
Abstract
Abstract
In the ocular pharmacology market, there is a noteworthy unmet demand for more efficacious delivery of ocular therapeutics. Contact lenses are emerging as an alternative ophthalmic drug delivery system to resolve the drawbacks of the conventional topical application methods. Thus, contact lenses drug delivery systems have been developed to provide an increased residence time of the drug at the surface of the eye leading to enhanced bioavailability and more convenient and efficacious therapy. Several research groups have already explored the feasibility and potential of contact lenses loading conventional drugs used to treat anterior eye disorders. Drug incorporation to the lens body is achieved with techniques, like simple soaking, inclusion of drug-loaded colloidal nanoparticles, or molecular imprinting. Regardless of the technique used, key properties of the contact lens, such as transparency and oxygen permeability, should be preserved. In this article, we reviewed the different techniques used for drug delivery through contact lenses, analyzing their advantages and disadvantages, and focused on articles describing contact lens-based ophthalmic drug delivery systems with significant potential to use in ocular therapeutics.
Introduction
To overcome the low ocular bioavailability, frequent application of doses of drugs at high concentrations is used to achieve the desired therapeutic effects. This discontinuous dosing not only results in extreme fluctuations in ocular drug levels but, also, a significant portion of the applied solution can be absorbed in the conjunctiva or collect in the nasolacrimal system, which drains into the nasal cavity and leads to absorption in the bloodstream. The presence of certain drugs in the bloodstream can induce undesirable systemic side effects. For example, fluoroquinolones can produce not only corneal, but also systemic toxicity (e.g., hepatotoxicity, nephrotoxicity, and neurotoxicity).3–5 Glaucoma treatments, in particular, β-adrenergic receptor blockers, such as timolol, can also generate deleterious effects in the heart. 6
Additionally, the real dose effectively administered can vary by the application technique, the type of eye drop carrier, and the compliance of the patient.7,8 Thus, a significant variation in the concentration of drug present in the eye can occur during eye drop treatment. The eye can be exposed to a series of potentially toxic peak concentrations followed by inadequate concentrations until the next dose that could lead to ocular and systemic side effects, and serious complications depending on the therapeutic window and the underlying pathophysiology.
The problems associated with topical ocular administration of drugs by eye drops have prompted the research of alternative approaches for ophthalmic drug delivery, such as mucoadhesives and viscous polymer vehicles, nanoparticles, in situ gel-forming systems, iontophoresis, or punctal plug.9–12 An ideal ocular drug delivery system should be able to increase the residence time of the drug in the eye, and to avoid large fluctuations in the ocular drug concentration as well as possible systemic side effects. In this context, soft contact lenses (SCLs) are gaining an increasing attention as new vehicle for ophthalmic drug delivery. In the eye, contact lenses are separated from the cornea by a thin fluid layer called postlens tear film. The fluid in the postlens tear film is not well-mixed with the remaining tear fluid. The mixing time of the fluid in the postlens tear film with the outer tear fluid is about 30 min. 13 Thus, ophthalmic drugs released from the SCLs will have a residence time in front of the cornea for at least 30 min compared to 2 min for eye drops. 14 The enhanced residence time may lead to an increase in drug bioavailability to possibly as large as 50% compared to 1%–5% by eye drops. 15 This increased corneal bioavailability also implies the decrease of the amount of drug that enters in the systemic circulation, thus potentially reducing side effects. Accordingly, SCLs are an attractive system for ophthalmic drug delivery and several approaches are being currently investigated to enhance drug loading capability and to control the release rate of drugs from the contact lens. In this review, we describe different strategies used in the design and development of contact lens for drug delivery (Fig. 1) and the therapeutic applicability of these devices in the treatment of various ocular disorders.
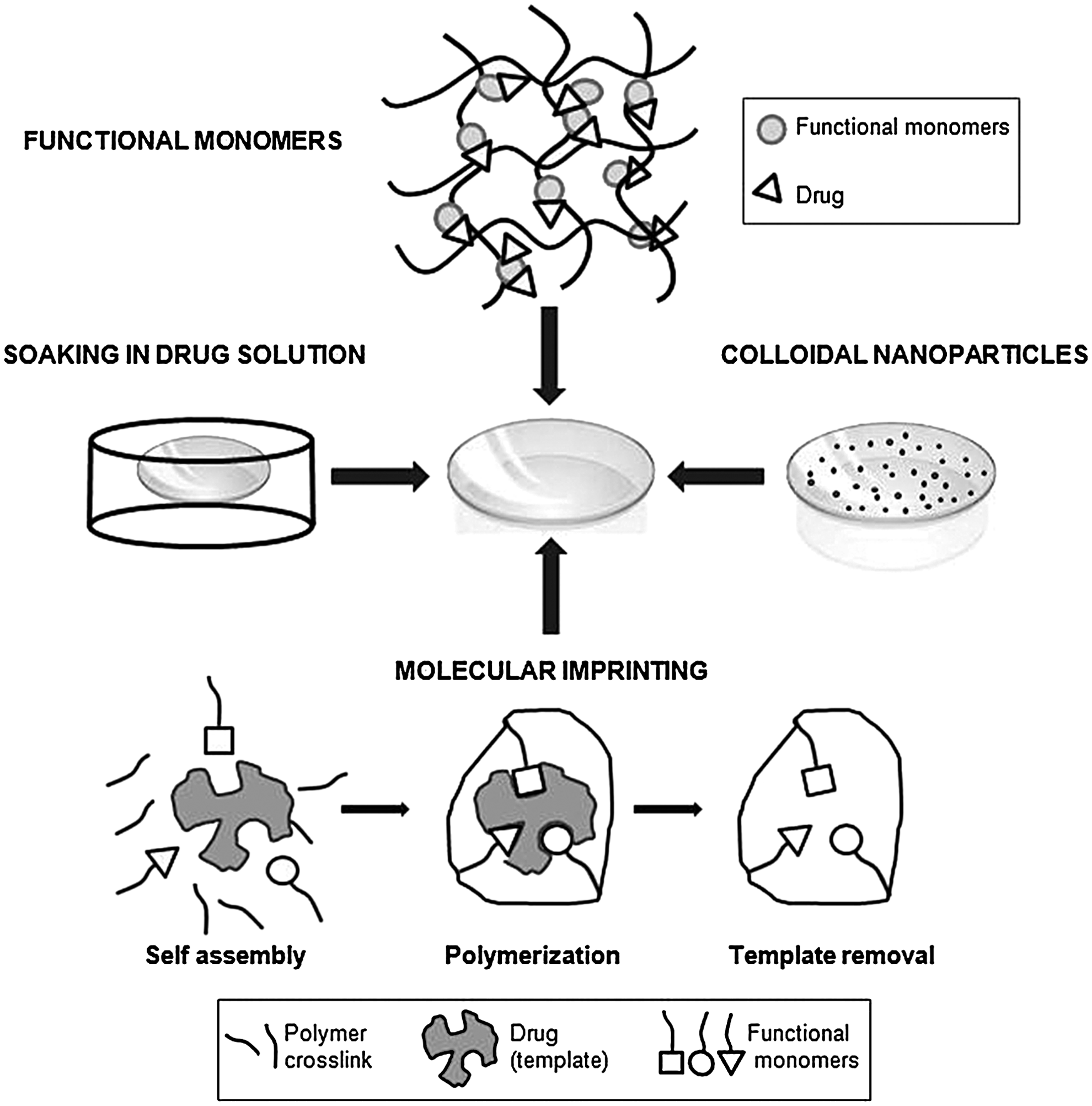
Schematic representation of different techniques used for drug delivery through contact lenses: soaking of lenses in drug solution, copolymerization of the contact lenses hydrogels with functionalized monomers, incorporation of drug-loaded colloidal nanoparticles, and molecular imprinting.
Strategies Used to Generate Contact Lens-Based Drug Delivery Systems
Soaking of lenses in drug solution
The simplest way to incorporate a drug into SCLs is to soak preformed lenses in the drug solution. The delivery of very diverse drugs, such as pilocarpine, 16 antibiotics, 17 timolol, 18 dexamethasone 19 from SCLs made from poly (2-hydroxyethyl methacrylate) (pHEMA) hydrogels (with a high water content that facilitates the diffusion of solutes) has been investigated mainly in in vitro assays. In these experiments, after soaking SCLs in drug solutions, the dynamic drug release was monitored. SCLs based on commercially available silicon-containing hydrogels or polyvinyl alcohol hydrogel have also been examined for delivery of ophthalmic drugs.20–23
Although in the majority of the cases, a higher bioavailability of the drug delivered via contact lenses was observed compared with eye drops (e.g., combination of in vitro experiments with modeling of the in vivo behavior showed that at least 20% of the drug timolol that was entrapped in a pHEMA contact lens entered the cornea, which is larger than the fractional uptake recorded using eye drops 18 ), the soaking method present some important limitations. First, the drug uptake in SCLs depends on several factors (the water content and thickness of the lens, the molecular weight of the drug, the solubility of the drugs in the gel matrix…) that can limit the loading capacity in some cases, resulting in low drug loading.
To improve drug loading, Nakada and Sugiyama developed a contact lens with a hollow cavity by bonding together 2 separate pieces of lens material. 24 This compounded lens has more drug loading capacity; however, oxygen and carbon dioxide permeabilities of the compounded lens are smaller compared with regular SCLs, due to the presence of 2 separates sheets of lens material, which may induce corneal edema.
A second limitation of the soaking method is that the release of the drug from soaked contact lenses tends to occur very quickly with the entire drug diffusing in a few hours. For example, the corticosteroid prednisolone, the glaucoma drug pilocarpine, and the antibiotic ciprofloxacin were released from hydrophilic contact lenses within 1 to 3 h.16,25,26 In vitro experiments have shown complete release of ketotifen fumarate from drug-soaked alphafilcon A (pHEMA) lenses in ∼5 h. 20 Similarly, the release of ketotifen fumarate from silicone hydrogel contact lenses was no longer than 4 h. 21 A significant release of ketotifen fumarate was detected initially at 10–15 min, and then reaching release plateaus from 1 to 4 h.
Thus, slow and extended drug release is not properly accomplished for soaked contact lenses.
To increase drug release durations, Kim et al., developed new silicone hydrogel materials that showed extended release of timolol and dexamethasone for times ranging from 2 weeks to 3 months from 100-μm-thick gels. 27 Nevertheless, these new materials have not been currently used for contact lenses production, so extensive in vitro and in vivo testing would be necessary to demonstrate the applicability of these materials in contact lenses production. An alternative approach has been developed to extend the release duration from silicone hydrogel contact lenses.28–30 In this approach, vitamin E aggregates are incorporated within contact lenses to create barriers to drug diffusion, resulting in increased releases times from drugs that are loaded into the lenses from hours to several days. These vitamin E-loaded lenses maintain proper oxygen permeability, ion permeability, and light refractive properties to be used as extended wear contact lenses.
Copolymerization of the contact lens hydrogels with functional monomers
Another method to make ophthalmic drugs deliverable by SCLs involves the incorporation of monomers able to interact with the target drug into the hydrogels. The monomers act as drug binding points for protonizable or hydrophobic molecules, and communicate functionality to the hydrogels. Cationic monomers, such as methacrylamide propyltrimethylammonium chloride have been used to enhance the loading capacity and to extend the release of anionic drugs based on an ion-exchange reaction. 31 In physiological conditions, the tear fluid ions compete with the drug for the ionic groups of the hydrogel and the drug is released. Similarly, Sato and coworkers, used the anionic monomer 2-methacryloxyethyl phosphate to incorporate the cationic drug naphazoline into pHEMA SCLs. 32 Acrylic acid has also been shown as an useful monomer to increase hydrogel affinity for insulin, oxprenolol, or timolol. 33
On the other hand, the simultaneous use of several monomers has also been reported. Thus, the combination of the hydrophobic monomer 3-(trimethoxy-silyl)propyl methacrylate and the ionic monomer N,N′-dimethylaminoethyl methacrylate, improved the loading of insulin and protamine and their extended release from pHEMA SCLs. 34 Other monomers incorporated to improve the efficacy of pHEMA SCLs in drug delivery are 4-vinyl-pyridine (VP) and N-(3-aminopropyl) methacrylamide (APMA). 35 These incorporated monomers increased the amount of nonsteroidal anti-inflammatory drugs ibuprofen (up to 10-fold) and diclofenac (up to 20-fold) that were loaded on the lens. Remarkably, physical properties of the pHEMA hydrogels, such as viscoelastic properties, the glass transition temperature, and water uptake behavior, remain unaltered after the incorporation of monomers. Dried loaded pHEMA–APMA and pHEMA–VP hydrogels quickly swelled in water; but ionic/hydrophobic interactions limited the drugs released to be below 10%. Once the water-swollen hydrogels were transferred to pH 5.8 or 8.0 phosphate buffers or NaCl solutions, the release was prompted by competition with ions in the media. Under these conditions, extended release was achieved due to remaining of hydrophobic interactions and the high polymeric density of the pHEMA hydrogels (sustained release process happened for 24 h for ibuprofen and almost 1 week for diclofenac).
Dispersion or immobilization on the contact lens surface of drug-loaded colloidal nanoparticles
This method is based on incorporation of drug-loaded colloidal particles (nanoparticles, liposomes, microemulsions, etc.) into the matrix of contact lenses.36,37 Drug-loaded colloidal particles entrap a large amount of drug, and then are dispersed in the lens material during polymerization. Nanocapsules prevent the interaction of drug molecules with the polymerization mixture and also provide additional resistance to drug release. The drug must first diffuse through the nanoparticles and penetrate the particle surface to reach the hydrogel matrix. Thus, it is expected that colloidal particle-loaded contact lenses can deliver drugs at a slow rate for a long period of time. Following this technique, lidocaine-loaded dimyristoyl phosphatidylcholine liposomes were dispersed in pHEMA contact lenses. 38 Lidocaine was released for 7 days with 2 separate time scales; there was an initial burst that released about 15%–30% of the drug in the first few hours, and then there was a much slower release over a time scale of days. The presence of the dispersed liposomes reduced the transparency of the contact lenses (80% of transmittance as compared to 90% for the pure pHEMA contact lenses).
Nanoparticle/liposomes-loaded lenses requires 2 steps for fabrication: preparation of the particles, followed by entrapment in the lens matrix. Alternatively, nanoparticles and/or nanodomains can be generated in situ in 1 step by addition of surfactants to the polymerizing mixture. The surfactants can interact with the polymer matrix and form micellar aggregates creating hydrophobic sites inside the gel system, where a hydrophobic substance will preferentially partition. Kapoor and coworkers applied this strategy to develop Brij surfactant-laden pHEMA hydrogel contact lenses.39,40 Results indicated that this contact lens-based delivery system can deliver the drug cyclosporine A at a therapeutic dosage for a period of about 20 days and possesses suitable mechanical and optical properties for contact lens application. In this contact lens system, a Brij surfactant could be also released, indeed an average release of about 30 μg/day was demonstrated. According to previous toxicological studies with Brij surfactants,41,42 this concentration would have negligible toxicity, as even at high concentrations (20 mg/mL), Brij surfactants did not cause toxic effects on the ocular surface.
Apart from being dispersed, drug-loaded nanocarriers (nanoparticles or liposomes) can be immobilized on the surface of contact lenses that are previously functionalized. To immobilize levofloxacin liposomes on commercial contact lens (Hioxifilcon B), polyethylenimine was covalently bounded onto the hydroxyl groups present on surface contact lens, followed by NHS-PEG-biotin molecules being attached onto the surface amine groups by carbodiimide chemistry. NeutrAvidin was then bonded onto the polyethylene glycol (PEG)-biotin layer, and liposomes containing PEG-biotinylated lipids were docked onto the surface-immobilized NeutrAvidin. Subsequent addition of further NeutrAvidin and liposome layers enabled multilayers to be formed. 43 No significant changes in cell growth or viability were found in cytotoxic assays, indicating the biocompatibility of the tested liposome-laden contact lenses. 44 In contact lenses bearing 2 layers of liposomes, levofloxacin release was completed in 30 h, while liposomes of 5 or 10 layers maintained a sustained delivery of levofloxacin until 120 h. 45 However, this multilayer scheme of liposomes may be inconvenient, since oxygen and carbon dioxide permeabilities were decreased.
Molecular imprinting
Molecular imprinting allows the creation of macromolecular memory for a template molecule embedded within a flexible macromolecular network. 46
In this technique, the components of the hydrogel network are organized in such a way that high-affinity binding sites for the drug are created. Drug is added before polymerization, and the monomers should arrange as a function of their ability to interact with the drug molecules. After polymerization, the drug molecules that have acted as templates are removed, and the polymer network may exhibit tailored-active sites or imprinted pockets with the size and the most appropriate chemical groups to interact again with the drug. Imprinted network formation can tune the drug loading and release profile with a proper optimization of drug affinity relating to the number and strength of interactions between the drug and polymer. The use of imprinted hydrogels as SCLs was first explored by Alvarez-Lorenzo and coworkers. Imprinted hydrogels composed of HEMA, and small amounts of methacrylic acid had higher loading of timolol (12 mg timolol/g dry hydrogel) than nonimprinted gels, with the drug being released in the next 8–10 h. 47 Later studies revealed that it is possible to prolong the drug release modifying monomer to template (M/T) ratio. The increase of the monomer/template rate resulted in a slower in vitro release with 50% of timolol being released in 3 days. 48 Similarly, imprinted hydrogels prepared with a high M/T ratio showed a great ability to control the release of the antibiotic norfloxacin, sustaining the process for 2–5 days. 49 Likewise, the release rate of sodium diclofenac from imprinted contact lenses was significantly reduced by increasing the M/T ratio from 1 to 10.5. 50 Collectively, these results reflect that the functional M/T ratio is a critical variable in the optimization of imprinted contact lenses design.
Improvement in drug loading and extended release can be also reached when multiple functional monomers are included instead of single monomers.51,52 Thus, ketotifen fumarate loading was 6-fold greater in the highest functionalized imprinted hydrogels and their diffusion coefficients were 10 times lower than in less functionalized hydrogels.51,53
Miscellaneous
An alternative methodological strategy to load the drug into contact lenses is the supercritical solvent impregnation/deposition method, which is characterized by dissolving the drug into compressed high-volatile fluids, such as carbon dioxide (at subcritical or supercritical conditions), and then contact the resulting mixture with the polymeric matrixes to be loaded. Using this approach, acetazolamide has been successfully loaded in commercial contact lenses (Balafilcon A). 54 The amount of drug loaded and the final drug released can be controlled by adjusting the employed operational conditions (pressure, temperature, processing time, and depressurization rate) and without change thermomechanical, surface/wettability, and optical properties of the commercial contact lenses. For example, faster depressurization rates may favor drug depth impregnation rather than surface/near-surface impregnation, thus diminishing initial burst release and promoting a more prolonged and sustained drug release.
On the other hand, SCLs functionalized with pendant cyclodextrins for controlled drug delivery have been generated. 55 This technique consists of synthesizing first the hydrogel, and then attaching the β-cyclodextrin molecules through a few of their hydroxyl groups. Thus, the β-cyclodextrins neither participate nor interfere in the network formation, and consequently not significantly alter its structural properties. The pendant β-cyclodextrins markedly improved the ability of the hydrogels to load diclofenac (1,300%) and sustained drug release for up to 2 weeks in lacrimal fluid.
Finally, contact lenses with a drug–polymer film integrated have also been designed and characterized. 56 Steeper contact lenses were created by encapsulating econazole-impregnated poly(lactic-co-glycolic) acid (PLGA) films in pHEMA hydrogels by ultraviolet hotopolymerization. The contact lenses retained the fungicidal effects of econazole over the course of 3 weeks and exhibited both the curvature (8.05-mm base curve) and the diameter (15.5 mm) consistent with measurements of commercially available lenses. 57
Physical Properties of Contact Lens Drug Delivery Systems
Physical properties are a significant consideration in the design and quality control of contact lens for drug delivery. However, there are not many studies analyzing in depth all these properties collectively. In this section, we discussed some of the physical properties (transparency, oxygen permeability, glass transition temperature, wettability, and water content) evaluated for drug eluting contact lenses generated using different technologies and compared with those of commercial lenses.
Transparency of the lens
Optical clarity of the contact lens should be maintained after incorporation of drugs. Novel approaches have enabled to generate contact lens drug delivery systems with acceptable transparency, although it could be improved in some cases. For instance, pHEMA gels loaded with liposomes showed a transmittance of 80% compared with 90% for the pure pHEMA gels. 38 In contrast, surfactant laden SCLs were transparent and clear and 100-μm-thick hydrated gels had transmittance values larger than 98.5% at a wavelength of 600 nm, and so are suitable for contact lens application. 40 Drug eluting contact lenses formulated with other techniques, such as supercritical solvent impregnation also exhibited optical clarity and transmittance values greater than 92%, which is an acceptable commercial optical clarity value. 54
In molecular imprinting contact lenses designed for ocular delivery of carbonic anhydrase inhibitors drugs, the inclusion of zinc methacrylate as a monomer generated hydrogels slightly opalescent and lower transmittance; 58 however, molecular imprinting contact lenses, including other monomers,52,59 have shown to maintain transmittance values comparable to those of conventional lenses.
Oxygen permeability
Drug eluting contact lens should allow transfer of oxygen to the eyes since low oxygen permeability can cause severe side effects, such as corneal edema. To avoid hypoxia, a minimum value of oxygen transmissibility (Dk/t) around 125 has been suggested. 60 Oxygen permeability in contact lens is generated using some approaches, like contact lenses characterized by a hollow cavity binding 2 lenses 24 or contact lenses containing multilayer scheme of liposomes. 45
The silicone hydrogel contact lenses show excellent oxygen permeability. The reported values of oxygen permeability (Dk) of various silicone hydrogel contact lenses are 140 for NIGHT&DAY™, 110 for O2OPTIX™, and 103 for ACUVUE® OASYS™. Different drugs have been soaked in these contact lenses together with vitamin E to prolong drug release time. No significant changes in Dk values were observed with 35% of vitamin E loading, indicating that oxygen permeability was not substantially modified. 30 Moreover, recently, molecularly imprinted silicone hydrogel contact lenses for drug delivery have been generated; 61 however, data about oxygen permeability of the lenses were not provided.
Glass transition temperature
Thermomechanical characteristics are important commercial contact lens properties, since they will control some of their functional features as ophthalmic devices, including comfort. Glass transition temperature has been measured in drug eluting contact lenses manufactured by various approaches. Analysis by differential scanning calorimetry did not show significant differences in glass transition temperature when monomers were incorporated in pHEMA SCLs as compared to pure pHEMA SCLs. 35 Glass transition temperature was neither affected after supercritical solvent impregnation process 54 or in SCLs functionalized with pendant cyclodextrins for controlled drug delivery. 55
Wettability
Wettability of contact lenses is a critical variable that affects their physiological compatibility and the stability of the prelens lacrimal fluid. It can be determined by contact angle measurements. Wettability of pHEMA contact lenses was slightly increased when copolymerized with high proportions of glycidyl methacrylate, but slightly decreased when cyclodextrins were attached. 55 Likewise, contact angle values of surfactant-laden pHEMA SCLs were lower than those for control pHEMA SCLs. 40
On the other hand, the supercritical solvent impregnation method did not greatly affect the contact angle measurements when compared to control SCLs. 54
Water content
Water content of contact lenses is crucial as it likely impacts comfort and an increase in the water content enhances the oxygen permeability of pHEMA contact lenses. For pHEMA hydrogels, SCLs containing comonomers (4-VP and APMA) less than 20% of the aqueous phase of the hydrogel consisted of free water, in good agreement with data reported for pure pHEMA hydrogels. 35 Similarly, water content was not altered in molecularly imprinted pHEMA hydrogels contact lenses designed for norfloxacin and ketotifen fumarate release.49,52 In contrast, an increase in water content was detected in surfactant-laden pHEMA SCLs, presumably due to the formation of small pores (less than 40 nm), which are filled with water. 40
Treatment by Contact Lens-Based Drug Delivery Systems of Ocular Disorders
Contact lens wear can present several negative effects. Corneal erosions are a relatively rare complication of contact lens wear, with a higher incidence when lenses are worn in extended wear modality. 62 The use of contact lens can also predispose to microbial keratitis (frequently associated with an inadequate use and maintenance of contact lenses). 63
In addition, contact lens wear is a risk factor for dry eye symptoms being much more prevalent in patients who wear contact lenses (affecting about 50%) than in the nonlens-wearing population. 64 Finally, wearing of contact lens is usually minimized in ocular allergy patients during seasonal flare-ups and its use is contraindicated in specially severe allergic conditions, such as vernal conjunctivitis. 65
All these factors could limit the applicability of contact lenses as drug delivery systems. However, some of these adverse effects induced by contact lens wear could be also mitigated by the incorporation and release of certain drugs into contact lenses. For example, the inclusion and delivery of re-wetting or lubricating agents could ameliorate contact lens-induced dry eye and can make more comfortable contact lens use in allergic patients during periods of maximal allergic response.
Contact lens-based drug delivery system is supposed to be used for ocular surface and anterior chamber treatment, but, also their potential application for treatment of posterior segment diseases has been suggested, 66 although this point still needs further investigation.
In this section, promising results of contact lens-based delivery of representative drugs (until now administrated by means of eye drops) currently prescribed for the treatment of various ocular surface and anterior chamber disorders are summarized (Table 1).
EGF, epidermal growth factor.
Antibiotics for ocular infection
Infection of the eye leads to conjunctivitis, keratitis, endophthalmitis, and other diseases, which are responsible for increased incidence of morbidity and blindness worldwide. Patients who develop a severe ocular infection of the outer surface of the eye require frequent dosing of an antibiotic to solve this potentially sight-threatening complication. The dosing regimens for the antibiotics can be very frequent. As an example, in severe cases, such as acute bacterial keratitis, dosing is required as often as every 15 or 30 min. 67 Thus, sustained antibiotic delivery by contact lenses can be particularly valuable during treatment of ocular infections. Consequently, the delivery of different antibiotics by contact lenses has been analyzed,17,45,49 being the uptake and release of the antibiotic ciprofloxacin from contact lenses as one of the most widely studied. Ciprofloxacin has a broad spectrum of antibacterial activity against both Gram-positive and -negative bacteria and it is commonly prescribed for treating microbial keratitis, conjunctivitis, or endophthalmitis.68,69 The first studies with ciprofloxacin-soaked conventional and silicone hydrogel contact lenses indicated that the antibiotic uptake was appropriated and the amount of drug released enough for pathogen treatment; however, ciprofloxacin was released too quickly to be clinically useful for extended drug delivery.70,71
To reach a sustained release, a contact lens integrating a thin ciprofloxacin–PLGA film into a pHEMA hydrogel was designed. 56 This drug-eluting system showed zero-order release kinetics at a therapeutically relevant ciprofloxacin concentration for 1 month. The larger thickness of this contact lens could complicate patient acceptance and decrease oxygen and carbon dioxide permeabilities. Nevertheless, this disadvantage has been subsequently overcome due to the new design of a thinner curved contact lens integrating the drug–polymer film. 57
Recently, conventional hydrogel contact lenses that incorporate nanosphere-encapsulated ciprofloxacin have been synthesized. 72 Transparency was preserved in these contact lenses and the proliferation of greater than 107/mL of bacteria added daily over 3 days of culture was inhibited, with up to 5×109 total microbes killed in a single inoculation. These results demonstrate the potential of these contact lenses to provide sustained and effective bactericidal activity.
Corneal injury
Corneal defects with delayed re-epithelization can result from a variety of causes, including corneal dystrophies, recurrent corneal erosions, ocular trauma, corneal surgery, and decreased corneal innervation. Topical application of various agents, such as the epidermal growth factor (EGF), has been reported to accelerate wound healing in vivo. 73
On the other hand, a contact lens can act as a bandage to shield the leading edge of the healing epithelium from damage because of blinking, allowing newly reproduced epithelial cells a greater opportunity to recover the corneal surface. Therefore, contact lens acting in its traditional role as a bandage and in a nontraditional role as a drug delivery device for compounds effective in improving wound healing may enhance the clinical outcome in patients with corneal injury.
Bearing in mind this notion, EGF-soaked contact lenses were developed and their therapeutic activity was tested in a rabbit model of ocular trauma. 74 EGF-treated contact lenses achieved a significantly higher overall healing rate of corneal epithelial defects as compared to saline-soaked contact lenses.
Consistent with this finding, a pilot clinical assay with patients revealed that the use of EGF-soaked contact lenses improved the healing time in noninflamed corneas of patients with delayed corneal re-epithelization. 75 A complete recovery was observed even in patients previously treated unsuccessfully with other methods.
Allergic conjunctivitis
Allergic conjunctivitis affects up to 40% of the general population, with seasonal allergic conjunctivitis accounting for up to 90% of these ocular cases. 76 Antihistamines, such as ketotifen fumarate, are used to alleviate the sign and symptoms of allergic conjunctivitis through multiple pharmacological actions. 77 Ketotifen fumarate is a selective noncompetitive antagonist of histamine H1-receptors and it can also inhibit histamine release from mast cell. Nowadays, ketotifen fumarate is administrated by eye drops and 2–4 applications are required each day for allergic conjunctivitis treatment. As reported in the literature, the inhibition effect of ketotifen fumarate is biphasic. 78 In concentrations above 0.1 mM, ketotifen fumarate induced secretion of histamine from rat and mouse mast cells. At low concentrations (0.05–0.005 mM) it increased in vitro phytohemagglutininin-induced proliferative response of human lymphocytes. Therefore, it is important to maintain a stable concentration in the eye for a long time in treatment of allergic conjunctivitis. To keep a relatively stable ketotifen fumarate concentration in tear fluid, ketotifen fumarate was loaded by soaking in conventional and silicone hydrogel contact lenses. 21 In in vitro assays, all the contact lenses released an amount of ketotifen fumarate higher than the dosage provided by eye drops (25 μg/d) with the majority of the drug released within the first hour. Under these conditions of quick releasing, a lower amount of drug should be loaded into the lens to prevent an overdose. Surprisingly, when experiments were performed in vivo using rabbits, the presoaked silicone hydrogel contact lenses sustained ketotifen fumarate release in an effective dose ∼ 30 μg/mL for ∼8 h. 23 One possible reason suggested by the authors to explain this different behavior is the relatively large volume of solution used to measure drug release in in vitro assays (contact lenses were transferred to 6 mL of solution compared with a tear film volume around 7–30 μL). In this nonreplenishing solution, it is likely that the difference of concentration between the contact lens and solution remains large, causing continuous and quick release. It would seem if the contact lens is placed in a smaller solution volume, such as the tear film, drug will be released until the difference of concentration between these 2 mediums balance. Moreover, as the tear volume is replaced and drug is absorbed into the ocular tissue, more drug will be released from the lens over time.
On the other hand, a remarkable increase in ketotifen fumarate precorneal residence time and bioavailability was detected when imprinted contact lenses were used to release the drug as compared to soaked-contact lenses. The imprinted lenses demonstrated an extended release and relatively constant tear concentration of ketotifen fumarate (170±30 μg/mL) for 26 h under in vivo conditions. 79
Although contact lenses use is contraindicated in allergic patients with more severe symptoms, such as vernal conjunctivitis, with regular monitoring and patient compliance to lens care, successful and safe contact lens wear is achieved in most patients with mild-to-moderate ocular allergy.65,80 For these patients, the sustained release of the pharmaceutical agent, such as ketotifen fumarate, from contact lenses could reduce the discomfort and inconvenience of ocular allergy treatment. In fact, a phase III clinical study has been completed in 2011 in the United States conducted by Vistakon Pharmaceuticals. This trial was a double-blind, randomized, placebo-controlled study enrolling 250 subjects to evaluate the safety of a novel contact lens ketotifen fumarate delivery system in healthy normal volunteers. The different primary measures analyzed, such as lid and lid margin erythema and swelling, conjunctival redness, corneal erosion, corneal staining or corneal edema, fulfill the safety criteria, indicating the potential applicability of these novel contact lenses in patients.
Dry eye
The dry eye syndrome is a multifactorial disease of the tears and the ocular surface, associated with discomfort symptoms, visual disturbance, and tear film instability. In severe cases, this may lead to ocular surface damage. Common clinical signs of a patient with dry eye syndrome include inflammation, increased osmolarity, decreased tear breakup time, and ocular surface epithelial damage. 81 A common treatment method to overcome discomfort symptoms in dry eye is the use of re-wetting agents applied as eye drops.82,83 Various molecules working as rewetting agents, such as hyaluronic acid or hydroxypropyl methylcellulose, have been also included in SCLs and their subsequent release have been analyzed. This lens combination device can provide great comfort in dry eyes and it can be particularly valuable for combating contact lens-induced dry eye. Soaking a variety of both silicone hydrogels and hydrogel commercial contact lenses in a hyaluronic acid solution did not load sufficient amounts of hyaluronic acid and release was complete under 1 h. 84 In contrast, using molecular imprinting strategies, it was possible to synthesize hydrogel contact lenses able to release hyaluronic acid at a controlled rate. This re-wetting agent was released at a therapeutic rate of ∼6 μg/h for 24 h. 85 Also, lenses produced in this work could serve dual roles as comfort and therapeutic contact lenses, as hyaluronic acid has been shown to have therapeutic properties in corneal wound healing and epithelial cell migration. 86
White et al., designed a molecularly imprinted silicon hydrogel contact lens, for the extended release of the other re-wetting agent, the hydroxypropyl methylcellulose. The lenses presented an extended controllable release of hydroxypropyl methylcellulose under physiological flow rates at a linear rate of ∼16 μg/day over a period of up to 60 days. 61 Taking into account that a typical eye drop delivers 0.125 μg of hydroxypropyl methylcellulose and drops are instilled frequently, an application of 20 drops a day yields a cumulative release rate of 2.5 μg/day. Therefore, the daily mass delivery rate from imprinted contact lenses is 6-fold higher than the eye drop release rate that reinforces the potential applicability of these imprinted contact lenses as an alternative approach for dry eye treatment.
In another attempt to alleviate dry eye symptoms, silicone hydrogel contact lenses were soaked with phospholipids (1,2-dimyristoyl-sn-glycero-3-phosphocholine) (DMPC) as these molecules play a key role in the maintenance of tear film stability. Silicon hydrogel contact lenses were able to load the phospholipid and an average of nearly 1 μg of DMPC was eluted within 10 h. 87
Lately, research on the dry eye treatment is focused on the inflammatory etiology of the disease. 88 It is believed that by reducing the eye inflammation, there are relieved the ocular signs and symptoms and decreased the effects on vision-related functioning. 89 Thus, anti-inflammatory drugs, such as cyclosporine A, can be used for the dry eye syndrome treatment of moderate-to-severe dry eye disease. 90 To address the disadvantages of cyclosporine A delivery through eye drops, cyclosporine A delivery from contact lenses have been proposed. Surfactant-laden hydrogel contact lenses, designed for a sustained drug delivery, released cyclosporine A at a therapeutic dosage for a period of about 20 days. 39 Otherwise, the ability of cyclosporine A-soaked silicone hydrogel contact lenses to increase drug residence time and bioavailability compared to delivery via eye drops was also checked. 91 Silicone hydrogel contact lenses maintained cyclosporine A delivery rates within the therapeutic window for 14 days. Moreover, when 20% of vitamin E was incorporated into the lens, cyclosporine A release extended up to 1 month.
Finally, molecular imprinted techniques were used in the design of pHEMA-co-diethylaminoethyl methacrylate-co-polyethylene glycol (200) dimethacrylate SCLs 79 for controlled release of the nonsteroidal anti-inflammatory diclofenac sodium form. According to the authors, the imprinted lenses released diclofenac at a constant rate time of 8.62 μg/h for 1 day, being close to the maximum dose delivered by eye drops, making the lenses only suitable for daily disposable use.
Glaucoma
Glaucoma is a group of progressive optic neuropathies, characterized by the damage caused to the optic nerve, fiber layer, and ganglion cells. If it is not treated, it results in visual field loss. 92 An important risk factor for the nerve damage is the elevated intraocular pressure (IOP), and the restoration of the IOP to the normal level is the most common treatment for glaucoma. 93 Several different classes of drugs are currently prescribed with this purpose, such as prostaglandin analogs, beta-adrenergic receptor antagonists, carbonic anhydrase inhibitors, and alpha2-adrenergic agonists. 94 Braga and colleagues used the supercritical solvent impregnation process to load the carbonic anhydrase inhibitor, acetazolamide, into commercially silicone-based SCLs. In vitro tests indicated that acetazolamide was released during 8 h in an efficient concentration to induce IOP decrease. 54 These findings suggest their use for glaucoma treatment and simultaneously for the correction of refractive deficiencies as the acetozolamide-impregnated contact lenses retain their optical properties. Alternatively, imprinted pHEMA hydrogels that mimic the active site of carbonic anhydrase were designed to generate contact lenses with high affinity for carbonic anhydrase inhibitors, such as acetazolamide or ethoxzolamide. Hydrogels sustained in vitro release of these antiglaucoma drugs for 2 weeks, after which the amount released was still<50%. 58 These hydrogels were cytocompatible and possessed adequate oxygen permeabilities to be used as medicated SCLs; nevertheless, other aspects, such as optical transparency of the lenses remain to be determined.
Delivery from contact lenses of the beta-adrenergic receptor antagonist, timolol, has been widely studied. In in vitro studies, loaded imprinted contact lenses were able to prolong timolol release for more than 24 h 59 and even a more extended release was observed in imprinted contact lenses in which the ratio M/T was increased. 48 In in vivo assays with rabbits, loaded imprinted contact lenses provided a 3.3- and 8.7-fold greater timolol ocular bioavailability than nonimprinted and eye drops, respectively. 95
In a different approach, timolol was loaded into silicone hydrogel contact lenses containing vitamin E as a biocompatible diffusion barrier, and its efficacy reducing IOP was tested in glaucomatous dogs. Timolol delivered from contact lenses achieved the same efficacy as eye drops, but with one-third of the drug loading, indicating a higher bioavailability for contact lenses compared to eye drops. 96 The reduction of the therapeutic drug dosage is particularly interesting to diminish the systemic side effects caused by the use of timolol. 6 Additionally, by incorporation of vitamin E into the lenses, IOP can be significantly reduced for 4-day treatment with continuous wear of lens. 29 Controlled release of timolol from extended wear contact lenses could lead to increased patience compliance, particularly to glaucoma patients who also need vision correction.
The above-mentioned studies with antiglaucoma drug-loaded contact lenses were all carried out in vitro or in vivo using animal models. Interestingly, a pilot study for glaucoma therapy using drug-loaded contact lenses has been also conducted in humans. 97 Human trials involved 3 glaucoma patients who were at one time contact lens wearers, but had to stop due to the difficulty in administering glaucoma drugs, while wearing lenses. Contact lenses soaked with their prescribed glaucoma drugs, timolol and brimonidine tartrate (alpha2-adrenergic agonist), were used. Patients wearing the contact lenses for 30 min per day for 2 weeks showed IOP values equivalent to those obtained with previous eye drop treatment and no ocular toxicity was observed. These data are promising in support of the applicability of contact lenses for glaucoma therapy, but further research, with a higher number of patients, is necessary to fully confirm this use.
Conclusions
Considering the disadvantages associated with topical ocular administration of drugs by eye drops (i.e., low bioavailability, frequent instillation requirement, patient compliance, potential systemic side effects, efforts have been focused in the development of new therapeutic devices for delivery of ophthalmic drugs. In this context, therapeutic contact lenses can be considered as an excellent alternative to release ocular medication. An ideal SCL-based ophthalmic drug delivery should exhibit a high drug loading and controllable drug release. While the first generation of drug-soaked contact lenses released the drug very quickly, progress in the field has led to produce therapeutic contact lenses by other techniques (i.e., molecular imprinting) with higher therapeutic loading and controlled, extended release. Most of the studies performed to evaluate contact lens drug delivery systems were in vitro assays. In vivo validation of therapeutic contact lenses has not been so widely studied and this aspect deserves further research. On the other hand, efforts should be led to generate therapeutic contact lenses with physical and mechanical properties that mimic those of commercial lenses on the market. Thus, drug-loading contact lenses could be potentially used as combined devices for simultaneous therapeutic and correction of refractive deficiencies.
Footnotes
Acknowledgments
We would like to thank the Universidad Complutense de Madrid (Project GR35/10-A-920777), the Ministry of Economy (Project SAF 2010/16024), and the Institute Carlos III (RETICS RD07/0062/0000) for their funding contribution to this publication.
Author Disclosure Statement
No competing financial interests exist.