
Abstract
Abstract
Purpose:
To review the existing evidence that supports the subconjunctival use of triamcinolone acetonide (TA) in the treatment of various ophthalmic diseases.
Methods:
A literature search was performed for published articles about the pharmacokinetic (PK) and pharmacodynamic characteristics of triamcinolone, as well as its potential ophthalmic use, focused mainly in the subconjunctival mode of delivery. Search terms included corticosteroids, triamcinolone, ocular, subconjunctival, and ophthalmic.
Results:
Corticosteroids represent the mainstay of treatment of ocular inflammation, exerting their action by affecting multiple pathways of the inflammatory response, making them particularly effective in the majority of cases. However, due to the number and severity of the side effects associated with their use, they have to be given with caution. Corticosteroids can be given topically, subconjunctivally, intraocularly, and systemically to treat a variety of ocular diseases with specific pharmacological and PK characteristics. Triamcinolone is one of the most widely used corticosteroids in the treatment of ocular inflammation. This glucocorticoid used subconjunctivally was proven to be particularly safe and effective in some common and important inflammatory ophthalmic diseases such as anterior scleritis, uveitis, and corneal graft rejection. Further, there are other indications for its successful use where data exist, but somehow less abundant.
Conclusions:
This article highlights the potential of TA to complement the treatment armamentarium of anterior segment inflammation.
Introduction
The purpose of this article was to review the use of subconjunctival triamcinolone acetonide (SCTA). Subconjunctival use of corticosteroids, including SCTA, is not a novel therapeutic approach. However, like all subconjunctival modes of drug delivery, its application has been in decline since the advent of newer, fortified corticosteroids, formulated to penetrate the eye better. These were considered to be safer and more effective, and their administration was much less invasive and traumatic for the patient, although they often required high level of compliance.
We performed an extensive literature search in Medline using the keywords ocular, subconjunctival, triamcinolone, ophthalmic, and corticosteroids.
Properties of Triamcinolone Acetonide
Triamcinolone in its 2 commercially available forms, acetonide and diacetate, is a moderate-strength corticosteroid with a relatively long duration of action that can last a minimum of 6 weeks when injected locally (Table 1).11–13 Triamcinolone acetonide (TA) is the most widely used form of the drug. TA for ophthalmic use is administered as an injectable suspension either periocularly or intraocularly as an off-label medication. 2 The most widely used preparation is Kenalog (TA, aqueous suspension 40 mg/mL; Bristol-Myers Squibb), which contains benzyl alcohol as a preservative and has been found to be less toxic for the eye in both humans and animals than the vehicles of other frequently injectable corticosteroids. 2 TA exists in a crystalloid form, the size of the particles ranging from 1 to more than 20 μm, with the majority of them being in the range of 1–5 μm. 14
Goodman & Gilman's. The Pharmacological Basis of Therapeutics. McGraw-Hill; 2001. The material is reproduced with permission of the McGraw-Hill companies.
Apart from its subconjunctival administration, TA is also used in the management of various ocular diseases intravitreally (IVTA) and as a posterior sub-Tenon's or orbital floor injection.2,15–18,19 Anterior-segment surgeons are also using TA to visualize and remove the vitreous from the anterior chamber in cataract surgery complicated with posterior capsule rupture.20,21 Recently, intracameral corticosteroids, including TA, have been successfully used in the treatment of endothelial immune reactions after penetrating keratoplasties (PKPs).22,23
TA and its vehicle showed no retinal24,25 or corneal endothelial toxicity 26 after intravitreal injection and additionally decreased inflammation after surgery. 15 However, one investigation showed that IVTA doses of 4 mg or higher caused prominent retinal damage, with these contrasting findings suggesting that other factors may contribute to intravitreal retinal toxicity of TA, such as preservatives. 27 Finally, sterile, noninfectious endophthalmitis occurring after IVTA is most likely an inflammatory reaction to TA or its vehicle rather than a result of ocular toxicity, with a good visual recovery after treatment. 28
Recently, new formulations of TA were approved by the FDA in the United States under the commercial names Trivaris (TA injectable suspension 80 mg/mL; Allergan) and Triesence (TA injectable suspension 40 mg/mL; Alcon). Both were approved for intraocular use; they are available in single-use preparations and have the major advantage of a preservative-free formulation. In addition, Triesence is terminally sterilized. Thus, the risk of toxicity and sterile or infectious endophthalmitis is potentially reduced to a great extent.
In ophthalmic practice, TA is used in its injectable form with doses ranging from 4 to 20 mg. The variable amount used may result in a difference in pharmacokinetics; higher doses may have the potential benefit of a longer duration of action. 29
SCTA in Ophthalmic Disease
Indications
SCTA has been used with success for anterior scleritis30–32 and recalcitrant vernal keratoconjunctivitis, 33 and prevent pterygium recurrence after surgery, 34 superior limbic keratoconjunctivitis, 35 uveitis, corneal burns and ulcers, herpetic keratitis, and episcleritis, 4 intraocular surgery,4,36,37 as well as in upper eyelid retraction related to active thyroid eye disease.38,39 SCTA is mainly used in recurrent and refractory cases, resistant to other medication and when there are contraindications for conventional treatment. A summary of the indications for SCTA is given in Table 2 in order of its relative effectiveness, as this is elicited by the number of studies referring to its successful use. Clinicians should always seek and obtain informed consent by all patients undergoing SCTA.
In anterior scleritis, usually, patients who had experienced failure of systemic anti-inflammatory medicines were recruited. However, because SCTA was found to be very effective and safe, many patients were given SCTA after they had failed local immunomodulatory therapy only (topical or subconjunctival corticosteroids). 30
Recently, SCTA in conjunction with intensive topical corticosteroid treatment has been reported to successfully reverse corneal endothelial graft rejection after posterior lamellar corneal transplantation 40 and PKPs.41,42 Corneal graft rejection is a complex immune process in which the immune-privileged status of the eye is lost by inflammation and neovascularization mediated mainly by cytokines, growth factors, T-lymphocytes, and antigen-presenting cells. 7 These elements of the inflammatory cascade are the main target of the anti-inflammatory effect of corticosteroids, as mentioned earlier in the text. Short-acting subconjunctival steroids such as betamethasone, for the treatment of corneal transplant rejection, appear to have a limited role, and their use is in decline. 43 We suggest that if subconjunctival TA is used for corneal graft rejection, it should be placed as close to the limbus—and thus rejection site and the antigen-presenting cells—as possible in accordance with the suggestions of previous authors regarding optimal positioning of subconjunctival injections. 44
SCTA has also been successfully used to reverse neovascularization in rabbits. 45 As new vessels can mature over 2–3 weeks, 46 subconjunctival TA should be considered early in the management of corneal new vessel formation, which is resistant to topical steroids.
Pharmacokinetics
A number of reports suggest that subconjunctival steroids achieve intraocular penetration mainly through the temporary incision leakage into the tear film and then through the cornea into the eye. However, due to the lipophilic barrier of the corneal epithelial layer, water-soluble formulations such as phosphate hydrophilic derivatives do not penetrate the cornea easily.1,11,47,48 There is also a local scleral and vessel absorption,11,41,47–49 which probably becomes more important once the incision has healed. Once in the eye, a fourth route of drug diffusion has been postulated: from aqueous into the vitreous. 48 The local fibrolytic effects of SCTA, restricted adjacent to the drug, may play an important role to the scleral absorption by enhancing diffusion of the drug. 50
The penetration of TA after sub-Tenon's injection 5–6 mm from the limbus has been studied in rabbits. It was demonstrated that there are saturable ocular barriers to the trans-scleral delivery of TA into the vitreous with the lymphatics/blood vessels of the conjunctiva being presumably the most important of them. Increasing the amount of the drug injected produced higher levels intraocularly, which was attributed to saturation of these barriers. Other barriers postulated in this study were the sclera, choroid, and retina. 49
The concentration, vehicle, and formulation of a drug may play a much more important role in the degree of intraocular penetration and overall therapeutic effect than its actual pharmacological strength. TA is a long-acting minimally soluble corticosteroid, and its absorption rate may considerably differ from that of short-acting water-soluble corticosteroids.47,51 In other nonocular models, it has been shown that corticosteroids with lower solubility such as TA are absorbed slower, thus maintaining the drug levels for a longer time and creating lower systemic corticoid levels.52,53
One major advantage of subconjunctival/sub-Tenon's injection of corticosteroids, either posteriorly or anteriorly, is the delivery of the maximum amount of drug into the eye—whether this is the aqueous, vitreous, or subretinal fluid—than the rest of the body when compared with other periocular modes of delivery or oral medication. Systemic absorption after a subconjunctival injection is nearly equal to that after a peribulbar injection or oral administration. 54 However, a smaller dose is needed to obtain equal intraocular concentrations when the drug is injected subconjunctivally compared with peribulbar or oral delivery, and thus the absolute systemic corticosteroid concentration is lower with a reduced risk of systemic adverse events and a more target-specific drug application. 48 In clinical practice though, this is probably most relevant for children due to their significantly less body mass. 11 Even IVTA is associated with systemic absorption, but this is not considered pharmacologically significant. 2 In addition, TA is a moderately potent corticosteroid that minimizes its systemic effects. Generally, it is preferable to reserve the systemic corticosteroid therapeutic option for severe, bilateral intraocular inflammation or when an associated systemic inflammatory condition coexists.1,47,48,55,56
A study carried out in humans has demonstrated significant intraocular penetration of short-acting water-soluble corticosteroids (dexamethasone disodium phosphate) after subconjunctival injection of 0.5 mL of 5 mg/mL solution, much higher than that achieved with peribulbar injection or oral administration. Up to 858 ng/mL of dexamethasone was measured in the aqueous humor in this study. 48 This is much higher than the 670 ng/mL of prednisolone acetate and the 31 ng/mL of dexamethasone alcohol recorded in the human aqueous humor after topical administration of 1 drop only.1,47 In addition, another study showed that repeated topical application of dexamethasone disodium phosphate 0.1% results in a maximum aqueous humor and vitreous concentration of only 30.5 and 1.1 ng/mL, respectively. 54 One other study showed increased intraocular penetration of prednisolone acetate (Econopred plus; Alcon) with a peak aqueous humor level of 1,130 ng/mL 30–45 min after instillation. 1 The above discrepancies could be attributed to the different formulations used in each study, as it has been proven that lipophilic derivatives penetrate the normal cornea more than hydrophilic ones. Also, higher concentrations of any corticosteroid, regardless its relative potency, achieve higher intraocular concentrations. 47 The timing of the tissue sample retrieval after instillation could also affect the final drug concentration. A major shortcoming is that the intraocular concentration of short-acting corticosteroids injected periocularly, as well as after topical administration, rapidly declines within a 24-h period unless repeated in frequent intervals.1,48
Although subconjunctival or anterior sub-Tenon's TA injections produce a significant anterior segment steroid concentration that remains detectable in the aqueous humor for months, the peak vitreous levels are substantially less. This discrepancy could be attributed to the lack of postequatorial diffusion of drug following these modes of administration.47,49 A study in rabbits showed that periocular injections anterior to the equator (subconjunctival and subtenons) results in the drug tending to remaining anterior to the equator, concluding that such an approach is more useful in anterior ocular disease and far superior to systemic drug administration. 57
Studies reviewing the histological and biochemical characteristics of subconjunctivally injected corticosteroids and TA are scarce. According to one literature review, the therapeutic and diagnostic excision of the drug revealed the eosinophilic material present in the subepithelial connective tissue that was granular in the case of TA (after 3 weeks) or foamy and homogeneous in the case of methylprednisolone acetate (after 7 weeks). 58 Quantification of the TA subconjunctival depots revealed interestingly enough that TA depots could be present for as long as 13 months after the injection. 59 This is in accordance with 2 other reports with the TA being present for as long as 7 months 51 and 10 months, 60 as well as our own anecdotal experience with SCTA depots being present for more than 12 months in some cases. Kalina's study revealed that the percentage of the originally injected triamcinolone in the excised sample ranged from 4.2% to 44%, with a mean of 20%, and the disappearance rates from depot triamcinolone did not correlate with the time from injection to surgical excision. 59 In other published reports, the amount of residual surgically excised triamcinolone was 5.9% after 4.5 months 61 and 19% after 6.5 months. 60
Delivery and Mode of Action of TA
The authors believe that SCTA acts by locally suppressing the immune response over a period of time, due to the crystalline nature of the drug. The long-acting and constant presence of local steroid (up to several months) appear to be an important property, as TA is only a moderate-strength glucocorticoid, 4 times the strength of hydrocortisone and 5 times weaker than betamethasone. 11 Recently, antivascular endothelial growth factor (anti-VEGF) agents have been used to reverse corneal neovascularization and graft rejection in humans and animals, but their effect was short-lived and limited.62–64 This is in contrast with the pluripotent corticosteroid agents and specifically the long-acting TA (Fig. 1).8,11
Properties of triamcinolone acetonide (TA).
It is a well-accepted notion that subconjunctival delivery is a safer way to administer drugs periocularly compared with retrobulbar and peribulbar injections, because the needle tip is visible throughout the procedure, thus minimizing the risks, such as retrobulbar hemorrhage or perforation of the eye. 48
The technique we recommend for the most efficient use of SCTA is to cause precipitation of the white crystals in the syringe and remove the supernatant before the injection. This can be achieved by positioning a 2-mL or insulin syringe in a vertical position and observe the separation of the crystals from the vehicle as a densely white precipitate with an overlying grayish, turbid fluid. If 1 mL of TA is used, the precipitate will measure ∼0.1–0.15 mL and will account for the larger amount of TA in the solution. Whitening of the subconjunctival area is observed while injecting with a 27-gauge needle, indicating that pure TA is mostly present, and thus a drug depot is created (Fig. 2). In this way, the short-term absorption of leaking TA via the cornea is reduced, and absorption for longer may be achieved. The potentially toxic vehicle and preservative could also be minimized in this way. Sometimes, resistance may be felt while advancing the plunger due to the presence of drug crystals, and thus a smaller gauge needle may facilitate administration. A long needle track could also minimize leakage of the drug from the subconjunctival space. Injection should be placed anteriorly to facilitate potential removal in the future if complications occur. Shaking the vial before use is not affecting the actual dose of TA delivered. 65

Subconjunctival triamcinolone acetonide (SCTA) injection inferotemporally, visible as an opaque area of drug depot (black arrow).
Complications and Side Effects of SCTA
Intraocular pressure
The most significant and most common adverse reaction of SCTA is the development of increased intraocular pressure (IOP) (Table 3). This a well-known complication of the topical ophthalmic use of corticosteroids, especially, in individuals with primary open-angle glaucoma or a family history of glaucoma.48,59–61,66,67 Other well-documented risk factors for steroid-induced IOP rise are increasing age, myopia, and type I diabetes. 68 In general, the higher the steroid potency the greater the ocular hypertensive effect. 69 The systemic use of corticosteroids has also been proven to have a similar effect on the IOP, but not as profound as with other modes of delivery. 70
The time for the discovery of IOP elevation after subconjunctival injection of triamcinolone varies in different studies from 1 week 51 to 10 months. 60 The duration and severity of the steroid-induced IOP response appear to be inversely related to the solubility of the subconjunctival corticosteroid preparation, irrespectively of whether topical corticosteroid treatment, before SCTA injection, caused IOP rise or not. 51
Baseline measurement of IOP is required before the SCTA injection. Thereafter, regular monitoring is necessary in more frequent intervals initially and no longer than 6 months if IOP is not elevated in the first few months. In case of IOP rise, attempts for normalization include both pharmacological and surgical methods. Topical beta-blockers, carbonic anhydrase inhibitors, and alpha-agonists are usual first-line treatments with miotics and prostaglandins being relatively contraindicated or ineffective. 68 The most effective and safe way to manage the elevation of IOP after subconjunctival injection of long-acting corticosteroids is surgical excision of the depot,48,68 and this is our own clinical experience as well (Fig. 3), though this may not be feasible for more posteriorly placed depots. Thus, as mentioned earlier, depots of triamcinolone in case of subconjunctival injection should be placed anteriorly to facilitate potential removal in the future if deemed necessary. Similarly, vitrectomy may help control the IOP in selected cases after intravitreal TA. Trabeculectomy remains an effective surgical treatment in those patients who have a persistently raised IOP after complete/incomplete removal of the SCTA depot and are refractory to medical therapy. However, as always, the adverse consequences of trabeculectomy or other forms of filtration surgery should be considered in relation to the potential benefits and alternative treatments. 68
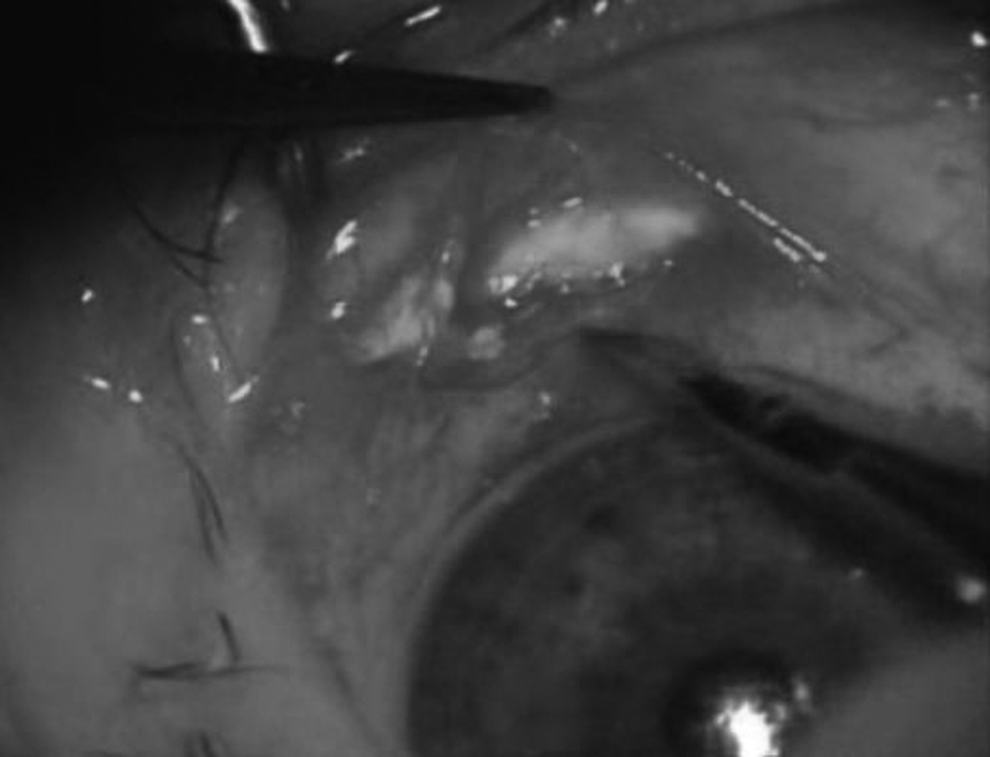
SCTA depot removed surgically.
Cataract and other less-common side effects
Cataract, well documented with other routes of corticosteroid administration,71,72 was linked with only one case of SCTA, 41 although concurrent uveitis was also postulated as a possible cause. 46 Other reported side effects of SCTA are conjunctival ulceration, 73 infectious scleritis, 74 blepharoptosis and mydriasis, 51 and conjunctival ischemia. 75 Potential side effects of SCTA such as delayed wound healing or systemic absorption of TA have not been reported as of yet.
Finally, the SCTA injection should ideally be placed inferiorly if possible, for cosmetic reasons, as the white deposit is covered by the lower eyelid. Subconjunctival hemorrhage is also a well known, but trivial side effect.
Summary
SCTA is a very efficient mode of treatment in ocular anterior segment disease, especially in the management of anterior scleritis, where it has been widely used. Excellent outcomes were also reported in corneal graft rejection and vernal keratoconjunctivitis. Smaller doses are required compared to systemic administration for equivalent or even greater local corticosteroid concentration, and there is also a more target-specific drug application and reduced risk of systemic adverse events. 1 It is also a generally safer mode of administration with higher intraocular penetration, less potential toxicity, and fewer complications compared with peribulbar and infraorbital injections or systemic administration,11,48 particularly beneficial in cases of noncompliance.
We believe that the dosing of TA needs to be adjusted in relation to the severity of inflammation, with higher doses in severe cases, both for optimal control of inflammation and saturation of the ocular barriers from the conjunctiva to the retina. Whether anteriorly placed TA injection will be more effective if placed in the sub-Tenon's area is not clear, and these 2 anatomically distinct spaces are not distinguished in most studies and in clinical practice. 52
Raised IOP appears to be the most important and commonest side effect. It cannot be predicted with certainty which patient will develop steroid-induced high IOP, as topical steroid nonresponsiveness does not preclude IOP rise after SCTA. The fact that topical corticosteroids are given in a pulsed fashion and that repository corticosteroids enter the eye in a continuous pattern may contribute to this undesirable effect. 51 Thus, it is necessary to establish a baseline IOP before initiating therapy and closely monitor the IOP for at least 6 months after periocular TA, especially if risk factors are present. It seems that surgical excision of the subconjunctival depot is an effective way to normalize IOP.
It is important to note that the visibility of triamcinolone correlates with its action.32,60 Although TA is not more potent than dexamethasone or betamethasone, SCTA seems to have a more favorable outcome, but also results in more frequent and severe IOP rise, which could indirectly confirm its effectiveness. The reason is not clear, but it could be attributed to the less-soluble form of TA, slow release of the drug from the formed depot, and the long duration of action.
Some of the substantial studies referred in this review have used short-acting corticosteroids, and some caution is required when extrapolating their results to long-acting drugs such as TA. The difference is that a slower release and more sustained intraocular levels are achieved with long-acting medication, such as TA, and this in turn may mean lower levels into the systemic circulation, as previously shown in nonocular models. 52 In addition, the majority of the studies regarding the intraocular delivery of corticosteroids after diverse modes of administration were done in animals and other nonocular models, for example, joints. Their results can be significantly different from human and ocular data because of the differences in the anatomy and physiology.
The role of SCTA in various ocular diseases and especially in corneal graft rejection and corneal new vessel formation needs to be further investigated. Questions such as optimal dosing and optimal mode of delivery for TA remain to be answered. We believe that SCTA is a safe, efficacious, and cost–effective adjunct or alternative to currently available treatments for the contemporary ophthalmologist.
Footnotes
Author Disclosure Statement
No competing financial interests exist.