
Abstract
Abstract
Purpose:
To develop a minimally invasive rabbit model of postoperative anterior chamber (AC) inflammation using a commercially available frequency doubled Nd:YAG laser [intended for selective laser trabeculoplasty (SLT)].
Methods:
Escalating laser energy was applied to the iris of male Dutch-belted rabbits and the subsequent inflammatory response was observed to determine the laser dose required to generate self-limiting inflammation of at least 3 days' duration. In subsequent experiments, 10 eyes of 10 male Dutch-belted rabbits underwent baseline slit lamp examination, intraocular pressure (IOP), and AC flare meter readings. Starting 1 day before laser application, 5 animals received topical 20 μL dexamethasone 1% to 1 eye 4 times daily for 5 days. Five control animals were treated with saline. Masked assessments of flare, cells, and IOP were made daily for 7 days. Histopathologic changes were assessed in enucleated eyes.
Results:
Compared to controls, dexamethasone-treated rabbits had less postlaser AC flare on postoperative day (POD)2 (19±5 vs. 44±21photons/ms, P=0.03) and POD3 (16±9 vs. 33±11 photons/ms, P=0.03). In dexamethasone-treated rabbits, clinically graded flare (on POD1) and cells (on POD1 and 2) were lower than controls, but did not reach statistical significance. In the control group, IOP was significantly lower than the dexamethasone-treated group on POD2 (14.1±3.4 vs. 19.8±1.1 mmHg, P=0.03) and POD3 (14.2±2.2 vs. 19.0±2.2 mmHg, P=0.01). Histopathology showed pigment clumping and changes limited to anterior layers of the iris.
Conclusions:
Commercially available SLT laser can be used to create a minimally invasive, steroid-responsive animal model of anterior uveitis with the potential for use in the evaluation and comparison of drugs intended to treat AC inflammation.
Introduction
A number of experimental animal models of uveitis have been reported. Several retinal antigens have been used for their uveitogenic properties, to immunize various animals, and thereby induce experimental autoimmune uveoretinitis (EAU).3,4 Another model called the experimental melanin protein-induced uveitis uses bovine uveal tissue antigens for immunization to induce inflammation that is more limited to the uveal tissues.5,6 Other procedures to generate uveitis include, topical application of prostaglandin E2 (PGE2), 7 a paracentesis procedure, 8 subcutaneous injection of the mycobacterium tuberculosis H37Ra antigen,9,10 intravitreal injections of bovine serum, 11 horse serum, 12 or egg albumin, 13 intracameral injection of streptococcus beta-hemolytic group A, 14 and intravenous, intraperitoneal, or footpad injection of endotoxin in rats. 15
Some methods, such as the use of topical PGE2 for inducing anterior segment inflammation are fairly short in duration, providing limited opportunity for observing the effect of a therapeutic agent. Most of the above methods are invasive, have limited repeatability because of dependence on the individual animal's variable immune response and can leave permanent blinding sequelae. These immunogenic procedures can cause severe inflammation for months, and require sacrifice of the study animals. Also, immunologically induced inflammation differs significantly from postoperative inflammation. In the former, the source of inflammation remains in place until the inciting antigen is cleared by the body's defense mechanisms. In autoimmunity-mediated mechanisms, the pathological process is ongoing despite the removal of the inciting antigen from the body. On the other hand, postoperative inflammation is likely a one-time traumatic insult that leads to the breakdown of the blood–aqueous barrier. Hence, antigenically induced inflammation may not be the best model to study postoperative anti-inflammatory therapies. Also, models that involve inadvertent posterior segment inflammation, along with the desired anterior segment inflammation, may not be the best for evaluation of topical therapies with excellent anterior segment penetration and potency, but poor posterior segment penetration.
A new, less invasive and more predictable uveitis model will be a valuable tool in the development of anti-inflammatory therapies. Also, a transient inflammation of a few days duration may allow adequate time for study of anti-inflammatory therapy with limited consequences for the study animal.
Selective laser trabeculoplasty (SLT) is used clinically as a treatment for elevated IOP. 16 A frequency doubled 532 nm Q Switched Nd:YAG laser is applied as fixed spots of 400 μm in size and energy of 0.4–2.0 millijoules (mJ) for 3 ns each to the trabecular meshwork. The IOP usually is reduced for months to years after the procedure, with minimal histopathologic changes. 17 The low fluence, short duration laser energy, based on the principles of selective photothermolysis, targets intracellular melanin, causing no coagulative damage, and little structural change to the surrounding tissues.18–21 Application of SLT spots to the pigmented iris tissue offers an opportunity to create anterior segment inflammation with limited tissue damage. To the best of our knowledge, this method of creating experimental anterior uveitis has not been reported previously.
The goal of this study was to evaluate the possibility of generating self-limited anterior segment inflammation in a rabbit model using application of SLT spots directly to the iris tissue. This report details the preliminary work involved in determining the laser energy required to generate such inflammation. The histopathologic consequences of laser applications were studied. The steroid responsiveness of the model was tested to demonstrate a potential role for the model in the study of anti-inflammatory therapies for the treatment of anterior uveitis.
Methods
The study was conducted in 3 phases. All animal experiments described herein were approved by the Institutional Animal Care and Use Committee of the University of Nebraska Medical Center before the study start. The research described here adhered to the ARVO Statement for the Use of Animals in Ophthalmic and Visual Research. In Phase 1, the irides of 2 enucleated rabbit eyes were subjected to the escalating power of SLT laser ranging from 0.4 to 1.2 mJ. This was done to confirm the absence of any gross coagulative and disruptive changes to ocular tissues.
The purpose of Phase 2 of the study was to determine the energy level and number of spots required to produce inflammation of a few days duration. The objective was to create inflammation that was self-limiting without significant damage to ocular tissues, yet long enough to allow the study of uveitis treatment modalities. The specific power and number of spots were chosen empirically given the lack of available data from similar experiments. Male Dutch-belted rabbits, 37 to 40 weeks of age, were used in this phase of the study. While the animal was anesthetized with a cocktail of ketamine (15 mg/kg) and xylazine (3.75 mg/kg) administered intramuscularly, a slit lamp examination was performed and baseline measurements were made. After a topical drop of proparacaine (0.5%) anesthetic to the cornea, ocular measurements included IOP by pneumatonometry (Classic 30; Reichert Ophthalmic Instruments, Inc., Depew, NY) and flare readings with a laser flare-cell meter (KOWA model FM 600). The cells and flare were graded according to the SUN Working Group Grading Scheme. 22 Laser treatments commenced immediately following baseline examinations and measurements. Escalating doses were used to establish the power and number of nonoverlapping spots needed to generate a mild inflammation that persisted for at least 3 days. A doubling of the baseline flare value was considered significant. Measurements were continued for up to 3 days with a follow-up measurement at 7 days to confirm a return of flare to baseline levels. Initially, 0.6 and 1.0 mJ of energy were used and 30 spots were placed along the peripheral iris of 1 eye of 1 rabbit each. Postoperatively, animals were examined for the presence of flare for up to 3 days. Subsequent protocols included 50 and 100 spots of 1 mJ, 50 spots of 2.0 mJ, 100 spots of 1.5 mJ, and 100 and 150 spots of 2.0 mJ. The maximum laser power (200 spots of 2 mJ) was limited by the maximum available energy from the commercial SLT instrument and the number of spots was limited by the area available for laser spot placement on the iris tissue. Laser spots were uniformly applied over the iris tissue starting at the most peripheral iris and covering the more central tissue as the number of spots increased. In initial experiments, spots were at least 1 spot width apart. However, experiments with a greater number of spots required a more confluent placement of laser spots. The central 1–2 mm of the iris was not treated because of the potential of injury to the iris sphincter and native lens. Pneumatonometry, slit lamp biomicroscopy, and laser flare meter readings were performed on all study days. The endpoints used for the assessment of inflammation thus generated were clinically observed cells and flare, and objective flare measurements by an aqueous flare meter.
In phase 3 of the study, the response of the observed inflammation to topical steroids was evaluated. Ten rabbits were divided into 2 groups of 5 each; Group A was administered one 20 μL drop of dexamethasone 1%, 4 times daily (9am, 11am, 2pm, and 5pm) to one randomly chosen eye for 5 days starting 1 day before SLT. The same administration schedule was applied to Group B, which was dosed with 20 μL sterile saline (Eye Stream; Alcon, Ft. Worth, TX) instead of dexamethasone. Based on the results of Phase 2, a regimen of 200 spots of 2 mJ each was selected for laser treatment. Tonometry, slit lamp examination, and laser flare meter readings were repeated as described in Phase 2. Measurements were made by an observer masked to the assigned treatment of each rabbit. All rabbits used in Phase 3 had been lasered at least once before during phase 2 of the study. Animals were reused for this phase after a return to baseline (as assessed by cells, flare, and IOP). All values are reported as mean±standard deviation unless otherwise noted. Data means were compared using paired t-tests for continuous variables and nonparametric equivalents for discrete ordinal variables. Seven days after the laser treatment for Phase 3, the study animals were sacrificed with an overdose of intravenous sodium pentobarbital (150 mg/kg) and histopathologic examinations were performed on ocular tissues.
Results
Phase 1
No obvious tissue shrinkage or disruption was observed during the application of SLT to enucleated eyes. The observed tissue response comprised of microcavitation bubble formation, minimal flattening of the iris surface corresponding to the area of the laser spot, and tissue blanching in the area of the laser spot. Greater blanching was observed with higher laser powers and in the eye with subjectively greater pigmentation.
Phase 2
Phase 2 of this study involved observations at increasing laser power and number of spots to produce a consistent flare response. Values after total laser application in parentheses represent laser energy per spot times the number of spots applied. In 1 rabbit treated with 18 mJ (0.6 mJ×30 spots), no significant increase in flare was observed on day 1. At 30 mJ (1 mJ×30 spots), significant flare was observed on day 1, which returned to baseline by day 2 (n=1). In 3 of the 4 rabbits treated with 50 mJ (1 mJ×50 spots), 1 rabbit treated with 75 mJ (1.5 mJ×50 spots), and 1 rabbit treated with 100 mJ (2 mJ×50 spots), no significant increase in flare was observed on day 1. Two rabbits treated with 112.5 mJ (1.5 mJ×75 spots) had significant flare on days 1 and 2 returning to baseline by day 3. At higher doses, a more consistent and sustained response was observed (Fig. 1). At 400 mJ (2 mJ×200 spots), 4 of 4 rabbits treated had increased flare in the anterior chamber (AC) that persisted for at least 3 days and returned to baseline values by day 7. Based on these experiments, 200 spots of 2 mJ each was chosen as the laser power for Phase 3.
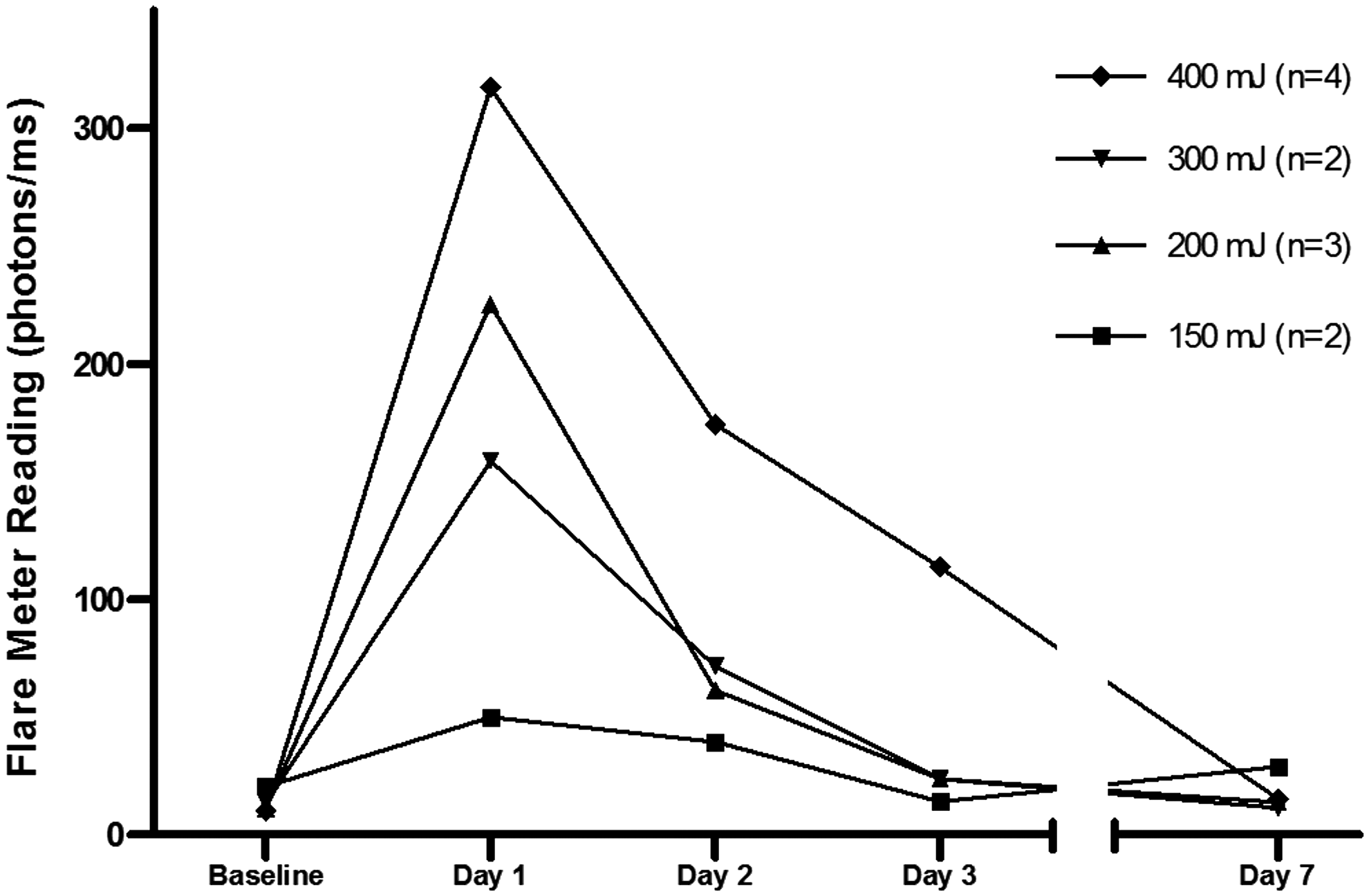
Flare response of laser-treated eyes at increasing laser energy levels. Laser spots were applied immediately following baseline flare measurements. A dose–response relationship was observed between the laser energy applied and the ensuing anterior chamber flare.
Phase 3
This phase of the study evaluated the steroid responsiveness of the inflammation generated by the laser. Rabbits treated with dexamethasone had an increase in flare from a baseline of 9.7±2.9 photons/ms to a peak of 92.0±68.5 photons/ms on day 1, which progressively reduced to 23.0±3.8 photons/ms by day 5 (Fig. 2). In the control group, flare increased from a baseline of 15.7±6.5 photons/ms to a peak of 85.5±42.6 photons/ms on day 1, subsequently, progressively resolving by day 5, to 18.8±7.8 photons/ms. Flare was significantly higher in the control group as compared to the dexamethasone-treated group on day 2 (43.7±21.2 photons/ms vs. 19.1±4.8 photons/ms, P=0.03) and day 3 (33.4±11.0 photons/ms vs. 16.1±8.7 photons/ms, P=0.03) after laser. There was no difference in observed flare between the 2 groups at baseline or on postlaser days 1, 4, and 5.

Comparison of flare by a laser flare meter in the dexamethasone- and saline-treated groups after laser treatment to the iris. Laser spots were applied immediately following baseline measurements. Error bars represent SEM. P-values were obtained using the unpaired t-test comparing the 2 groups. Asterisks indicate a statistically significant difference.
No cells or flare were detected in either group by the slit lamp examination at baseline. Clinically graded flare peak was 1.8±0.4 on days 1 and 2 in the dexamethasone group and 2.4±0.5 on day 1 in the control group (P=0.09) with a subsequent progressive resolution in either group (Fig. 3). Cells peaked on day 2 in both the dexamethasone (2.2±0.8) and control group (2.6±0.5) with a subsequent resolution by day 5 (Fig. 4).

Comparison of clinically graded flare (grades of 0 to 4) in the dexamethasone- and saline-treated groups after laser treatment. Laser spots were applied immediately following baseline measurements. Error bars represent SEM. The P-value was obtained using the Mann–Whitney test. Asterisk indicates a borderline statistically significant difference.
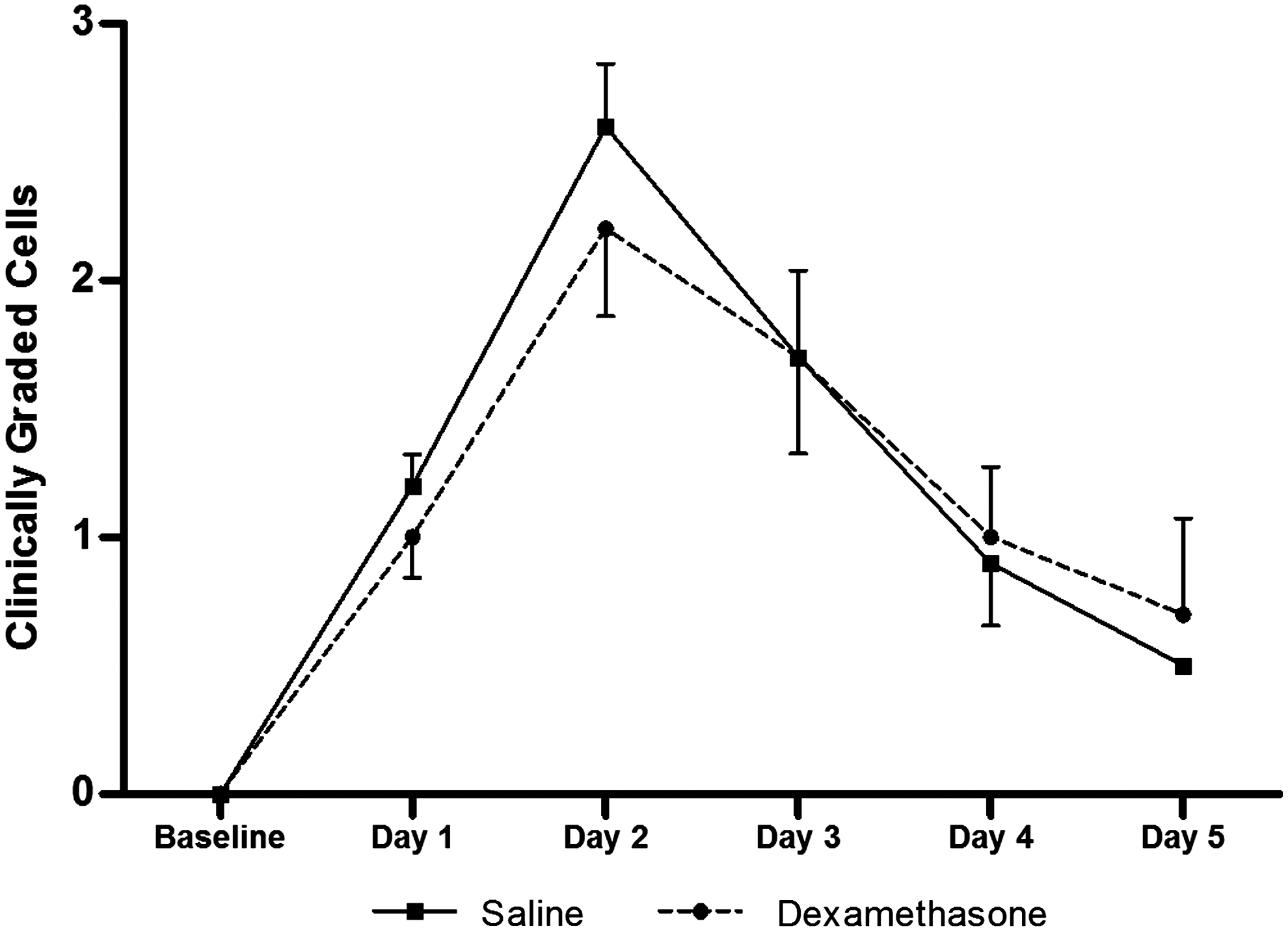
Comparison of clinically graded cells (grades of 0 to 4) in the dexamethasone- and saline-treated groups after laser treatment. Laser spots were applied immediately following baseline measurements. Error bars represent SEM. The difference between the groups did not reach statistical significance.
At most observation times (except in the control group on day 4), IOP was significantly lower in both groups compared to their respective baselines. Compared to the treatment group, IOP was significantly lower in the control group on days 2 (14.1±3.4 mmHg vs. 19.8±1.1 mmHg, P=0.03) and 3 (14.1±2.2 mmHg vs. 19.0±2.2 mmHg, P=0.01), coinciding with the days of significantly higher flare in the control group (Fig. 5). The significance of IOP lowering on these days is limited by the lack of IOP matching at baseline where the control group had a lower baseline IOP than the treatment group (24.6±2.1 vs. 28.7±2.1 mmHg, respectively, P<0.01).
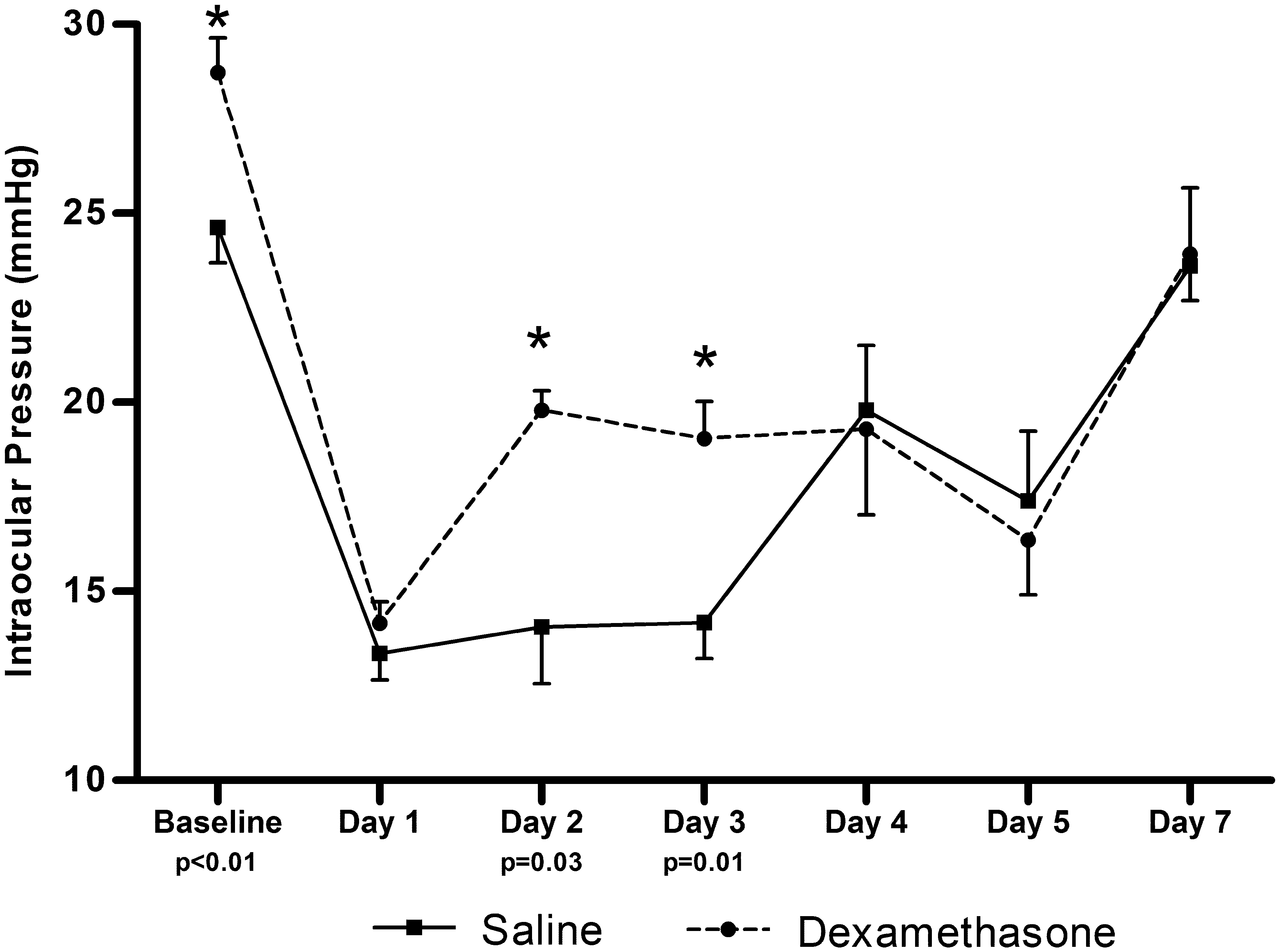
Comparison of intraocular pressure in the dexamethasone- and saline-treated groups after laser treatment. Error bars represent SEM. The difference between the groups was significant at baseline and postoperative days 2 and 3. P-values were obtained using the unpaired t-test. Asterisks indicate a statistically significant difference.
Histopathology
On gross examination, tissue changes in the enucleated specimens were limited to the iris tissue with large areas of patchy depigmentation observed on the anterior iris surface, corresponding to the application of laser spots (Fig. 6a, b). Histopathologic changes were limited to the anterior layers of the iris and comprised of localized flattening of the surface stroma with underlying large clumps of extra and intracellular pigment (Fig. 7a, b). The localized flattening did not show any evidence of adjacent coagulative changes. The fibrovascular structures of the iris and the posterior layers appeared fairly well preserved in the lasered eyes. No changes were observed in the cornea, ciliary body, lens, retina, or choroid when comparing the lasered eye to the contralateral control eye.

The iris tissue of the enucleated rabbit eye,
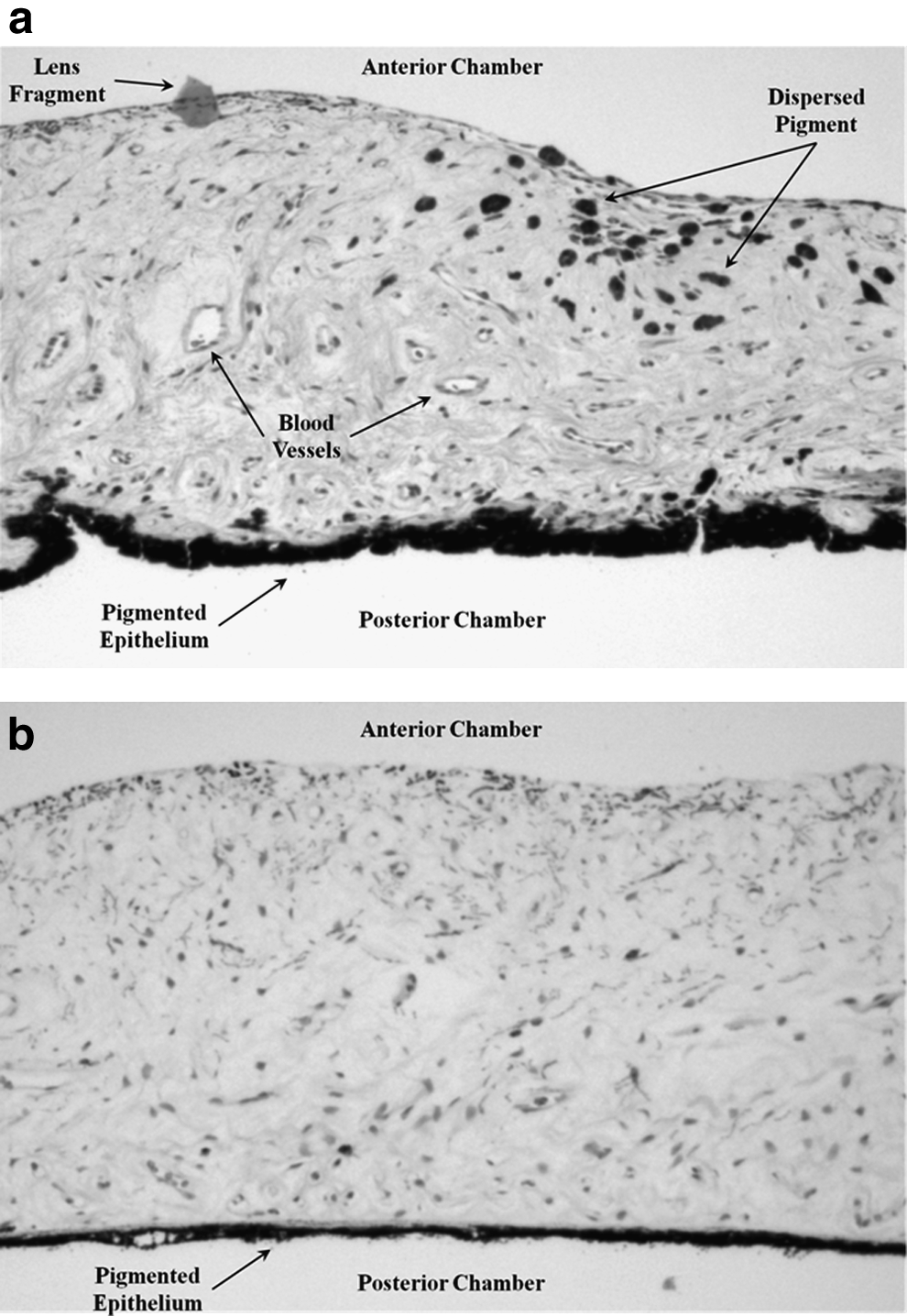
Photomicrograph of hematoxylin and eosin stained iris cross-section of a rabbit eye,
Discussion
This study describes a novel model of ocular inflammation in rabbits utilizing a commercially available frequency doubled Nd:YAG laser. Anterior segment inflammation can result from a myriad of causes with postoperative inflammation being one of the most common encountered in any clinical practice. The inflammation observed in our study is more akin to surgically induced inflammation rather than one produced by the introduction of foreign antigens. The latter is more likely to simulate inflammation from autoimmune and infectious causes.
The laser paradigm provides a longer window of observation of the inflammatory response from a single insult, as compared to the much shorter duration of inflammation generated using topical prostaglandins. 7 The model is less invasive than one that requires injections of antigens into the eye; the intraocular placement of the needle alone can generate ocular inflammation. 8 Because no needle is inserted into the eye, the current model avoids any accidental introduction of microorganisms and ocular infection. Infection can increase the amount of inflammation observed and likely will not be responsive to an anti-inflammatory drug being evaluated in a study. This potentially could make the drug under study appear less efficacious in controlling inflammation and the results would be harder to interpret.
Dutch-belted rabbits tolerate the laser treatment well, based on behavior and the return to baseline of all observed parameters by 1 week. The changes observed on histopathology were very limited. Given the clinical experience with SLT and the observed minimal histopathologic changes to the tissues, 20 the generation of inflammation can be repeated in the same animal.
Effects of laser application to iris tissue with lasers other than the SLT have been reported previously.23–28 To the best of our knowledge, this is the first report of the effects of application of SLT laser directly to the iris tissue. Compared to argon laser, SLT laser is devoid of coagulative and mechanical tissue damage when applied to the trabecular meshwork of eye bank eyes. 20 SLT laser uses a small fraction of the energy needed by argon laser in performing laser trabeculoplasty. SLT laser selectively targets the pigmented cells in the target tissues leading to cracking of intracytoplasmic pigment granules and disruption of endothelial cells. 19 This may explain why minimal changes were observed in the histopathology sections despite large areas of depigmentation observed grossly on the tissue surface. The depigmenting properties of Q switched frequency doubled Nd:YAG laser have been used for the treatment of pigmented hypertrophic scars in the field of dermatology. 29 When used clinically to perform trabeculoplasty, the 400 μm spot size of the SLT laser can lead to some inadvertent overlap with tissues anterior or posterior to the trabecular meshwork. The histopathologic findings of this study suggest that some overlap of laser spots on the iris tissue during trabeculoplasty at clinically used energy levels may be innocuous. However, the application of laser spots to the human iris tissue has not been studied and cannot be considered safe without additional investigation.
The exact mechanism by which the laser generated inflammation in our model has several possible explanations. The inflammation may have been a consequence of the mechanical stimulation of the iris (without photocoagulation) and melanocyte disruption secondarily leading to an inflammatory response. Alternatively, the breakdown of the blood–aqueous barrier may have been a direct effect of the laser spots. The peak absorption of hemoglobin is close to the 532 nm wavelength of frequency doubled Nd:YAG laser. 30 Absorption of such energy by blood vessels forms the basis of treatment of port wine stains with Nd:YAG laser. 31 A highly vascular tissue like the iris may absorb energy by the circulating red blood cells that in turn induce a breakdown of the blood–aqueous barrier.
The reduction in measured flare by dexamethasone supports the steroid responsiveness of our model. The lack of difference in flare between the 2 groups on day 1, but the significantly reduced flare in steroid-treated animals on days 2 and 3, suggest that steroid pretreatment did not alter the impact of the initial laser insult to the tissues. However, eyes treated with topical steroid had less flare and higher IOP during resolution of the inflammation than control eyes. These results suggest that the model may be useful for comparison or preclinical evaluation of anti-inflammatory therapies used to control postoperative inflammation. A predictable, simple model such as the one currently described can facilitate a quick screening of drug molecules being evaluated for potential therapies.
The measurement of flare using a flare meter is a validated technique for the study of ocular inflammation. 32 Clinical assessment of cells and flare is a subjective technique at best, with significant inter- and intra- observer variability despite well-described grading scales. 33 The flare meter can circumvent this problem by providing a measure of inflammation on a continuous scale, thereby significantly reducing the sample required to obtain statistically significant differences. For example, even though the difference in flare meter readings reached statistical significance on days 2 and 3 with a sample size of 5, the sample size required for the difference in cells to be significant between the 2 groups in our study (with a power of 80%, and alpha error of 0.05) will be 42 rabbit eyes.
Our study and model have several limitations. The sample size was small. This study was planned as a proof-of-concept study and no ad hoc sample calculations were made. This was done to minimize the number of animals affected during the execution of the study. Even with the limited sample size, the goals of the study were accomplished. The limited sample number, with reuse of some of the study animals after return to baseline, was sufficient to establish the dose of laser needed to generate clinically useful inflammation. A statistically significant difference in objectively measured flare and borderline significant difference in subjectively graded flare could be demonstrated with the use of a potent steroid. The data obtained from this study potentially can be used for sample size calculations of future planned studies. Because of technical limitations of the commercially available laser, we were unable to establish the peak of the dose–response curve for the laser application. The highest response was seen with the highest power of the laser used. It may be possible to generate more and longer lasting flare with even higher laser energy levels. In the future, a custom-designed laser with higher available energy levels may be able to accomplish this. Nevertheless, use of the commercially available version of the laser generated clinically useful flare without significant trauma to the study animals. As mentioned above, this model likely represents surgically induced inflammation and is not likely to be representative of other endogenous infectious and noninfectious uveitis encountered in clinical practice. The mean flare generated on day 1 was significantly lower in phase 3 of the study as compared to phase 2 for an identical dose of the laser. All study animals used in phase 3 had been lasered at least once previously in the same eye in phase 2 of the study, with varying amount of laser applied to each individual rabbit. Repetition of laser in the same animal, after a return of flare reading to baseline, was done to minimize the number of animals sacrificed for this pilot study. This may explain a lower amount of flare seen in phase 3 with 400 mJ of laser energy used as compared to phase 2, where repeated application of laser to the same animal may be associated with diminishing returns in terms of the flare generated. This is similar to a lower initial efficacy of SLT laser therapy upon repeat application, as compared to initial application, when used for trabeculoplasty in humans. 34 However, this should not affect the conclusions from phase 3 of the study as both the control and dexamethasone-treated eyes had received prior laser and the purpose of this phase was to determine the steroid responsiveness of the inflammation generated. As an additional limitation, as with any animal model, the results obtained from this model may or may not apply to human situations. The blood–aqueous barrier in rabbits is known to be less robust than that in primates. 35 However, there are several reasons to use rabbits. They are relatively easy to handle and maintain and may be the species of choice for drug screening experiments before proceeding with more costly and robust primates. Dutch-belted rabbits are preferred over albino rabbits because of the pigmented iris, which may be necessary for the needed tissue response to laser.
In summary, this study describes a clinically useful, steroid responsive AC model of inflammation in Dutch-belted rabbits by using a commercially available Nd:YAG laser. Future studies involving larger numbers, other species like nonhuman primates, and additional anti-inflammatory medications will help determine the validity of the model in a wider variety of experimental and clinical circumstances.
Footnotes
Acknowledgments
The authors extend a special thanks to Tara Rudebush, Stacey Wenthur, and Brooke Dworak, for their help with animal handling, and to Dr. Gerald Christensen and Dr. William West for their expertise in interpreting the histology slides. Support: Research to Prevent Blindness, Allergan Horizon Grant, Pfizer.
Author Disclosure Statement
No competing financial interests exist.