solution. Rabbits in Group I (n=5) were injected with 0.1 mL lornoxicam solution, having a concentration of 250 μg/mL. Rabbits in Group II (n=5) were tested for the effects of 1,500 μg/mL lornoxicam solution (0.1 mL). Each concentration was intravitreally injected randomly in 1 eye (experimental eye) of each rabbit, while in the other eye (control eye) 0.1 mL of sterile balanced saline solution was injected.
For evaluation of vitreal clearance 30 eyes (15 rabbits) were injected with 0.1 mL lornoxicam solution 250 μg/mL.
Evaluation of retinal toxicity
Retinal toxicity was assessed by means of clinical inspection by slit lamp, indirect ophthalmoscopy, intraocular pressure (IOP) measurements, electroretinogram (ERG) recordings, and histological evaluation of the retinal tissue at the end of the follow-up period. All clinical examinations were performed prior to the intravitreal injection and at days 1, 15, and 30 after the injection. After the last ERG recording session, the rabbits were sacrificed by intravenous injection of an overdose of pentobarbital sodium (80 mg/kg body weight), and their retinas were prepared for histological evaluation using light microscopy to assess possible histological alterations of the retinal tissue. All animals were evaluated prior to the experiment for any media opacities or retinal damage.
Evaluation of vitreous clearance
For the determination of the vitreous clearance of the drug, both eyes of 15 rabbits were intravitreally injected with 250 μg/0.1 mL solution of lornoxicam (vitreous clearance evaluation followed the study of retinal toxicity, thereby the dose that did not demonstrate signs of retinal toxicity was chosen). The eyes of 3 rabbits were enucleated at time points 0, 1, 2, 6, and 24 h after the injection was performed. The eyes were enucleated and immediately placed at −80°C conditions. The frozen vitreous was eviscerated whole from all eyes 6 ; about 1.1±0.2 mL of vitreous was collected from each eye. The samples were mechanically homogenized for 2 min, placed in eppendorf tubes, vortexed for 5 s, and centrifuged at 14,000 rpm for 3 min. A quantity of 0.4 mL of sample was diluted with 0.8 mL of acetate buffer 0.5 M, pH 4.1. Liquid–liquid extraction 7 was performed with 2×2 mL of dichloromethane-ethylacetate (1:1 v/v). The organic phase was separated by centrifugation at 4,000 rpm for 5 min, evaporated to dryness under a gentle nitrogen stream, and redissolved in 0.1 mL of methanol. A reversed-phase high-performance liquid chromatography method was carried out using a Discovery C18, 5 μm, 250×4.6 mm ID column. The mobile phase consisted of KH2PO4 (pH=4.7, 0.05 M): acetonitrile: methanol (50:25:25) and the injection volume was 20 μL. The elution conditions were isocratic and the mobile phase flow-rate was set at 0.6 mL/min. Lornoxicam was detected at 372 nm with a UV/VIS detector and the retention time was 10.7 min. The recovery of lornoxicam was calculated at 69% and the limit of determination at 0.2 μg/mL.
Intravitreal injection
All procedures (for both retinal toxicity and clearance evaluation) were performed under sterile conditions using an operating microscope for visualization. A 30-gauge needle attached to a 1.0 mL tuberculin syringe was inserted into the vitreous ∼1 mm posterior to the limbus. The syringe was directed toward the center of the vitreous. A volume of 0.1 mL was then slowly injected. To avoid drug reflux following the injection the syringe remained in the vitreal cavity for 15 s and then was retrieved slowly.
Tonometry
IOP measurements were performed using a calibrated Tono-Pen XL (Medtronic Solan). 8 Every value represents the average of 5 consecutive measurements.
Electroretinography
The examination was performed in accordance with the mentioned methods by Tsilimbaris et al. 9 Prior to ERG recordings the pupils were fully dilated by topical application of phenylephrine (2.5%) and tropicamide (0.5%). The full-field light-evoked ERG was recorded from the experimental and control rabbit eyes using the computerized Primus 2.5 system (Tomey), utilizing Ganzfeld stimulation with a maximum flash intensity of 3.5 cd s/m2. An active electrode (HK loop electrode by Medelec, Oxford Instruments), placed in the lower palpebral sac was referenced to a 9 mm cup silver-silver chloride electrode (Oxford Instruments) placed near the orbital rim (rabbit hair was previously shaved to improve conductivity). For ground electrode, an earring clip was placed at the earlobe. Electrical impedance was smaller than 5 kΩ for all electrodes. Data were sampled at a rate of 1,000 Hz, constrained by online band-pass filtering between 0.3 and 300 Hz. ERG signals were amplified (x5 K), while artifactual signals (e.g., blinks) were automatically removed. ERG responses were initially recorded in the light-adapted state (background luminance of 25 cd/m2) and then in dark-adapted state, following 30 min of dark adaptation. Two ERG responses were recorded: (1) photopic flash responses (average response of 4 consecutive events of 1 Hz frequency and 2.5 cd s/m2 intensity each), (2) scotopic flash responses (average response of 4 consecutive events of 1 Hz frequency and 2.5 cd s/m2 intensity). ERG analysis for flash responses was based on measurements of the b-wave amplitude, from the trough of a-wave to the peak of b-wave.
Histology
After enucleation, the eyes were prefixed in cold glutaraldehyde 2.5% in 0.1 M cacodylate buffer (pH 7.4). After short prefixation, posterior segments were removed from all eyes and were placed in the same fresh fixative. Tissue samples were postfixed in 1% osmium tetroxide in 0.1 M cacodylate buffer (pH 7.4) for 1 h at 4°C, dehydrated in a series of alcohols and propylene oxide, and then imbedded in epoxy resin. For light microscopic examination, 1 to 3 μm sections were prepared and stained with rapid trichrome 5%. 10 The examination was performed with a Diaplan binocular microscope.
Statistical analysis
The significance of the IOP and time, and that of b-wave amplitude and time was statistically evaluated using 2-way ANOVA with repeated measures. A P-value lower than 0.05 was considered statistically significant.
Results
Clearance of lornoxicam from the vitreous
Intravitreal lornoxicam decreases from 127.7±5.9 μg/mL at 0 h to 78.5±14.5 μg/mL at 1 h, to 55.6±4.6 μg/mL at 2 h, to 10.9±1.7 μg/mL at 6 h, and to 0.6±0.2 μg/mL at 24 h. The mono-exponential regression line shown in Fig. 1, demonstrates lornoxicam vitreous concentration in respect with time. Lornoxicam (intravitreal injection of 250 μg/0.1 mL) is eliminated from the vitreous by a first-order kinetic process with an elimination rate constant of 0.415h−1 and a half-life of 1.7 h.
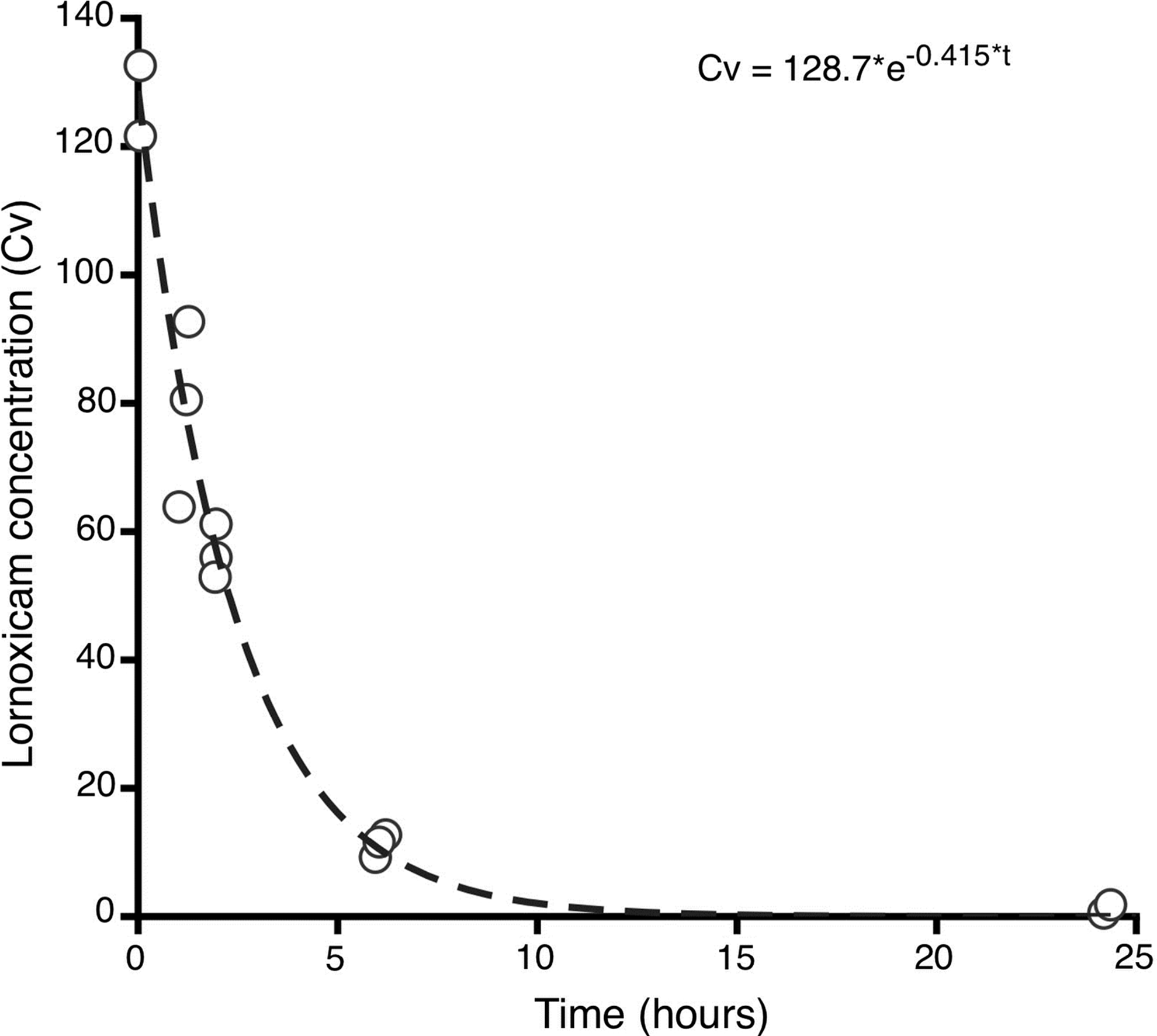
Lornoxicam concentration in the vitreous of rabbits after a single intravitreal injection as a factor of time. The data represent the mean drug concentration. Cv represents lornoxicam concentration in the vitreous and t is time.
ERGs and IOP
Characteristic waveforms of grand-averaged photopic and scotopic flash ERGs for groups I and II are shown in Fig. 2. A decrease in amplitude in both photopic and scotopic ERG values was observed for group II experimental eyes 1 day after intravitreal injection of lornoxicam; this decrease did not reach statistical significance (P=0.08). Repeated measures ANOVA demonstrated no significant effects between photopic flash b-wave and time [F(3, 24)=0.112, P=0.952], or between scotopic flash b-wave and time [F(3, 24)=1.918, P=0.568].
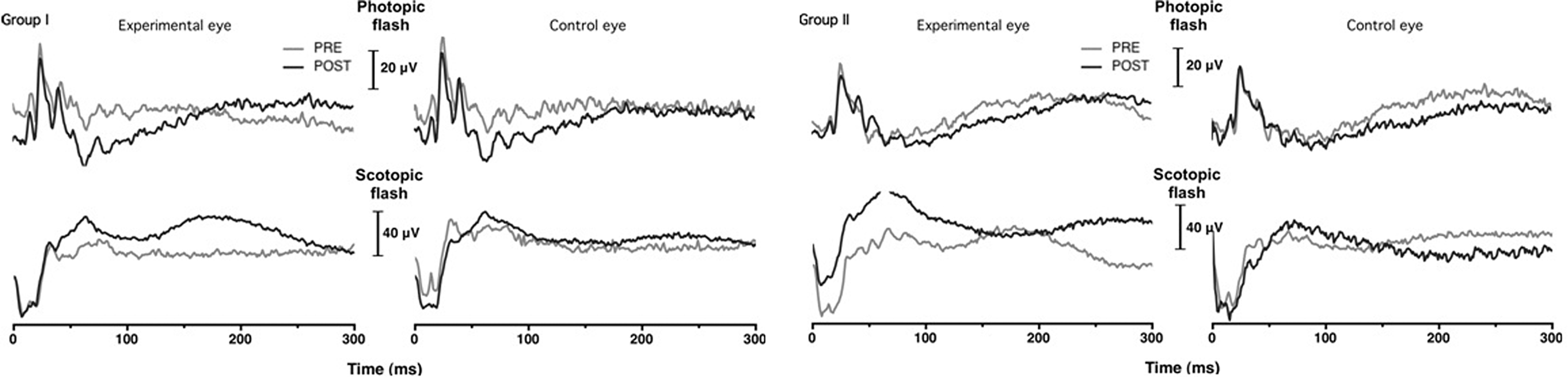
Grand-averaged (n=5) full-field light-evoked photopic and scotopic electroretinogram waveforms for experimental (left) and control (right) eyes of groups I and II at: (1) one day prior to the injection (PRE—light grey lines) and (2) 30 days following the injection (POST—dark grey lines). Group I received 250 μg, whereas Group II received 1,500 μm of lornoxicam solution.
Concerning IOP measurements, in group I, IOP prior to the intravitreal injection was 10.0±0.9 mmHg and 11.9±1.8, 10.3±0.7 and 10.5±2.7 at days 1, 15, and 30 postinjection, respectively. In group II, IOP prior to the intravitreal injection was 10.5±1.6 mmHg and 10.7±1.1, 11.7±4.0 and 9.7±0.9 at days 1, 15 and 30 post injection, respectively. Repeated measures ANOVA demonstrated no significant effects between IOP and time [F(3, 24)=0.979, P=0.419].
Biomicroscopy
Biomicroscopical evaluation of animals of both groups revealed no signs of macroscopic ocular toxicity. Specifically, no signs of intraocular inflammation, corneal or lens opacities, or retinal findings were seen. Minor conjunctival irritation at the site of injection was temporary, subsiding during the follow-up time in all cases. Behavior of all animals remained normal during the follow-up time.
Histology
Light microscopy of the retinal specimens revealed normal retinal anatomy with no signs of induced toxicity (Fig. 3A and 3B) for both control and treated eyes in group I. On the contrary, histological evaluation of all the experimental eyes (5 eyes) of group II, which were injected with 1,500 μm/0.1 mL lornoxicam solution revealed signs of retinal toxicity and histological alterations. Specifically, all eyes demonstrated areas with disorganization and morphological alterations at the level of the inner nuclear and outer plexiform layers. Disappearance of normal stratification of outer retina with vacuolization and thinning was evident (Fig. 4B and 4C). In some areas, total disappearance of nuclear bodies of the outer nuclear layer was observed. Moreover, disconnection between the cells of the outer nuclear layer and the pigment epithelial cells could be seen (Fig. 4B). Pigment epithelial cells preserved their contacts with the Bruch's membrane in all specimens. No desquamation or degeneration of pigment epithelial cells was observed. Histological evaluation revealed that the induced retinal morphological changes had a segmental character, occurring only in parts of the retinal tissue, while neighboring areas remained normal. The control eyes of group II did not demonstrate any signs of retinal toxicity; retinal histology in these eyes was normal (Fig. 4A).

Retinal histological images of Group I animals (injected with 250 μg/0.1 mL lornoxicam) for both the control
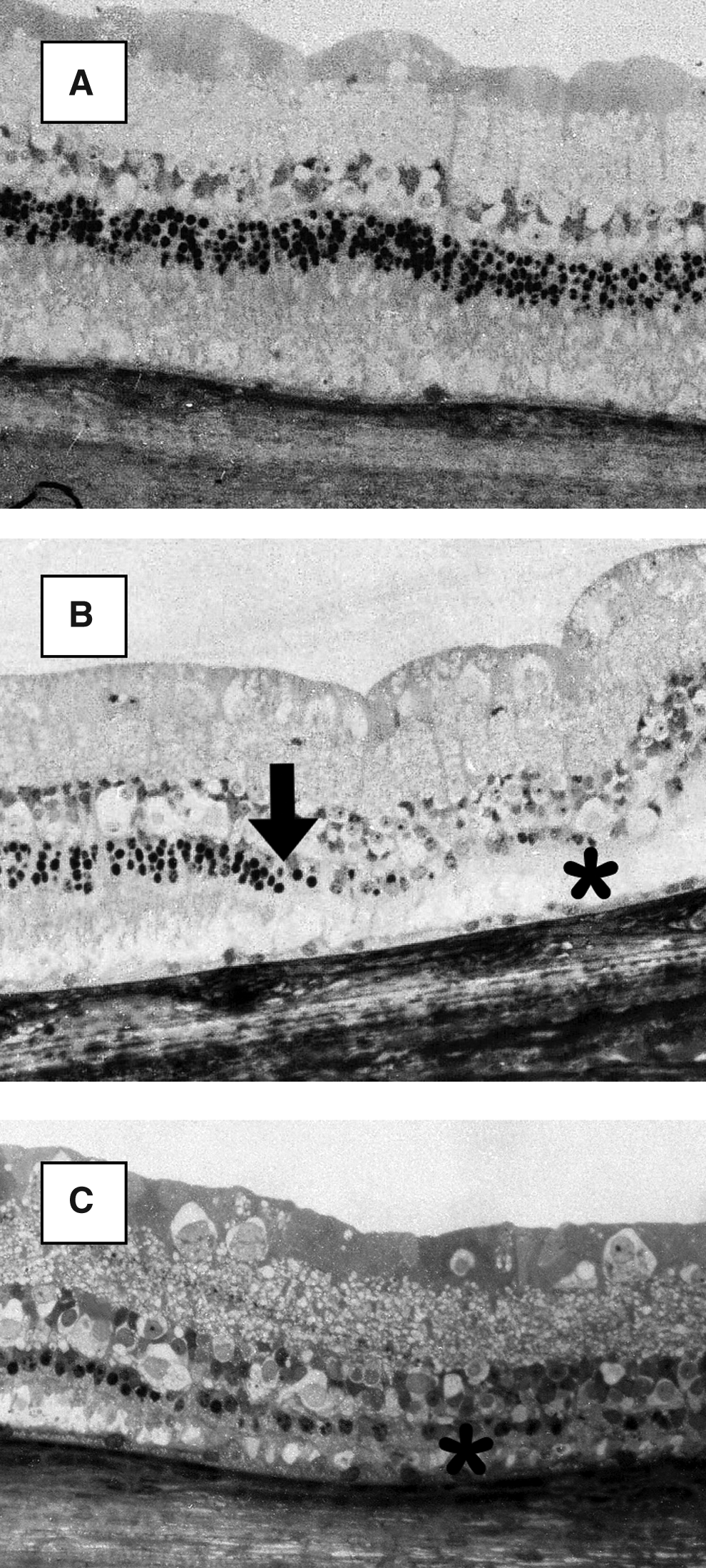
Retinal histological images of Group II animals (injected with 1,500 μg/0.1 mL lornoxicam).
Discussion
Topical application of medication is sufficient for anterior segment disorders, but usually does not achieve delivery of adequate levels at the posterior segment and at the level of the retinal tissue. To overcome this limitation, the use of intravitreal injections has been introduced. This approach offers direct drug delivery into the eye, and a high local concentration is achieved using a relatively small dose compared with systemic dosing. Despite the fact that intravitreal injections have been associated with such complications as endophthalmitis, 11 cataract development, 4 and retinal detachment, 12 their practice has been established due to the significant therapeutic capabilities they demonstrate.
Inflammatory intraocular conditions or conditions with an inflammatory component such as posterior uveitis, postoperative cystoids macular edema, diabetic macular edema, and vascular occlusion related macular edema, are conditions for which treatment approaches include interference on the inflammatory cascade with drugs that are delivered topically, systemically, or intravitreally. Today, corticosteroids represent the only anti-inflammatory drugs that are delivered by means of intravitreal injections. Intravitreal corticosteroids are effective but their use can be complicated with cataract development and increase of IOP.
NSAIDs also interfere with the inflammatory cascade by inhibition of COX and the synthesis of prostaglandins, and they might represent a good candidate for intravitreal administration. NSAIDs may overcome some adverse effects of corticosteroids, such as cataract development and IOP elevation.3–5 There have been several publications that evaluate the safety and efficacy of intravitreal Ketorolac 13 ; this non selective COX inhibitor demonstrates a satisfactory safety profile along with significant therapeutic potentials. Further, it has been reported that intravitreal delivery of Ketorolac achieves high drug concentration at the level of the retina. 13 Ketorolac has been evaluated for the treatment of choroidal neovascularization and diabetic macular edema, demonstrating promising outcomes.14,15
In our study we evaluated lornoxicam's intravitreal behavior by testing 2 doses of lornoxicam with respect to retinal toxicity, IOP changes, and biomicroscopical changes; further we evaluated the vitreal clearance of the drug. Lornoxicam is a NSAID of the oxicam class with analgesic, anti-inflammatory, and antipyretic properties. It is available in oral and parenteral formulations. Like other NSAIDs, lornoxicam inhibits prostaglandin biosynthesis by blocking the enzyme COX. Lornoxicam inhibits both isoforms in the same concentration range, that is, the ratio of COX-1 inhibition to COX-2 inhibition is 1:1.
The half-life of intravitreal lornoxicam was found to be 1.7 h. Small molecular weight substances such as lornoxicam are expected to have short half-lives in the vitreous. This finding is consistent with the intravitreal half-life of ketorolac, 13 another NSAID. Such a small half-life may indicate that repeated injections would be necessary to achieve prolonged therapeutic levels. Since drug concentration begins to diminish soon after the injection has been performed, increase of the intravitreal dose might be another alternative to extend the presence of the drug in the vitreous cavity. However, for drugs that are eliminated from the vitreous following first-order kinetics, doubling the dose would prolong its effect for only 1 half-life. Doubling the dose, on the contrary, increases the possibility of drug-induced retinal toxicity. Drug entrapment in slow-release vehicles might represent a more safe and effective way to prolong the intravitreal half-life to avoid both repeated injections and increase in dose.
Retinal toxicity assessment of lornoxicam included ERG recordings, histological findings, and clinical inspection. Concerning the low dose eyes of Group I (250 μg/0.1 mL solution of lornoxicam–a dose 30 times greater when compared with systemic equivalent) no findings of retinal toxicity were demonstrated in any examination; on the contrary, histological findings of retinal toxicity were revealed in the high dose eyes of Group II (1,500 μg.0.1 mL solution of lornoxicam–a dose 185 times greater when compared with systemic equivalent) with all study eyes presenting areas of retinal atrophy and disorganization at the level of the inner nuclear and the outer plexiform layers. Even though Group II demonstrated histological findings of retinal toxicity, the ERG measurements did not reveal any statistical significant difference between the control and experimental eyes. An explanation for this contradictory result may be that the extent of retinal damage observed in histology might not be enough to induce significant ERG findings. It is known that significant changes in ERG occur after extended damage of the retinal tissue; in our specimens, however, areas of toxicity were interchanging with normal areas.
In our study, we found that lornoxicam is toxic to the retina in a dose-related fashion, as it has been demonstrated for diclofenac. 16 As described by Shen et al. 16 intravitreal injection of 540 μg or higher doses of diclofenac resulted in ocular toxicity in rabbits, demonstrated as cataract, vitreous haze, and retinal damage observed by indirect ophthalmoscopy and light- and electron-microscopic examinations. No toxicity was observed in the eyes that received lower concentrations of diclofenac (400 μg or less diclofenac/HA).
Even though we evaluated the dose-related toxic effects of lornoxicam, we did not quantify the concentration of this agent at the level of the retinal tissue. This may be considered as a limitation of this study, since the target tissue of intravitreal drug delivery is the retina. Future studies need to determine this aspect providing information important in respect with the therapeutic capabilities of lornoxicam. Further, our study is lacking a histological evaluation of the crystalline lens. Although no cataract development or lens opacifications were revealed using the slit-lamp examination, a histological evaluation would be more conclusive in respect to possible toxic effects at the level of the crystalline lens. Finally, the 1 month follow-up used in this study may not be sufficient for cataract development after intravitreal delivery of lornoxicam, and thereby longer follow-up may be necessary to draw final conclusions. Moreover, future research should attempt a more comprehensive evaluation of the dose response and time course of the retinal damage and investigation of potential mechanisms of retinal damage.
In conclusion, an intravitreal dose of lornoxicam lower than or equal to 250 μg does not seem to cause any retinal toxic effects. The intravitreal use of lornoxicam could be considered as an alternative approach for ocular inflammatory conditions. Given the short half-life of the drug after intravitreal injection, strategies for sustained release might be necessary to improve its therapeutic potential. Further studies are necessary for the evaluation of the possible role of intravitreal lornoxicam in clinical practice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.