
Abstract
Abstract
Background:
To determine the adjunctive 24-h efficacy obtained with brinzolamide/timolol, or brimonidine/timolol fixed combinations (FCs) in open-angle glaucoma patients insufficiently controlled on travoprost monotherapy.
Methods:
Prospective, observer-masked, active controlled, crossover, comparison. Qualified primary open-angle or exfoliative glaucoma patients with a baseline intraocular pressure (IOP) >18 mm Hg at 10:00 on travoprost monotherapy were randomized for 3 months to either brinzolamide/timolol, or brimonidine/timolol FC therapy adjunct to travoprost. Patients were then crossed-over to the opposite therapy for another 3 months. At baseline and at the end of each treatment period, the patients underwent 24-h IOP monitoring.
Results:
Fifty patients completed the study. The mean 24-h baseline IOP on travoprost monotherapy was 20.1 mm Hg [95% confidence interval (CI): 19.6, 20.7 mm Hg]. Both adjunctive FC therapies significantly reduced the IOP at each time point and for the mean 24-h IOP (P<0.001) compared with travoprost monotherapy. Brinzolamide/timolol FC provided a significantly lower mean 24-h IOP (17.2 mm Hg, 95% CI: 16.4, 17.9 mm Hg) than brimonidine/timolol FC (18.0 mm Hg, 95% CI: 17.3, 18.8 mm Hg) (P<0.001). For all the 3 timepoints between 18:00 and 02:00, the brinzolamide/timolol FC provided a significantly lower IOP than the brimonidine/timolol FC (P≤0.036). For the other 3 timepoints, no significant differences were detected.
Conclusions:
This study demonstrated that both FCs provide statistically and clinically significant incremental 24-h IOP lowering to travoprost monotherapy. The brinzolamide/timolol FC however achieves a better mean 24-h IOP control owing to the greater efficacy in late afternoon and during the night.
Introduction
Since 1996, when the first topical prostaglandin analog (Latanoprost, Xalatan™) was introduced, the popularity of prostaglandins has increased dramatically mainly due to their improved 24-h efficacy compared to the prior first-line choice, timolol maleate. Prostaglandins have been shown to obtain a clinically significant 24%–29% 24-h IOP reduction. 6 The superior efficacy and the convenience of once-a-day administration allowed prostaglandin analogs to become a first-line treatment of glaucoma worldwide. Nonetheless, between 50%–75% of all glaucoma patients eventually require additional stepwise therapy to further reduce the IOP and prevent progression.7,8
Thus, the clinician frequently needs to introduce adjunctive therapy to the previously established prostaglandin monotherapy. However, which medication is best suited as adjunctive therapy and the efficacy of these options with prostaglandins remain controversial. It has been documented that timolol, a nonselective beta-receptor blocker, provides useful additional IOP lowering when added to a prostaglandin analog in a fixed or unfixed concomitant combination.9–12 Many physicians however are currently prescribing a fixed combination (FC) product as adjunctive therapy to prostaglandin monotherapies when substantial IOP reduction is needed to reach the desired target pressure. 13 The use of an adjunctive FC allows the minimal number of daily application with a potentially maximal therapeutic effect and may increase patient compliance. It is well documented that multiple medications and the complexity of treatment regimen are key determinants of poor adherence. Unfortunately, little is currently known on the 24-h efficacy of FCs when added to prostaglandins. It has been suggested however that additivity of adjunctive options is only partial; IOP reduction decreases with increasing treatment complexity; and the ratio of patients with a clinically meaningful additional IOP reduction is only 40% when a third IOP-lowering topical medication is introduced. 14
It is thus important for stepwise medical therapy to determine which adjunctive FC provides the best incremental 24-h IOP reduction to the available prostaglandin monotherapies. In the current crossover 24-h study, we therefore compared 2 FCs (brinzolamide/timolol and brimonidine/timolol FCs) as adjunctive therapy to travoprost in open-angle glaucoma patients.
Methods
The protocol adhered to the tenets of the Declaration of Helsinki, and was approved by the institutional review board of the Medical School of Aristotle University of Thessaloniki. Written informed consent was obtained from all study participants before enrolment. The study was registered with clinicaltrials.gov (identifier: NCT00981786). Our study was a prospective, observer-masked, active controlled, crossover comparison. We enrolled consecutive patients older than 29 years of age with early-to-moderate glaucoma (POAG or XFG) who were insufficiently controlled on monotherapy with travoprost 0.004% (Travatan; Alcon Laboratories Hellas, Greece). In the current study, early-to-moderate glaucomatous damage was defined as glaucomatous visual field damage <16 dB on the Humphrey SITA Standard perimetry program and the cup-to-disc ratio ≤0.8. Inclusion criteria were an initial, untreated morning (10:00±1 h) IOP reading >25 mm Hg; a mean morning IOP (10:00±1 h) >18 mm Hg ascertained by 2 separate measurements in 2 different visits on evening administered travoprost monotherapy; at least 20% morning IOP reduction from the untreated baseline on travoprost monotherapy; a need for further IOP reduction to achieve the desired target IOP as determined by the principal investigator; a neuroretinal rim and/or visual field damage typical for glaucoma; open angle with gonioscopy in both eyes; central corneal thickness of 500–600 microns; and best-corrected Snellen visual acuity better than 0.1.
Exclusion criteria were a history of nonadherence; <10% IOP decrease to any IOP-lowering medication; allergy, intolerance, or contraindication to travoprost, timolol, brimonidine, or brinzolamide; history of ocular trauma, inflammation, intraocular surgery, and use of topical corticosteroids in the last 3 months before entering the study; severe dry eyes; use of contact lenses; sign of ocular infection except for mild blepharitis; any corneal abnormality that could have affected the measurement of the IOP; being a woman of childbearing potential or a lactating mother; and an inability to understand the instructions and adhere to medications. The demographics of the participants are shown in Table 1.
POAG, primary open-angle glaucoma; XFG, exfoliative glaucoma; SD, standard deviation.
Qualified patients were asked to apply travoprost at 8.15
Statistics
Assuming a standard deviation of 2.4 mm Hg, the design provided an 80% power for detection of a 1.0 mm Hg difference between the treatment groups if 48 patients complete the study. The primary efficacy endpoint was the mean 24-h IOP (the average pressure for the 6 timepoints). The individual timepoints, peak, trough, and the fluctuation of 24-h IOP were included as secondary endpoints. A mixed model was used for the crossover repeated-measures design to adjust for period and carryover effects. 14 A 95% CI was constructed for the adjusted difference in means. An intention-to-treat approach was adopted, and the subjects were analyzed according to their randomized group.
The rate of the adverse events during the study between the treatment periods were evaluated by Cochran's Q test for patients that completed the study, while between the adjunctive FC periods were evaluated by McNemar's test. The Bonferroni-adjusted P-values are reported to correct the analyses for multiple comparisons in secondary endpoints. All other reported P-values were 2-tailed with P<0.05 considered as significant. Analyses were conducted using PASW Statistics 18.0 (IBM SPSS, Somers, NY).
Results
Of the 63 patients enrolled in the study, 50 subjects (54% women and 46% men; 66% POAG, 34% XFG) competed the study. Of the 13 study patients who did not complete the study, 6 did not meet the study IOP inclusion criterion for travoprost monotherapy, and they were excluded. Two patients withdrew after the first curve due to difficulties in undergoing repeated 24-h IOP monitoring; 5 patients who were randomized to the adjunctive FC therapies were withdrawn due to adverse events: 3 in the brimonidine/timolol FC period and 2 in the brinzolamide/timolol FC period.
The age (mean±SD) of trial participants was 64.2±9.8 years. Fifty patients were randomized, resulting in 23 receiving adjunctive brinzolamide/timolol FC and 27 receiving brimonidine/timolol FC. The individual time points, mean, peak, trough, and 24-h IOP fluctuation are shown in Table 2. The 24-h baseline IOP on travoprost monotherapy was 20.1 (95% CI: 19.6, 20.7 mm Hg). After the addition of the FC therapies, both treatment groups showed significantly reduced pressure at each time point and for the mean, peak, and trough 24-h IOP, when compared to travoprost monotherapy (P≤0.024 for all comparisons). Brinzolamide/timolol FC further reduced the 24-h travoprost-treated IOP by 3.0 mm Hg (14%), whereas brimonidine/timolol FC further reduced 24-h travoprost-treated IOP by 2.1 mm Hg (10%).
Adjusted for period and carryover effect.
Significant differences compared to travoprost monotherapy (P≤0.024).
Bonferroni-adjusted P-values for the comparisons between brinzolamide/timolol FC+travoprost and brimonidine/timolol FC+travoprost therapies.
FC, fixed combination; CI, confidence interval.
When the 2 FCs were compared directly, the brinzolamide/timolol FC added to travoprost provided a significantly lower mean 24-h IOP (17.2 mm Hg, 95% CI: 16.4, 17.9 mm Hg) than the brimonidine/timolol FC (18.0 mm Hg, 95% CI: 17.3, 18.8 mm Hg) (P<0.001) (Fig. 1). Interestingly, brinzolamide/timolol FC performed significantly better than brimonidine/timolol FC at all 3 time points between 18:00 and 02:00 (P≤0.036, for these time points). For the other 3 time points, no difference was detected between the 2 FCs (P>0.05). The peak and trough 24-h IOP values were significantly lower with adjunctive brinzolamide/timolol FC therapy (P<0.001 and P=0.002, respectively). However, no significant difference in the 24-h IOP fluctuation was observed between the 3 treatment options (travoprost: 3.7 mm Hg, 95% CI: 3.4, 4.0 mm Hg; travoprost and brinzolamide/timolol FC: 3.6 mm Hg, 95% CI: 3.2, 4.1 mm Hg; and travoprost and brimonidine/timolol FC: 4.3 mm Hg, 95% CI: 3.8, 4.8 mm Hg) (P>0.05, for all comparisons).
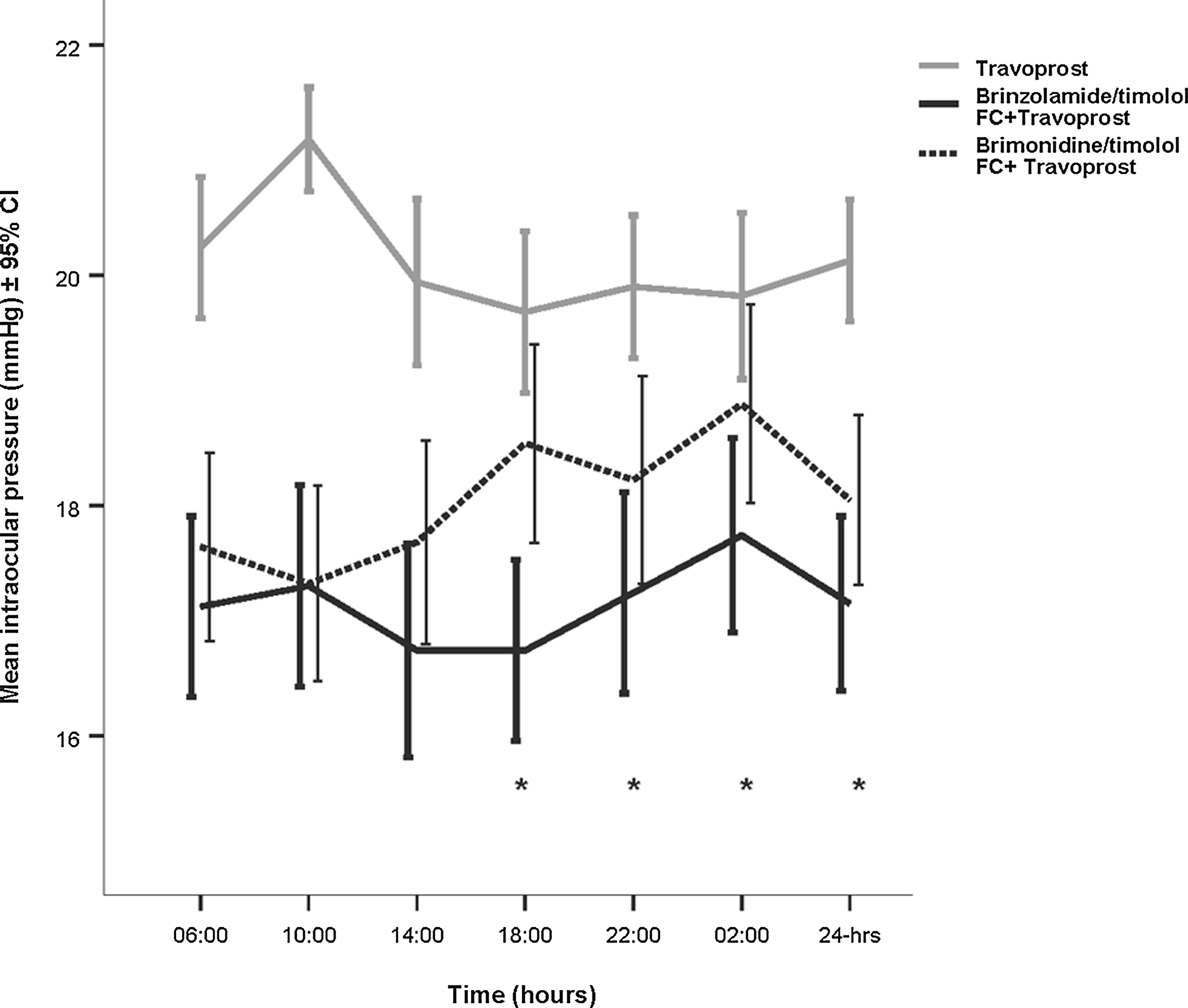
Mean intraocular pressure±95% confidence interval (CI) at each individual time point and for the 24-h pressure for the travoprost (gray solid line), brinzolamide/timolol fixed combination (FC)+travoprost (solid black line), and brimonidine/timolol FC+travoprost (black dotted line) treatment groups. Significant differences (Bonferroni adjusted P-values<0.05) between the adjunctive FC treatment groups are denoted with an asterisk (*).
The difference in the 24-h mean IOP reduction achieved with brinzolamide/timolol FC and brimonidine/timolol FC when added to travoprost is shown in Table 3. After adjustment for period and carryover effect, brinzolamide/timolol FC obtained significantly a greater mean 24-h IOP reduction (0.9 mm Hg, CI: 0.5, 1.3 mm Hg) than brimonidine/timolol FC as adjunctive therapy to travoprost (P<0.001). No period effect and carry over effect were found in the present study.
Adjusted for period effect (P=0.339) and carryover (P=0.901).
IOP, Intraocular pressure.
All 3 therapy options were well tolerated, but as expected, ocular and systemic adverse events were more frequent in the adjunctive FC treatment periods compared with travoprost monotherapy (Cochran's Q test, P=0.031 and 0.001, respectively). When the 2 FC treatments were compared (Table 4), transient blurring of vision occurred significantly more often in the adjunctive brinzolamide/timolol FC period (P=0.002), whereas itchiness and hyperemia occurred more frequently in the brimonidine/timolol FC period (P=0.016 and P<0.039, respectively). No significant difference was detected with regard to the other adverse events (P>0.05). The rate of systemic adverse events was similar with the 2 FCs, except for fatigue, which was more common in the brimonidine/timolol FC period (P=0.05).
Some patients experienced multiple adverse events.
Discussion
In the present study, we compared for the first time the 24-h IOP efficacy provided by the brinzolamide/timolol FC versus with that of the brimonidine/timolol FC when they are employed as adjunctive therapy to glaucoma patients insufficiently controlled with travoprost monotherapy. The results of this investigation demonstrate that both FCs significantly reduce the 24-h IOP from travoprost baseline and provide clinically meaningful incremental IOP reduction (10%–14%). The brinzolamide/timolol FC provided a statistically superior quality of 24-h IOP lowering.
This investigation sought to better understand the potential differences between available FCs when they are selected as adjunctive therapy in patients insufficiently controlled on prostaglandin monotherapy. The use of more complex medication regimens, comprising a prostaglandin analog and an FC, are often needed in clinical practice. However, as of yet, there is limited evidence and no comprehensive guideline on how to optimize the selection of available FCs to the stepwise therapy ladder of prostaglandin-treated patients. Specifically, there is no controlled evidence on the efficacy of brinzolamide/timolol FC as adjunctive therapy to prostaglandin monotherapies and, as yet, no direct comparative data between brinzolamide/timolol and brimonidine/timolol FCs as adjunctive therapies to prostaglandins. A previously published 24-h study has investigated the incremental efficacy of dorzolamide/timolol FC to latanoprost, 13 and a peak and trough prospective study investigated the efficacy of brimonidine/timolol FC as adjunctive therapy to latanoprost. 15
In a randomized, double-masked, multicenter, 3-month trial, it was shown that twice-daily brinzolamide 1% provides a significantly lower mean daytime IOP than twice-daily brimonidine 0.15% when it is used as adjunctive therapy to travoprost. 16 In another crossover study, 17 which employed 3 IOP measurements timepoints (8:00, 12:00, and 16:00), the efficacy of brimonidine/timolol FC was similar to that of dorzolamide/timolol FC in open-angle glaucoma patients. In this small, 1-month study, the baseline IOP was relatively low (22.9 mm Hg), and probably could not optimally separate the efficacy of these 2 FCs. When these FCs were compared recently over 24 h, 18 dorzolamide/timolol FC was found to be superior to brimonidine/timolol FC at 2 individual time points (18:00 and 02:00), as well as for the mean (−0.7 mm Hg), peak, and trough 24-h IOP. Since a comparative trial of dorzolamide/timolol versus brinzolamide/timolol FC has shown that these 2 FCs provide similar (30%–33%) IOP lowering for up to 1 year of treatment, 19 this evidence implies that on a direct comparison, brinzolamide/timolol may also be superior over 24 h than brimonidine/timolol FC. This may not be the case; however, since efficacy decreases with increasing number of medications, and the potency of FCs may be somewhat different in conjunction with prostaglandins.13,14,20 Thus, evaluation of the additional IOP lowering induced by different FCs when they are added to a prostaglandin required specific controlled evidence.
This investigation has demonstrated that both adjunctive FC therapies significantly reduce the IOP at each time point and for the mean 24-h curve compared with travoprost monotherapy. Thus, both FCs are clinically valuable when further IOP reduction is needed in open-angle glaucoma patients inadequately controlled on travoprost monotherapy. However, the additional 24-h IOP decrease was greater with the brinzolamide/timolol FC (17.1 mm Hg) compared with the brimonidine/timolol FC (18.0 mm Hg). Further, at 3 timepoints (18:00, 22:00, and 02:00), adjunctive brinzolamide/timolol FC therapy provided a significantly lower IOP than adjunctive brimonidine/timolol FC therapy, with the mean differences ranging 1.0–1.8 mm Hg, respectively. For the other 3 timepoints, no significant difference could be detected between the 2 adjunctive FC therapies. The reduced efficacy of brimonidine/timolol FC late in the afternoon and during the night is consistent with previously published evidence. In previous daytime studies,21,22 the range of IOP reduction by brimonidine/timolol FC was between 4.4 to 7.6 mm Hg and 4.4 to 5.3 mm Hg. It is worthy to note that although brimonidine/timolol FC reduced the morning IOP by 28% from untreated baseline and by 1.6 mm Hg from timolol baseline, 23 the afternoon time points (15:00 and 17:00) showed only a 0.6- and 0.0-mm Hg further IOP reduction, respectively, compared to timolol monotherapy. As indicated before, a recent 24-h study 18 also reported a reduced efficacy for brimonidine/timolol FC late in the afternoon and during the night. This is further substantiated by previous published 24-h efficacy evidence on brimonidine.24–26 In contrast, cumulative 24-h evidence 6 suggests a longer duration of action and a better nighttime efficacy for carbonic anhydrase inhibitors. These data may account for the better 24-h efficacy of the brinzolamide/timolol FC when added to travoprost.
No significant difference could be demonstrated in terms of 24-h IOP fluctuation for the 2 FCs investigated. This may be due to the narrow 24-h IOP fluctuation (3.7 mm Hg) already obtained with travoprost monotherapy.3,4 Unsurprisingly, both ocular and systemic adverse events were more common with the FC and travoprost combined therapy. The only significant differences in terms of adverse events between the 2 FCs were the incidence of transient blurred vision, which occurred in 20% of those in the brinzolamide/timolol treatment period, while itchiness and hyperemia were more common (18% and 16%, respectively) with the brimonidine/timolol FC treatment.
To the best of our knowledge, this controlled, crossover 24-h study is the first comparison of brinzolamide/timolol FC and brimonidine/timolol FC as adjunctive therapy in POAG or XFG patients insufficiently controlled on travoprost monotherapy. The present study was short term. Future studies are needed to compare the long-term efficacy of these FCs when added to available prostaglandin monotherapies. FCs and prostaglandins are often employed together as adjunctive therapy in many countries. The present study provided controlled information on the optimal stepwise therapy in glaucoma. Since combination therapy is becoming more common in the long-term management of glaucoma progression, future investigations on long-term safety and efficacy of using different FC therapies in adjunct to a prostaglandin will be of good added value to the body of published literature.
Footnotes
Acknowledgment
This study was supported in part by Alcon.
Author Disclosure Statement
Commercial relationship: A.G.P. Konstas is a consultant of Alcon, Allergan, MSD, NicOx; G. Holló is a consultant of Alcon, Allergan, MSD, NicOx, Pfizer and Santen; A.B. Haidich: none; D.G. Mikropoulos is a consultant of Alcon, Allergan; T. Giannopoulos: none; I.C. Voudouragkaki: none; E. Paschalinou: none; J.R. Samples is a consultant for Alcon, Allergan, MSD, Transcend, Aquesys, Ivantis, Aerie, and a shareholder of Refocus and Eyegenetix; V. Konidaris: none.