
Abstract
Abstract
Purpose:
Our recent study, which involved a randomized, placebo-controlled, double-masked 24-month trial (Ophthalmologica 2012;228:26–35), revealed that oral administration of black currant anthocyanins (BCACs) slowed down the visual field deterioration and elevation of ocular blood flow of open-angle glaucoma (OAG). To elucidate the underlying mechanisms of these BCAC-induced effects, as possible factors affecting glaucomatous optic neuropathy, changes of serum endothelin-1 (ET-1), nitric oxide (NO), and antioxidative activities were examined in the present study.
Methods:
From among patients with OAG who participated in the randomized, placebo-controlled, double-masked trial, serum specimens were obtained from BCAC-treated (n=19) or placebo-treated (n=19) patients at baseline and every 6 months. Healthy volunteers (n=20) with age and gender matching the patients were used as a control. Serum ET-1 concentration, [NO2−] and [NO2− + NO3−] levels, advanced oxidation protein products (AOPP), and antioxidant activities were measured by using commercially available kits.
Results:
At the trial baseline, serum ET-1 concentrations were significantly lower in patients with OAG (BCACs, 3.18±1.06 pg/mL; placebo, 3.44±0.84 pg/mL) than those in healthy volunteers (4.38±1.03 pg/mL) (one-way analysis of variance and a Tukey's multiple comparison post hoc test, P<0.05). Upon administration of BCACs, serum ET-1 concentrations increased to the levels of those in healthy volunteers during the 24-month period. In contrast, those of placebo-treated patients remained at lower levels (3.82±1.14 pg/mL). While [NO2−] and [NO2−+NO3−] levels, AOPP, and antioxidative activities of patients from both the BCACs and placebo groups showed comparable levels to those of healthy subjects at baseline, no significant changes were observed during the observational period in either the BCAC or placebo groups.
Conclusions:
Among the possible beneficial effects of BCACs toward visual field progression in patients with OAG, our present results suggest that BCACs caused normalization of serum ET-1 levels, and this may modulate ET-1-dependent regulation of the ocular blood hemodynamics.
Introduction
Anthocyanins (ACs) are kinds of polyphenols, rich in food and beverages such as red wine, cocoa and berries, and it is widely recognized that consumption of them serves several health benefits, such as antioxidative stress and anti-inflammatory effects.25,26 The ACs in black currants (BC) in particular have been implicated in improvement of visual functions.27–29 In our initial clinical trial, we found that systemic administration of BCACs (50 mg/day) to patients with OAG (n=30) for 6 months caused a significant increase in the blood flows at the ONH (P<0.05). 30 Furthermore, in the subsequent randomized, placebo-controlled, double-masked, 24-month trial, we demonstrated that patients with OAG administered with BCACs showed significantly less deterioration of mean deviation (MD) and increased ocular blood flows in comparison with placebo-treated patients during the 24-month trial period. 31 However, no significant changes in systemic blood pressure, pulse rates, and IOP during the 24-month period were observed in either group, nor were there any systemic or ocular side effects. These results suggested that oral administration of BCACs may be a safe and promising supplement for suppression of visual field deterioration in patients with OAG. Moreover, in addition to their IOP control, the efficacy of the BCACs may have some effects on ocular blood circulation and/or antioxidative stress. Thus, it was of great interest to elucidate what kinds of underlying mechanisms are involved in the BCAC-induced beneficial effects toward GON.
Among the several possible mechanisms obtained by BCACs, our study focused on the following biomarkers. ET-1 has been shown to be implicated in several ocular diseases, including GON, 32 diabetic retinopathy, 33 retinal vein occlusion, and retinal artery occlusion. 34 As for serum ET-1 levels, there are statistically significant differences between patients with glaucoma and control subjects.12–15 According to one report, in vitro, BCACs induced ET-dependent vessel dilatation in the bovine ciliary body. 35 Another factor affecting ocular blood circulation is nitric oxide (NO), a ubiquitous compound in the body that plays an important role in vasodilation via the relaxation of vascular smooth muscle, and hence in increasing circulation in the body. 36 A number of plant polyphenolic compounds, including AC, have been shown to modulate NO levels and/or actions. NO being a gaseous free radical has a half-life of <15 s and is rapidly metabolized to nitrate ([NO3−]) and nitrite ([NO2−]). As such, serum nitrate and nitrite are usually measured to evaluate serum levels of NO. In cases of oxidative stress, advanced oxidation protein products (AOPP) are the products of plasma protein oxidation, especially oxidation of albumin. 37 Because of their rapid response to changes, they are thought to be suitable for measuring short-term changes in oxidative stress. Serum levels are known to correlate with cardiovascular disease markers, and increase in subjects with inflammatory conditions such as ulcerative colitis, ankylosing spondylitis, and renal failure. 38 Increased serum AOPP levels are also reported in some patients with glaucoma.39,40 Regarding antioxidant capacity, living organisms have developed complex antioxidant systems to counteract ROS and reduce their damage. These antioxidant systems include several enzymes such as superoxide dismutase, catalase, and glutathione peroxidase. They also include several macromolecules such as albumin, ceruloplasmin, and ferritin, as well an array of small molecules, including ascorbic acid, alpha-tocopherol, beta-carotene, reduced glutathione, uric acid, and bilirubin. The sum of endogenous and food and/or supplement-derived antioxidants represents the total antioxidant activity of the system. 41
In the present study, we therefore examined the effects of BCACs on the serum biomarkers, serum ET-1 concentration, NO, AOPP, and antioxidant capacity related to ocular blood circulation and oxidative stress using serum specimens obtained from BCAC-treated and placebo-treated patients with OAG participating in a randomized, placebo-controlled, double-masked, 24-month trial. 31
Subjects and Methods
A randomized, double-masked, placebo-controlled single-center trial using 38 patients with OAG meeting the inclusion and exclusion criteria described below was conducted between November 1, 2006, and March 31, 2010, in the glaucoma clinic of the Department of Ophthalmology, Sapporo Medical University Hospital. 31 The experimental protocol is briefly described below. This protocol was approved by the Ethics Committee of the Sapporo Medical University School of Medicine and conducted in accordance with the Declaration of Helsinki. After an explanation of the study's purpose and its protocol were provided, written informed consent was obtained from all participants in our glaucoma clinic before inclusion.
Inclusion and exclusion criteria
From among 250 eligible patients with OAG, a total of 38 patients meeting the following inclusion and exclusion criteria were enrolled in the study.
Inclusion criteria
(1) More than 24 months of treatment by antiglaucoma drops and regularly receiving IOP measurements at 1–2-month intervals and the Humphrey visual field (program 30–2, SITA standard, Humphrey Instruments, San Leandro, CA) at 3–6-month intervals.
(2) Early-to-moderate stages of GON (MD greater than −12 dB) in at least 1 eye.
(3) Best-corrected visual acuity >0.6 at the trial baseline in at least 1 eye.
(4) Reliable performance on the Humphrey visual field testing 30–2 program (fixation loss of <20%, and a false-positive or false-negative response of <33%).
Exclusion criteria
(1) Ocular diseases other than OAG and an early or mild senile cataract that would not influence the Humphrey visual field testing.
(2) No other ocular, neurological, otolaryngological, or systemic diseases affecting optic disc damage.
(3) History of cataract surgery within the previous 24 months.
(4) History of glaucoma surgery.
(5) Use of supplements.
(6) History of drug or food allergies.
Methods
ACs (25 mg) extracted from BCs were packed into the same capsules as placebos, making them indistinguishable to patients or physicians. Based on the assignment list numbers, subjects randomly received daily doses of BCACs (2 capsules, 50 mg/day, n=19) or placebo capsules (n=19) for 24 months. During the follow-up period, glaucoma medications were not altered.
For the measurement of serum levels of ET-1 concentration, NO, antioxidant activities, and AOPP, the subjects were requested to remain in a sitting position quietly for 30 min. Their blood samples (5 mL) were taken in the morning (9–11
As a control, healthy volunteers (n=20, male/female, 10/10; age, 62.35±12.55 years) with age and gender matching the patients with OAG were employed.
Statistical analysis
Several observational data of serum levels of ET-1, [NO2−], [NO2−+NO3−], AOPP, and antioxidative activity of the BCAC-treated and placebo-treated patients with OAG at trial baseline were compared with those of healthy subjects by one-way analysis of variance (ANOVA). Additionally, a Tukey's multiple comparison post hoc test was performed to evaluate differences between the experimental groups. After normal distribution and homogeneity of data were confirmed using the Kolmogorov–Smirnov test and Bartlett test, respectively, above observational data obtained during the 24-month follow-up periods were compared between groups by a 2-way (time, treatment) ANOVA with repeated measures. Intergroup differences of changes of values at each time point from trial baseline in these data were analyzed by a paired t-test.
All statistical analyses were performed with MS-Excel. The significance level was set at P<0.05 for all statistical analysis.
Results
To elucidate underlying molecular mechanisms of BCACs in GON, several serum markers regulating vessel contraction and antioxidative stress, serum ET-1 concentration, NO, AOPP, and antioxidant activity were evaluated in serum specimens obtained from the randomized, placebo-controlled, double-masked, 24-month trial.
Serum ET-1 concentrations in patients from both groups (BCACs, 3.18±1.06 pg/mL; placebo, 3.44±0.84 pg/mL) at the trial baseline were significantly less than those recorded in the healthy control subjects (4.38±1.03 pg/mL) (Table 1, one-way ANOVA and a Tukey's multiple comparison post hoc test, P<0.05). During the 24-month trial, serum ET-1 concentrations of BCAC intake groups increased after 6 months from the baseline and reached levels (6 months; 3.74±1.08 pg/mL, 12 months; 4.12±1.40 pg/mL, 18 months; 4.43±1.52 pg/mL, 24 months; 4.59±1.84 pg/mL) comparable to those the healthy control subjects (4.38±1.03 pg/mL). In contrast, serum ET-1 concentrations in the placebo groups remained at lower levels throughout the 24-month period (24 months; 3.82±1.14 pg/mL, Fig. 1).
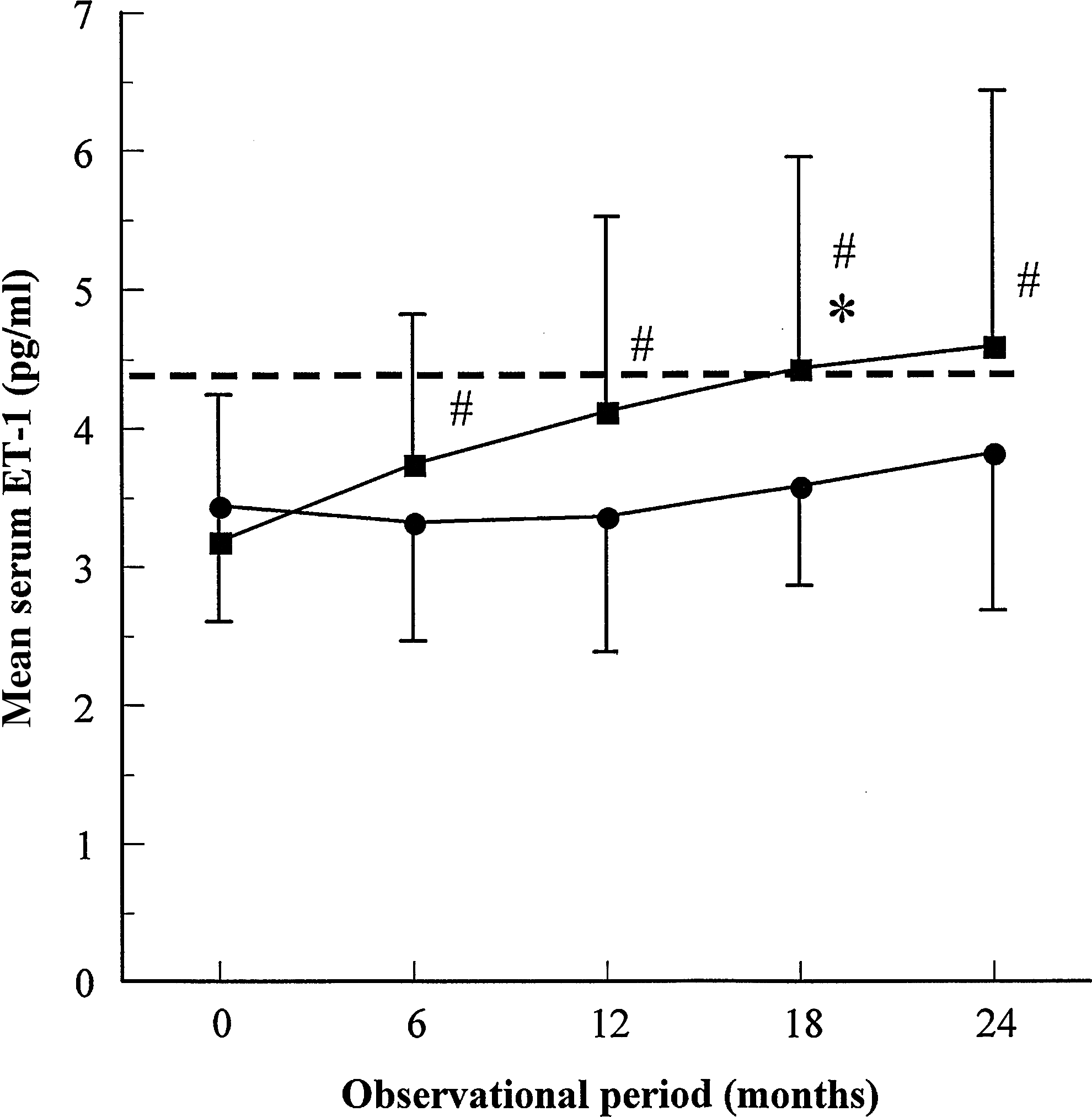
The time course of mean serum endothelin-1 (ET-1) concentrations. Mean serum ET-1 concentrations in the black currant anthocyanin (BCAC)-intake group (N=19, filled square) or placebo-intake group (n=19, filled circle) were plotted at baseline and each time point of trial period (6, 12, 18, and 24 months). Data expressed mean±SD. *: significant difference between groups (P<0.05, 2-way repeated-measure analysis of variance). #: significant intergroups difference between each time point and baseline (P<0.05, paired t-test). Mean serum ET-1 concentrations in the healthy subjects (n=20) are indicated as a dotted line.
Values shown are mean±SD.
Statistical difference with healthy subjects (P<0.05, one-way analysis of variance (ANOVA) and Tukey's multiple comparison post hoc test).
ET-1, endothelin-1; NO, nitric oxide; AOPP, advanced oxidation protein products; OAG, open-angle glaucoma; BCACs, black currant anthocyanins; NO2−, nitrite; NO3−, nitrate.
Patients' serum levels of [NO2−] and [NO2− + NO3−], AOPP, and antioxidative activity were comparable to those of healthy subjects at baseline (Table 1, one-way ANOVA and a Tukey's multiple comparison post hoc test). During the trial period, no significant changes were observed in these analyses between groups and intergroups (Tables 2–4, 2-way repeated measures ANOVA).
Values shown are mean±SD.
No statistical differences between groups (2-way repeated measures ANOVA) and intergroups (paired t-test) were observed.
Values shown are mean±SD.
No statistical differences between groups (2-way repeated measures ANOVA) and inter-groups (paired t-test) were observed.
Mean±SD (all such values).
No statistical differences between groups (2-way repeated measures ANOVA) and intergroups (paired t-test) were observed.
Discussion
Berries are known to be a fine source of polyphenols, especially ACs, micronutrients, and fiber. Epidemiological and clinical studies have shown that these constituents have been associated with several health benefits. 42 Human intervention studies using berries (either fresh, as juice, or freeze-dried), or purified anthocyanin extracts have demonstrated significant improvements in antioxidant activities, including low-density lipoprotein oxidation and lipid peroxidation.43,44 These benefits were recognized in healthy subjects as well as in those with existing metabolic risk factors. It has been suggested that underlying mechanisms of these beneficial effects include upregulation of endothelial NO synthase, decreased activities of carbohydrate-digestive enzymes, decreased oxidative stress, and inhibition of inflammatory gene expression. BCACs additionally possess antioxidant 45 and anti-inflammatory properties. 46 They are also especially known to induce beneficial effects toward visual functions such as improved adaptation to dark and video display terminal work-induced transient refractive alteration in healthy human volunteers, 27 in addition to slowing down GON progression. 31 Although the mechanisms underlying these ocular beneficial effects are unknown, it is thought that upon oral administration, intact forms of BC ACs are absorbed and transferred beyond both the blood–aqueous barrier and the blood–retina barrier into ocular tissues, including the retina, choroid, and ciliary body,47,48 resulting in beneficial biological activities. In fact, in vitro experiments have demonstrated that BCACs transferred into ocular tissues caused several ocular effects, including stimulation of rhodopsin regeneration in frog retinas, 28 suppression of ocular globe elongation in chick myopia models, 29 and the ET-dependent vasodilation in the bovine ciliary body. 35 In the present study, to elucidate possible mechanisms of BCACs demonstrating beneficial effects toward GON progression, we assayed several serum biomarkers obtained from BCAC-treated and placebo-treated patients with OAG who had participated in our previous randomized, double-masked 24-month trial. 31 We found that continuous supplementation of BCACs caused normalization of decreased levels of serum ET-1 concentrations in patients with OAG. In contrast, serum NO levels and antioxidative stress activities were not affected. Consequently, we concluded that BCAC-induced beneficial effects toward GON progression may primarily be ascribed to an ET-dependent mechanism.
ET-1 is a potent vasoconstrictor believed to play a role in local autoregulation of blood flow.49,50 It is produced by the vascular endothelial cells and released primarily abluminally. The ET-1 receptors (ETA and ETB) belong to the family of G-protein-coupled receptors. 50 Within ocular tissues, ETA and ETB are constitutively expressed in human uveal tissues, 51 the retina, and ONH. 52 ETA is mainly present on the vascular smooth cells and is responsible for the vasoconstriction caused by ET-1, and ETB is mainly present on the vascular endothelium and is believed to produce transient vasodilatation through release of NO.49,50 High levels of serum ET-1 have been shown in several diseases characterized by abnormal vasoreactivity, among them Raynaud's phenomenon, diabetes, and ischemic heart disease. 53 ET-1 is therefore believed to be pivotally involved in the pathogenesis of these diseases. A number of previous cross-sectional studies have shown that basal levels of plasma (or serum) ET-1 in patients with glaucoma were elevated at a higher level than control subjects.12–14 Conversely, other studies showed no significant difference in plasma (or serum) ET-1 between subjects with glaucoma patients and normal control subjects54–57 or lower levels of plasma ET-1 in patients with glaucoma when compared with normal subjects. 15 Although the conflicting conclusions indicate that no consensus regarding plasma (or serum) levels of ET-1 in patients with glaucoma have been reached, it is possible that data from all studies are accurate, since plasma (or serum) ET-1 levels may fluctuate due to seasonal, circadian, and other factors.
In our present study, serum ET-1 levels of patients with OAG were significantly lower than those in normal subjects at the trial baseline. These results are consistent with our previous study. 15 Consequently, we speculated that ET-1 receptors may be upregulated in response to the continued lower levels of serum ET-1 levels, since it is known that ET-1 has a positive feedback on the expression of its receptors.49,50 In this situation, a transient increase of serum ET-1 concentrations by cold stimulation may enhance ET-1-induced vasoconstriction (Fig. 2). In fact, previous studies demonstrated that patients with glaucoma, in contrast to the control subjects, have an abnormal hyperactivity of ET-1 in response to vasospastic stimuli such as cold. 58 It has been postulated that an imbalance between vasoconstrictor substances such as ET-1 and vasodilators such as NO is the cause of vasospasm in glaucoma.59,60 It was reported that patients with glaucoma who have vasospasm have a higher susceptibility to glaucomatous damage, which could be a consequence of a decreased dilation of blood vessels that properly autoregulate blood flow. 55 If our speculation is correct, BCACs induce normalization of ET-1, and its receptor balance may be beneficial for ocular blood circulation, since an increased ET-1 reactivity could lead to decreased ocular blood flow as indicated above.
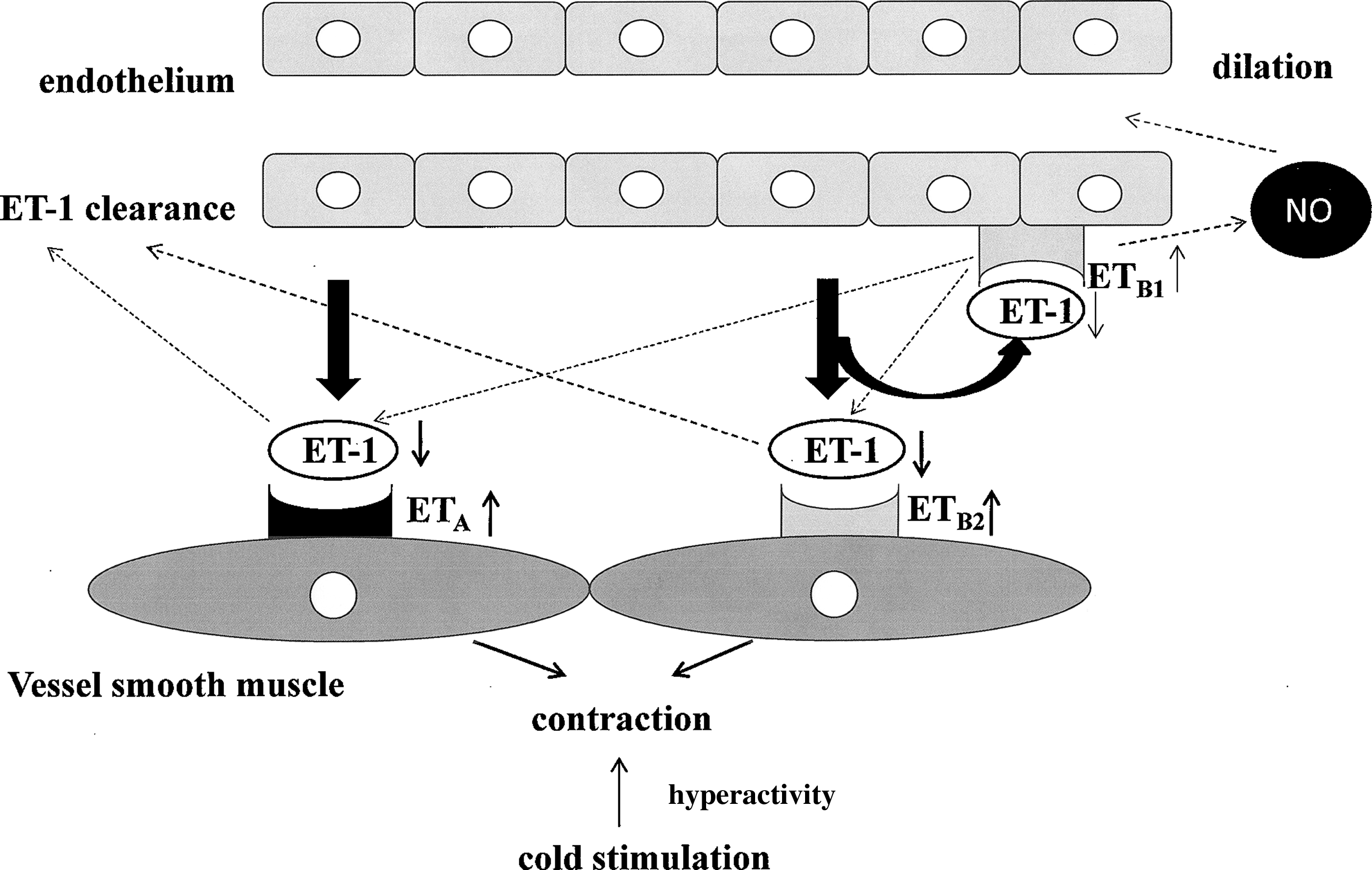
Possible mechanism of hyperactivity of ET-1-dependent vasospastic response found in patients with glaucoma. ET-1 produced by the vascular endothelial cells reacts with its receptors, ETA and ETB1,2. ETA and ETB2 are mainly present on the vascular smooth cells and are responsible for the vasoconstriction. ETB1 is mainly present on the vascular endothelium and causes NO-dependent vasodilation. ET-1 receptors may be upregulated in response to the continued lower levels of serum ET-1 levels. In this situation, a transient increase of serum ET-1 concentrations by cold stimulation may cause hyperactivity of ET-1-induced vasospastic response. NO, nitric oxide.
The possible mechanism in which supplementation of BCACs increases levels of serum ET-1 concentrations in patients with OAG to match those in normal subjects remains unclear. ETB receptor, which is targeted by BCACs, is known to also contribute to the clearance of ET-1 as well as NO-dependent vasodilatation. 35 Additionally, selective ETB antagonists increase plasma ET-1 concentration. Furthermore, animal models with an ETB gene mutation have increased plasma ET-1. 61 Studies have indicated that both wild-type rats treated with ETB antagonists 62 and heterozygous ETB knockout (KO) mice 63 impaired ET-1 clearance, whereas wild-type rats treated with ETA antagonists and heterozygous ETA KO mice have normal ET-1 clearance. Moreover, previous studies suggest that this ET-1 clearance occurs mainly in the lungs and to a lesser extent in the liver and kidneys.64,65 Since the ETB receptor is responsible for the clearance of ET-1, we can speculate that upon systemic administration of BCACs, this could continuously stimulate ETB receptor resulting in a decrease of the clearance of ET-1 within blood circulation, and in turn, this may induce ET-1 secretion by a feedback mechanism (Fig. 3).
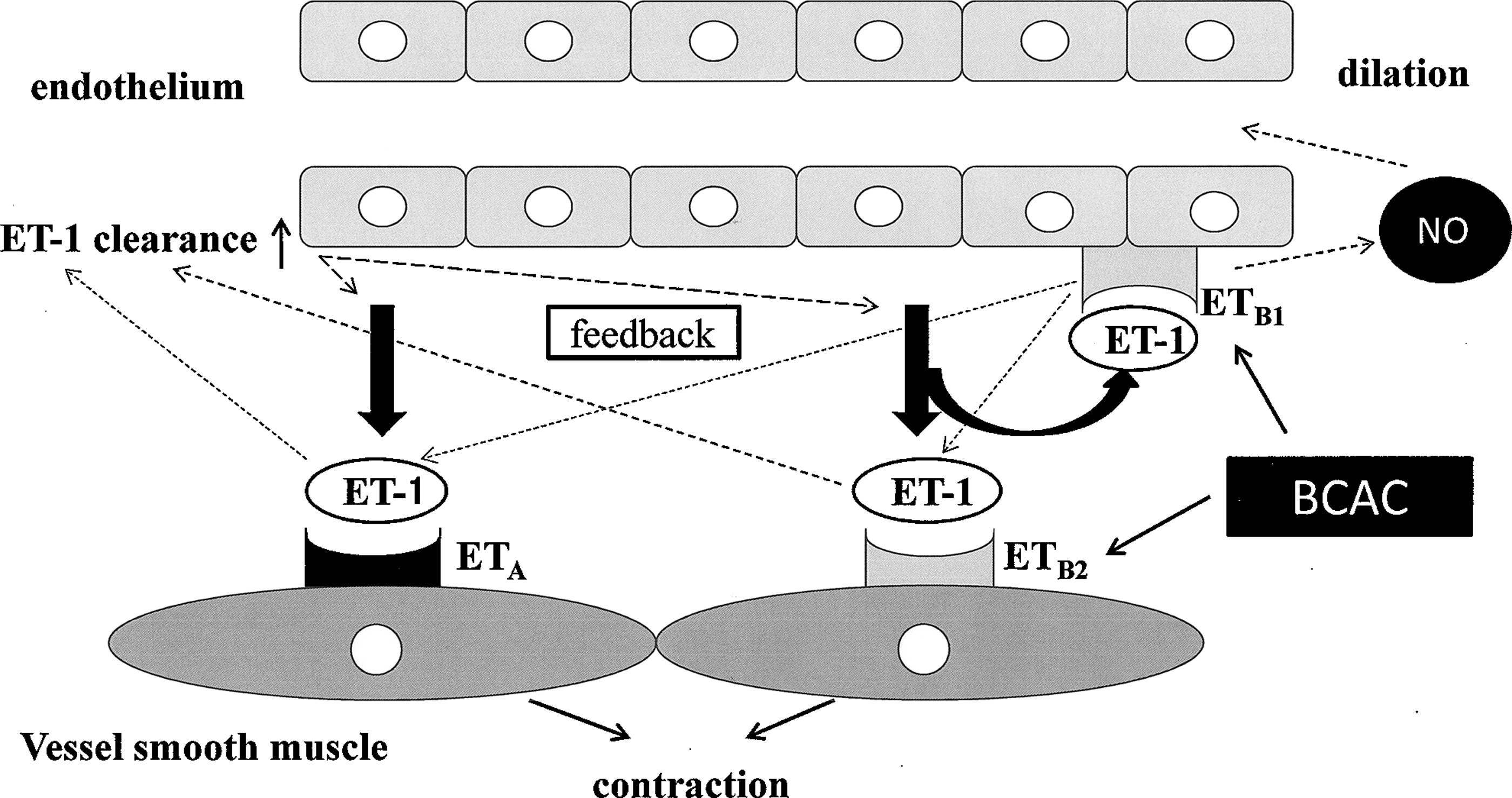
The possible mechanism in which supplementation of BCACs increases levels of serum ET-1 concentrations in patients with open-angle glaucoma to match those in normal subjects. ETB receptor, which is targeted by BCACs, contributes to the clearance of ET-1 as well as NO-dependent vasodilatation. Continuous administration of BCACs could cause a decrease of the clearance of ET-1 within blood circulation by stimulation of the ETB receptors, and, in turn, this may induce ET-1 secretion by feedback mechanism.
Based upon our previous and current findings, we conclude that systemic administration of BCACs to patients with OAG causes normalization of their serum levels of ET-1 concentration, which is presumably obtained by stimulation of the ETB receptor by BCACs, and this may in turn cause an increase in ocular blood flow and slow down patient's glaucoma progression. Quite recently, Shim et al. described that the Ginkgo biloba extract and bilberry ACs also improved visual functions in patients with normal-tension glaucoma. 66 Thus taken together, oral administration of BCACs may be a safe and promising supplement for suppression of the visual field deterioration in subjects with OAG in addition to their role in IOP control.
Footnotes
Acknowledgments
This project has been funded in part by a Grant-in Aid for Scientific Research (C) (22591945) from The Japanese Ministry of Education, Culture, Sports, Science and Technology (H.O.). This trial was registered at clinicaltrails.gov as UMIN000004961.
Author Disclosure Statement
No competing financial interests exist.