
Abstract
Abstract
New technologies for delivery of drugs, such as small molecules and biologics, are of growing interest among clinical and pharmaceutical researchers for use in treating anterior segment eye disease. The challenge is to deliver effective drugs at therapeutic concentrations to the targeted ocular tissue with minimal side effects. To achieve this, a better understanding of the unmet needs, what is required of the various methods of delivery to achieve successful delivery, and the potential challenges of anterior segment drug delivery is necessary and the primarily aim of this review. This review covers the various physiological and anatomical barriers that exist for effective delivery to the targeted tissue of the eye, the pathological conditions of the anterior segment, and the unmet needs for treatment of these ocular diseases. Second, it reviews the novel delivery technologies that have the potential to maintain and/or improve the drug's therapeutic index and improving both patient adherence for chronic therapy and potential patient outcomes. This review bridges the pharmaceutical and clinical research/challenges and provides a detailed overview of anterior segment drug delivery accomplishments thus far, for researchers and clinicians.
Introduction

Anatomy of the human eye representing different locations possible for drug delivery implants.
Drug delivery systems that target the anterior segment offer many advantages over conventional eye drops and fulfill an unmet need by increasing drug bioavailability, extending the duration of release, decreasing the amount of drug delivered, minimizing systemic exposure, and improving patient compliance and adherence, thus potentially fostering better outcomes and the quality of life over time.
Challenges: ocular drug delivery barriers
An important factor in drug delivery is the ability of a molecule to cross the physiologic barriers and penetrate the target tissue. Common barriers to ocular delivery include the ocular surface epithelial tight junctions, which affect diffusion of drugs. Tight junctions, such as gap junctions and zonula occludens (ZO), are the branching networks of proteins that are present to seal the space between cell membranes. Drug penetration depends on the integrity of tight junctions as well as the physicochemical properties of the drug, such as lipophilicity, aqueous solubility, molecular weight, polarity, and ionic charge. When formulating a drug for delivery to the eye, it is common to use vehicles that enhance penetration across these ocular tissue barriers to improve bioavailability. Drug metabolism as well as drug transporters present in the ocular tissue can play an important role in the amount of drug that actually enters the target tissue. A number of transporters in cornea and conjunctiva such as amino acid/peptide, nucleoside, organic anionic, organic cationic, and efflux pump transporter P-glycoprotein have been reported.1–5 Lastly, diseases that involve inflammation of the eye are often characterized by increased vascularity, vasodilation, and breakdown of the blood–aqueous barrier. Such changes occurring at the molecular and cellular tissue level can further affect and alter the local drug penetration, tissue bioavailability, pharmacokinetics, metabolism of the drug, and systemic absorption.
Tear film and bioavailability
Periorbital and precorneal factors such as blinking, eye lashes, tear film turnover, and induced lacrimation (reflex tearing) promote rapid surface clearance of topically applied drops. 1 Under physiological conditions the entire tear film is restored every 2–3 min resulting in clearance of topical solutions from the surface within 15–30 s. 6 Because of rapid tear film turnover, evidence suggests that only 1% to 5% of a topically applied solution has intraocular bioavailability due to dilution by the tear film and rapid conjunctival and episcleral lymphatic and vascular clearance.7,8 Only a fraction of the topical dose escaping conjunctival and episcleral barriers and tear film removal can then permeate across the cornea and/or conjunctiva, and sclera, a fibrous, porous tissue that is more permeable to macromolecules. 7
Once a drug enters the ocular tissue, the main ocular clearance pathway is the anterior route. Topically administered hydrophilic compounds are cleared mainly through the slower anterior route. The anterior route of clearance is primarily passive diffusion of drug into the anterior chamber and then excretion via the trabecular meshwork (TM) and Schlemm's canal and/or the uveoscleral pathway. Thus, drug clearance from the aqueous humor is through 2 routes: aqueous turnover and TM and uveal venous blood flow. 9 Clearance through the TM and uveoscleral pathway depends on the anterior chamber fluids and the permeability of drug. Once through the TM and/or the uveoscleral system, it enters the uveal venous system. 10 Observed differences in ocular penetration between in vivo and ex vivo delivery studies may be attributed to active ocular clearance both on the surface and from within the ocular tissue; obviously, active aqueous drainage is only present in living tissue.8,11,12 The conjunctiva is rich with lymphatics and blood vessels, which contribute to drug clearance. It was reported that after subconjunctival injection of small hydrophilic molecules, clearance is mainly through the surface blood vessels, whereas large hydrophilic molecules clear mainly through the lymphatic system. 13 Further, the rate of ocular clearance can also be affected and altered by the compound itself. Lipophilic drugs are capable of penetrating the endothelial walls of the uveal blood vessels, and therefore lipophilic drugs are cleared out from the anterior chamber more rapidly. 9
Cornea/conjunctiva and drug bioavailability
The cornea is the outer transparent tissue of the anterior segment, and it represents a highly impermeable barrier to drug penetration. It is composed of 5 layers (Fig. 2) with an average central thickness of 0.52 mm and a central radius of 7.8 mm. 14 The corneal epithelium, which is the outer layer, represents almost 90% of corneal cells and consists of 5 to 6 layers of stratified, squamous, nonkeratinized cells that have tight as well as gap junctions between cells, thus limiting the permeability of molecules. 6 In the corneal epithelium, the ZOs are a virtually impermeable barrier to fluid. In terms of drug delivery, these ZOs within the anterior segment help to establish diffusion barriers, such as the blood–aqueous barrier. This barrier, which can impede drug delivery from systemic blood flow, is established by the endothelial cells of the ciliary body vascular system and the nonpigmented ciliary epithelium tissue. 6 The presence of these tight junctions such as ZOs within the corneal and conjunctival epithelium can hinder paracellular transport of drugs when applied topically such as hydrophilic drugs. 9 Therefore, hydrophilic drugs have less permeability than lipophilic drugs in the cornea and conjunctiva. 9 Numerous articles have been written that focus on these intracellular barriers in the various ocular tissues and their impact on the diffusion of various sized and charged molecules.15–18
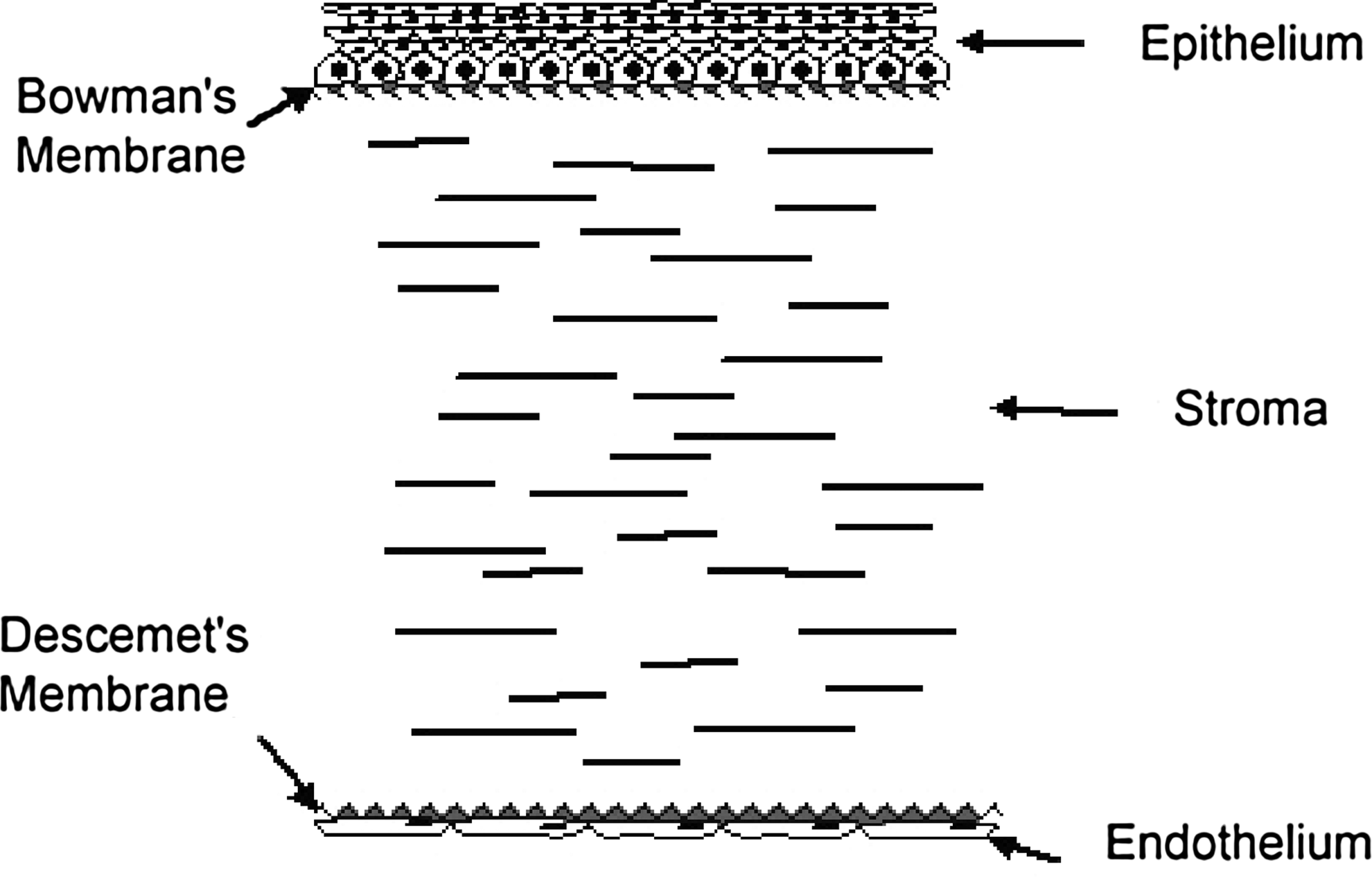
Cross-section of the cornea showing 5 distinct layers: epithelium, Bowman's membrane, stroma, Descemet's membrane, and endothelium.
Underneath the corneal epithelium are the corneal stroma and endothelium, which comprise additional barriers to drug penetration. While the corneal epithelium and endothelium tend to be more permissive to nonpolar, lipophilic drugs, the stroma has a higher water content and is relatively more permeable to polar, hydrophilic compounds. 19 Damage to these structures within the cornea from a trauma or disease can result in alterations in drug permeability. For example, mechanical abrasion to the corneal epithelium is known to enhance penetration of topical medications, especially water-soluble compounds. 19 It is also well established that the commonly used preservative benzalkonium chloride enhances corneal permeability to topically applied medications by disrupting the cell membranes and tight junctions. 20 Further, the corneal epithelium is more permeable to topical medications in patients with dry eye syndrome again due to the mechanical disruption of the epithelial cellular barriers. Treatment with preservative-free artificial tears has been shown to restore barrier function in such patients. 21
Drug absorption occurs via corneal and noncorneal pathways. A noncorneal pathway involves the conjunctiva, a mucous membrane that lines the anterior portion of the globe (bulbar conjunctiva), and the underlying surface of the inferior and superior lids. Noncorneal absorption of a drug is primarily through the bulbar conjunctiva, through sclera, and followed by uvea. 9 Noncorneal absorption may contribute significantly to intraocular drug levels after topical dosing of such hydrophilic compounds and larger molecules, for example, pilocarpine and inulin.22,23 It may be possible to use noncorneal absorption as a method for delivering drugs to ocular tissues without exposing the cornea to high concentrations; this would require special medical devices that are now in development.
Compared to the cornea, the conjunctiva (palpebral and bulbar) is more permeable to polyethylene glycol (PEG) molecules. 24 This is relevant for sustained delivery of proteins and polymers, since PEGylation can slow down the degradation and also provide water solubility to hydrophobic drugs and proteins, thus making them more amenable for a delivery technology. 25 Evidence suggests that the cornea is 15–20 times less permeable to PEG molecules with mean molecular weights (mwt) from 200 to 1000 than the conjunctiva and sclera, 24 indicating that the trans-scleral delivery for drugs having a molecular weight between 200 and 1000 might be more effective. There was no reported difference in the permeability of PEGs between the palpebral and bulbar conjunctiva. 24
Episclera/sclera and drug bioavailability
The sclera is a tough, fibrous tissue that extends from the cornea back to the optic nerve at the posterior portion of the eye. The sclera offers an attractive pathway for delivering drugs to the intraocular compartments due to its porous collagen and proteoglycan matrix. 26 Trans-scleral drug delivery may be more feasible than transcorneal or transconjunctival drug delivery because of the sclera's large accessible surface area (95% of total surface area of the globe), high degree of hydration, and the lack of lymphatics.27,28 The intracellular space of the sclera's fiber matrix may determine the movement of drugs dependent on the area of drug placement on the globe. 29 The posterior sclera (sclera posterior to the insertion of the rectus muscles) is composed of a looser weave of collagen fibers than the anterior sclera, which could explain the higher permeability of compounds through the posterior sclera than in the anterior sclera. 30 Further, scleral permeability may be dependent on the charge of the drug: positively charged compounds may have a more-favorable diffusion profile through the negatively charged scleral porous proteoglycan matrix.29,31 In vitro experiments have demonstrated that the sclera is permeable to molecules as large as 120-kDa fluorescein isothiocyanate (FITC)-conjugated dextrans 32 and 150-kDa IgGs. 33
Protein-mediated binding and active transporter systems are currently being investigated as a means to improve ocular bioavailability and drug penetration.34,35 Protein-mediated binding or transporter binding involves a targeted modification of a drug to allow it to bind to a cell membrane-bound transporter (protein) that plays an active role in transport across the cellular membranes. The transporters within the sclera, cornea, and conjunctiva can be made amenable to transporting specific ions and/or molecules that are adherent to the drug compounds. 1 Numerous reviews have been written on the various types of transporter systems in the ocular tissues that include efflux transporters and influx transporters that can shuffle drugs between cells or into/out of the cell cytoplasm.6,35 In general, drug binding to transporters must be reversible, and a dynamic equilibrium must be established between the bound and unbound molecular species to allow effective drug penetration. Their identification has become an exciting means to improve upon drug permeability and ocular penetration.
Anterior segment diseases
The anterior segment is the front third of the eye that includes the cornea, conjunctiva, iris, ciliary body, aqueous humor, and the lens. 36 Briefly discussed below are a few anterior segment diseases for which targeted drug delivery to the anterior segment may be useful.
Dry eye syndrome
Dry eye syndrome is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear-film instability with potential damage to the ocular surface. 37 It is a common eye condition, with a prevalence ranging from 8.4% in adults younger than 60 years to 19.0% in those older than 80 years. It is estimated that ∼20 million Americans suffer from dry eye symptoms, 38 and upward of 40% of people experience symptoms at some point in their life. The symptoms of dry eye disease may include a sandy feeling, itching, burning, or stinging. Intermittent blurred vision can be physically debilitating. Dry eye can be caused by decreased tear production or by increased tear film evaporation. More recently, dry eye has been linked to inflammation. 39 A shorter-than-normal tear breakup time and poor quality tear film may account for intermittent blurred vision. 40 Certain systemic and topical medications, allergies, computer use, age, menopause, contact lens wear, as well as a history of refractive surgery are risk factors for dry eye. Treatment typically ranges from chronic daily artificial tear use to topical ocular anti-inflammatory and/or oral supplements that attempt to improve the tear film quality and quantity. Due to the chronic nature of this disease, it is conceivable that a sustained release delivery technology could benefit patients with dry eye and ocular surface disease.
Ocular allergic conjunctivitis
Ocular allergic conjunctivitis includes a number of different hypersensitivity disorders: seasonal and perennial allergic conjunctivitis, atopic keratoconjunctivitis vernal conjunctivitis, and giant papillary conjunctivitis. 41 The allergens that cause allergic conjunctivitis tend to differ by patient age and demographic region. 42 Ocular allergy affects 15%–20% of the population in developed nations. 43 The associated healthcare costs related to allergic conjunctivitis have been reported to be as high as $5.9 billion in the United States, with 25% (US$1.5 billion) of it related to medication use. 44 Treatment varies based on the subtype of allergic conjunctivitis and usually involves topical antihistamines, vasoconstrictors, nonsteroidal anti-inflammatory drugs (NSAIDs), mast cell stabilizers, corticosteroids, and/or cyclosporine. Topical and systemic medications as well as supratarsal injections of the anti-inflammatory drugs are methods of delivering the drugs. 43 Although topical therapy is often fast acting to relieve symptoms, the duration of action may only be 3–4 h.
Some drugs, like topical mast cell stabilizers, require a loading interval of several days to weeks before exposure to the allergic antigen, to have a maximum efficiency. The need for a regular dosing of 4 times a day over a period of weeks before exposure is an important factor to consider when assessing adherence and compliance. 43
Postoperative inflammation
Postoperative inflammation is an acute anterior segment disorder that occurs in varying degrees in patients who undergo cataract surgery or other types of ocular surgery. Although postoperative inflammation after surgery is usually manageable with topical anti-inflammatory drops, in some cases, it can be more severe, requiring extensive chronic and aggressive therapy 45 If the surgically induced inflammation is persistent, the risk of developing secondary ocular complications, such as iritis, glaucoma, posterior capsular fibrosis, intraocular adhesions, and swelling in the retina (cystoid macular edema), increases. If the inflammation is left untreated, it can interfere with the patient's visual rehabilitation.46–48 The incidence of chronic postoperative inflammation is about 0.02% after cataract surgery46,49 and is increased in patients with a prior retinal pathology, underlying diabetes, or a history of iritis/uveitis. The current standard of care involves a combination of corticosteroid and NSAID eye drops to be taken for days to weeks after surgery. This condition may be better treated with a drug delivery technology that gradually releases the drug over the postoperative period and has adequate intraocular penetration. 50
Glaucoma
Glaucoma is a slowly progressive optic neuropathy characterized by a loss of retinal ganglion cells and optic nerve axons. 51 According to the WHO, glaucoma is the second leading cause of blindness in the world, with close to 65 million suspected cases, accounting for 12% of all cases of preventable blindness in the world. 51 About 2% of the population between 40 and 50 years of age and 8% over the age of 70 years have elevated intraocular pressure (IOP), a leading risk factor. 52 The current treatments for glaucoma aim to reduce IOP, which if reduced have been shown to slow the visual field loss in large prospective clinical trials. 53 Direct annual costs of glaucoma in diagnosed American patients is estimated at $2.9 billion, with additional costs attributed to patients who are unaware that they have glaucoma. 54 Given the asymptomatic nature of this chronic progressive disease, compliance and adherence are poor. Topical regimens may present local tolerability issues as well as systemic adverse events. Studies have demonstrated that not only are patients unable to adequately administer their topical drops, many patients are noncompliant with adhering to continuous daily administration.55,56 Very often they fail to fully understand the nature of their disease, which increases the likelihood of missed drops and failure to refill prescriptions.40,57,58 Thus, an alternative sustained-release therapy that improves compliance and adherence would be very attractive and is an area of increased drug delivery interest.
Uveitis
Uveitis is caused by swelling and inflammation of the uveal tissues (ciliary body, iris, and choroid) from such factors as autoimmune disease, infections, toxicity, malignancy, and trauma. Anterior uveitis, also called acute iritis, can present in any age group and be associated with pain, photophobia, and a red eye secondary to anterior segment inflammation. The visual prognosis for patients with anterior uveitis is generally good; however, the prognosis does depend upon the underlying pathology and the chronicity of the inflammation. Posterior segment complications are more likely to occur if there is an associated underlying disease that results in chronic persistent and indolent inflammation.59,60 Given that this intraocular inflammation can be relapsing and remitting in nature, the requirement for long-term systemic and topical immune therapies presents problems with respect to chronic drug toxicity as well as compliance issues.
Unmet Needs
Compliance, adherence, and persistence
A leading opportunity for alternative sustained drug delivery platforms is to improve upon the issues of compliance and adherence. Patients do not often comply with daily regimens, and they especially do not continue on chronic medications in asymptomatic diseases like glaucoma. Pharmacy records indicate that close to 2 months can go by between refills, even for simple-to-use once-a-day prostaglandin analogs. 61 Various reasons for noncompliance may include cost, miscommunication, and/or difficulties around purchasing and/or actually getting the medication in the eye.
Data confirm that many patients are unable to self-administer drops effectively, including the arthritic aging population and uncooperative pediatric glaucoma patients. 62 Work conducted in glaucoma patients has supported that the chronicity of the treatment, the asymptomatic nature of the disease, and the complexity of their medical regimen make adherence a challenge. Patient questionnaires and videos have demonstrated the difficulty that patients have in administering their drops accurately and as prescribed. 63 Recent data revealed that only 71% of 204 glaucoma patients were able to get a drop into the eye, and only 39% did so without touching the bottle to the surface of the eye. 64 Such studies confirm eye drop wastage, potential contamination of the eye drop bottles, and poor understanding of the situation among these patients.
Suboptimal therapy
Without effective therapies being dosed as prescribed, ocular diseases, especially those that are chronic and indolent, progress and lead to visual deterioration and less than optimal outcomes. Without adequate IOP control, glaucoma will progress, increasing the cost to society and the burden of illness, which is already estimated at 2.9 billion per year. 54 Thus, an improved delivery technology would not only improve compliance and adherence but also potentially improve prognosis and patient outcomes, given that the drug is actually being delivered to the targeted tissue as prescribed. With a better targeted delivery, the inflammation, infection, and/or elevated IOP will be adequately managed, decreasing the burden of disease, alleviating office visits due to recurrences from under treatment and potentially decreasing surgical intervention, and improving the economic cost burden. With comparative effectiveness and outcomes being used to gauge government and third-party payer reimbursement, a more effective mode of delivering a therapy with better patient outcomes could be economically attractive from a payer perspective.
Improved safety-risk profile
A targeted therapy delivered directly to the intended ocular tissue at therapeutic concentrations has the potential to minimize off-target effects and improve the safety profile of ocular drugs. For example, systemically administered steroids given at doses necessary to treat eye disease can cause diabetes, osteoporosis, Cushing's disease, and immune suppression. Local topical and intravitreal doses of steroids can lead to cataracts and glaucoma. However, if highly localized and sustained ocular delivery of a steroid could be achieved without the systemic and local side effects, and patient compliance improved, then sustained-release therapy in the treatment of anterior and posterior uveitis would be attractive.
Even with topical glaucoma therapy, local and systemic side effects can occur, which limit compliance and interfere with an effective IOP management. 65 Topical beta-blockers, for example, have the potential to produce cardiac effects such as bradycardia and hypotension, as well as exacerbate asthma. 66 Prostaglandin analogs, despite their extremely favorable systemic safety, are limited by the locally associated side effects of periorbital darkening, iris hyperpigmentation, and associated dry eye.65,67 In fact, topical glaucoma medications have been shown to induce and/or worsen dry eye and ocular surface disease, thus bringing to the forefront the need for glaucoma medication delivery that is not topically administered in contact with the cornea and conjunctiva.68,69 The possibility exists that an IOP-lowering agent delivered subconjunctivally and/or directly to the ciliary body and/or TM that bypasses the ocular surface could allow for effective and more potent IOP lowering with improved ocular tolerability.
Treatment Modalities
Topical
Topically administered drugs are the current standard of care for most anterior segment diseases. These topical agents can be liquids, suspensions, gels, or ointments; each with benefits and drawbacks. Although topical delivery is the preferred local route of delivery to the eye, there are hurdles to efficient ocular penetration with conventional topical formulations. 70 In addition to the rapid tear clearance due to blinking, the excess volume of liquid in the ocular tear film results in increased flow to the nasolacrimal duct rapidly within seconds and consequent systemic absorption through the nasolacrimal mucosal membrane. 71 Thus, the dosage that actually penetrates into the eye is estimated to be only 1%–5% of the total dose administered. 7 Recent research in the topical delivery formulation has focused on new drug carriers with the potential to improve the ocular surface residence time, increase corneal penetration, and therefore improve the efficiency of topical ocular delivery. Some of these approaches include use of mucoadhesives, prodrugs, nanospheres, liposomes, and inclusion of permeability enhancers. 72 Prolongation of the drug contact time with the ocular surface can be achieved using ophthalmic ointments and other viscous vehicles that serve to enhance ocular bioavailability. 73
Prodrug formulations use pharmacologically inactive or less-active derivatives of drug molecules that are better able to penetrate the cornea (e.g., they are more lipophilic) than the standard formulation of the drug. During the course of penetrating the eye, the metabolite of the prodrug will be produced that ideally will have a greater potency, and/or more favorable therapeutic index than the prodrug. An example of such a successful prodrug strategy is latanoprost, which requires an esterase to hydrolyze the isopropyl ester from the prodrug to produce the active acid form to achieve greater potency and penetration. 74 In addition to improving penetration, prodrugs may also improve the therapeutic index by reducing the adverse events associated with drug exposure to the ocular surface, thus making this an attractive approach. 74
Permeability enhancers such as surfactants, bile acids, chelating agents, and preservatives, have all been used to increase ocular tissue penetration, chemical stability, and bioavailability, and to decrease local tolerability issues. 75
Cul-de-sac implants
The cul de sac of the eye is a pocket where palpebral and bulbar conjunctiva meet in either the lower or the upper eyelid. Devices that sit between the palpebral and the bulbar conjunctival surface, such as topical ophthalmic drug delivery device (TODDD™), Lacrisert® and Ocusert®, have been designed to improve anterior segment drug delivery. Because such devices are inserted into a potential space external to the eye, they are less invasive and therefore safer than intraocular implants. TODDD by Vista Scientific, LLC, has been developed to improve the efficiency of otherwise topically delivered glaucoma drugs (Fig. 3). It is a small self-administered thin plastic insert or concave conjunctival shell worn under the upper eyelid on the bulbar conjunctival surface and capable of sustained drug delivery over several months. 76 The drug of choice is polymerized into the plastic, and upon insertion, the drug diffuses across the conjunctiva and sclera without changing the shape of the device. 76 It is currently in preclinical studies.

The topical ophthalmic drug delivery device (photo courtesy of Amorphex Therapeutics) is a superior under the lid cul-de-sac drug delivery device to improve topical delivery.
Lacrisert (hydroxypropyl cellulose ophthalmic) inserts into the inferior cul-de sac. Lacrisert, although not a true drug delivery implant, does breakdown to cellulose, which helps to stabilize the tear film, prolong tear film breakup time, as well as lubricate and protect the eye. 77 Studies have shown that Lacrisert reduces the signs and symptoms resulting from moderate-to-severe dry eye syndromes, such as conjunctival hyperemia and corneal and conjunctival staining. 77 One potential drawback with Lacrisert, however, is that patients are required to insert the pellet into the cul de sac themselves and educating patients on how to use these devices can be difficult. Some of the adverse events that are associated with the use of the hydroxypropyl cellulose inserts are blurry vision, foreign body sensation, ocular irritation, hyperemia, hypersensitivity, photophobia, eyelid edema, and caking or drying of the viscous material on the eyelashes. 78
Ocusert is a similar drug-eluting nonbioerodible device developed for glaucoma that delivers either 20 or 40 μg/h of pilocarpine over a 7-day period. 65 The insert is formed by a film of ethylene–vinyl ester copolymer that is impermeable to the passage of external fluid. It should be noted that Ocusert is no longer marketed due to untoward effects of pilocarpine, such as a miosis and brow ache.
Another device in development for topical transconjunctival delivery is the Visulex-P. The device (resembling a scleral lens) rests on the bulbar conjunctiva. Aciont® is developing the Visulex-P-noninvasive ocular drug device, which is based on a comfortable, self-adhering eye applicator tailored for the delivery of small molecules, such as dexamethasone, to both the anterior and posterior segments of the eye. 79 It is currently in the preclinical development.
Punctal plugs
Punctal plugs have been used for decades for the treatment of the dry eye syndrome. For this indication of dry eye, the punctal plugs are tiny, biocompatible devices inserted into the punctum, that is, tear ducts, superior or inferior, to block tear drainage and improve tear film quantity and residual contact time. Recently, punctal plugs have been investigated as a drug delivery technology for use in the treatment of glaucoma. Punctal plugs have the advantage of being noninvasive and capable of providing controlled release of a topical drug to the ocular surface. Such punctal plugs can be made of degradable and nondegradable materials and molded in such manners that plug retention times can vary. Those made from silicone, hydroxyethyl methacrylate, and polycaprolactone are intended for a 180-day use (www.qltinc.com/newsCenter/2011/110829.htm) after which they need to be removed. Recently, punctal plugs were developed from a thermosensitive, hydrophobic acrylic polymer to avoid the problems associated with extrusion (Cylindrical Smartplug®). This polymer changes from a rigid solid to a soft, cohesive gel when its temperature changes from room temperature to body temperature. 80 Companies such as Vistakon (Jacksonville, FL) and Ocular Therapeutix (Bedford, MA) also have products in development to improve punctal plug retention and drug delivery efficacy.26,81
Generally, punctal plug drug delivery systems are coated with a material that is impermeable to the drug and tear fluid on all sides, except the head portion, through which the drug is released into the tear film. The release of the drug from a punctal plug is controlled by drug diffusion from the polymer with released drug coming into direct contact with the tear fluid. The drug can be formulated and delivered from the plug in the form of a solution, suspension, microemulsion, nanoparticles, microparticles, or liposomes to improve the drug retention time. Some punctual plugs can be soaked in the drug solution before insertion. 80
A common issue with punctual plugs is displacement from the punctum. QLT, Inc. and Vistakon Pharmaceuticals, LLC, have separately developed punctal plugs for latanoprost (L-PPDS) and bimatoprost, respectively. QLT, Inc. in 2009 reported a preliminary overall retention rate of 75% after 8 weeks of follow-up based on a baseline sample of 447 eyes from 239 subjects who were fitted with prototypes from one family of designs (www.qltinc.com/newsCenter/documents/090728_LPPDS_Release.pdf). The retention rate did not meet the Company's retention criteria, and the designs continue to be refined and evaluated. In 2011, QLT showed that 60% of subjects at 4 weeks had an IOP reduction with latanoprost-eluting plugs of 5 mm Hg or greater with a retention rate in the lower punctum of 95% (www.qltinc.com/newsCenter/2011/110829.htm).
Anterior chamber, subconjunctival, and episcleral implants
Implants located in the anterior chamber, subconjunctiva, and episclera can be utilized for anterior segment drug delivery. Subconjunctival/episcleral implants have the advantages of direct delivery of medication into the eye, fewer adverse events than systemic delivery, and better patient compliance than topical eye drops. They are usually inserted with a small incision in the conjunctiva and placed in direct contact with the sclera. Although the sclera shows permeation of molecules up to 120 kDa, 32 physiologic mechanisms such as the episcleral blood supply and lymphatics can potentially clear the drug that crosses the conjunctiva and therefore reduce the drug absorption.
Anterior chamber implants can be placed in the aqueous humor within the anterior chamber. One example of an anterior chamber insert is Surodex™. Surodex is a rod-shaped biodegradable poly(
LX201 (Lux Biosciences) is a silicone matrix episcleral implant designed to deliver cyclosporine A to the eye's surface for a full year. 26 Lux Biosciences completed the enrollment in a phase III trial to prevent corneal transplant rejection. The company is also developing bioerodible polymer implants for potential use in severe dry eye, macular degeneration, and diabetic macular edema. A subconjunctival insert (Latanoprost slow release insert) is currently in phase I/IIa for glaucoma. It is being developed by Pfizer, Inc. and pSivida at the University of Kentucky. The insert is composed of a PLGA tube containing a latanoprost core. 26 The first human study is designed to assess safety and efficacy in lowering intraocular pressure in patients with primary open-angle glaucoma and ocular hypertension. The insert is a bioerodible tube composed of PGLA with one end sealed and the other end having a rate-controlling membrane for drug diffusion. There are 2 tubes available with 2 different diffusion rates. The lower-dose tube releases the drug at the rate of 1 μg/day. The higher-dose tube releases the drug at the rate of 4 μg/day (NCT01180062).
Drug-eluting contact lenses
The concept of using contact lenses to deliver therapeutic agents was first explored more than 30 years ago. In 1974, Hillman reported treatment of 25 patients with acute glaucoma using pilocarpine-soaked contact lenses. 84 Reduction in IOP was documented over the course of a few hours, and when compared to historical control patients treated with intensive pilocarpine eye drops, the efficacy was equivalent. The investigators concluded that sustained delivery of drug from contact lens is less disruptive to patients than intense administration of eye drops during an acute attack of glaucoma, and it eliminated the need for constant nursing staff interventions.
Although pilocarpine is no longer the standard of care for glaucoma, the concepts presented by Hillman remain relevant to ocular drug delivery. More recent studies by other groups have explored the absorption and release kinetics of cromolyn sodium, ketotifen fumarate, ketorolac tromethamine, and dexamethasone sodium phosphate from contact lenses in vitro. 85 Similarly, Xu et al. examined the in vitro and in vivo release in rabbits for contact lenses presoaked with ketotifen fumarate. 86 He found the release profiles of the drug-soaked contact lens to be similar between the in vitro release behaviors and the in vivo characteristics in rabbit eyes. The contact lens showed an initial burst release with an achievement of a steady state characterized up to a maximum value (Cmax). A faster release was seen for more hydrophilic hydrogel backbones. Further, in comparison to topical drops in vivo, they found greater sustaining levels of ketotifen fumarate in the tear fluid for the contact lens group over 3 days. The authors conclude that as a result of the affinity for the drug, ketotifen fumarate, in the contact lens, the drug is able to maintain a relative more-stable drug concentration in the tear fluid. 75
Bucolo et al. studied the use of corneal shields made of HA to release methyl prednisone in the treatment of inflammation. They found that the corneal shields were able to maintain effective levels of methyl prednisone in the rabbit aqueous humor for up to 48 h. 87 Ultimately, the limitation with all of these presoaking strategies is that the absorption and release kinetics rely solely on the physicochemical properties of the drug itself and its equilibrium when in contact with the tear film. Consequently, this design does not result in release profiles lasting more than a few hours for most drugs and 24 h in the case of ketotifen.85,86
In contrast to the strategies that rely on soaking the contact lens with drug, more sophisticated fabrication techniques have been employed to incorporate various drugs directly into the contact lens material. For example, Gulsen and Chauhan described a novel drug-eluting contact lens device embedded with lidocaine-laden nanoparticles. 88 In this study, drug-release properties were measured in vitro over a 10-day period. Various combinations of the drug and excipients were tested, and all formulations resulted in a complete release over a 7-to-8-day period. The investigators from this study discuss selection of lidocaine as a model drug, owing to its hydrophobicity, and assert that this property is an important determinant of drug loading into the lens and kinetics of release in vitro. While lidocaine appears to be a suitable molecule for such experimental purposes, its potential for clinical use would be limited by the propensity for corneal toxicity and neurotrophic keratitis commonly associated with chronic anesthetic exposure.
Another contact lens delivery strategy reported by Ciolino et al. (Fig. 4) involves fabrication of a contact lens that contains an annulus of a drug-releasing polymer embedded within the device.89,90 This approach has been tested with an antifungal agent, econazole, and the antibiotic ciprofloxacin. The in vitro data suggest that zero-order drug release is achievable over a 30-day period. Other groups have investigated the use of the molecular imprinting technology to enhance the uptake of drugs into the contact lens matrix and achieve zero-order release of ketotifen for up to 7 days.91,92

Polymer drug-eluting contact lens (photo courtesy of Dr. Joseph Ciolino) achieved zero-order release kinetics in 30 days in vitro. Currently being studied for antimicrobial and glaucoma drug delivery to the anterior surface.
All of these contact lens-based release strategies offer a significant dosing advantage over existing daily eye drops. The ultimate challenge for these technologies will be to demonstrate a safety and/or efficacy benefit over the standard of care in relevant clinical indications, especially with a contact lens left in places for days to weeks. For example, incorporation of the antihistamine ketotifen into contact lenses may provide symptomatic relief to patients who wear contact lenses and suffer from ocular allergy. However, a chronic 24-h contact lens wear is associated with corneal toxicity 93 and any strategy that promotes increased exposure of the ocular surface to a noxious stimulus should be carefully considered.
In contrast to ocular allergy, sight-threatening diseases such as glaucoma may be better indications for a contact lens-based delivery system with IOP-lowering agents; however, the same issues and safety concerns still exist for a contact lens being left in place for weeks to months.
Drug-eluting intraocular lenses and capsule drug rings
Cataract surgery is the most common ambulatory procedure performed in the United States. Postoperative prophylaxis for infection and inflammation generally involves some combination of antibiotic, corticosteroid, and NSAID eye drops, and the exact regimen varies by region and the prescriber. 50 As an alternative to postoperative eye drops, strategies have been developed to incorporate drug release mechanisms directly into the intraocular lens (IOL) device for primarily the anti-inflammatory effects. Siqueira et al. reported development of a modified polymethyl methacrylate (PMMA) intraocular lens (IOL) containing a biodegradable dexamethasone tablet. 94 This device (Fig. 5) was implanted into the posterior chamber of New Zealand white rabbits, and dexamethasone was detected at therapeutic levels over a 9-day period. 94 Similarly, Eperon et al. demonstrated release of triamcinolone acetonide from bioerodible polymer rings that were attached to the IOL haptics. 95 Implantation of this device into rabbits resulted in the reduction of aqueous humor protein levels (an indicator of inflammation) and inflammatory cells up to 7 weeks after implantation. 95 A third strategy reported by Shukla et al. involved application of multilayer coatings to a conventional IOL device 96 ; however, it has not yet been tested in animal models. One benefit to this multilayer approach is the potential to incorporate side-by-side layers of anti-inflammatory and antibiotic medications seamlessly into the same device. However, although intraocular anti-inflammatory delivery may very well eliminate daily dosing, possible adverse events such as elevated IOP due to prolonged steroid exposure may become a tradeoff for the safety risk benefit. This will need to be evaluated as drug development moves forward for these devices.

Drug-eluting intraocular lens (photo courtesy of Dr. Siqueira) placed in posterior chamber of the eye.
IOL-related drug delivery systems offer the potential to reduce and simplify the postoperative eye drop regimens, which could directly benefit patients and healthcare payers. All of the above delivery strategies have their own relative merits and weaknesses owing to their unique designs. For example, the design by Siqueira et al. appears to deliver ample quantities of drug into the eye, but it requires a modified IOL 94 that may affect the cost of goods and surgical technique required for implantation. In contrast, the haptic ring-based delivery system by Eperon et al. can be used with any IOL that has sufficiently narrow haptics on which to thread the drug polymer rings. 95 Here too, the issue of the surgical technique arises in that attachment of drug rings to haptics may limit implantation via standard procedures. The drug-coating technique reported by Shukla et al., 96 however, seems adaptable to any IOL platform, and a modification of surgical technique would not be required. Nonetheless, the question arises whether such multilayer drug coatings are sufficiently flexible and durable to withstand the folding and friction experienced during insertion through a small corneal incision. There are clearly tradeoffs between these various IOL-based drug delivery strategies, and further studies are required to assess their practicality in human subjects.
The capsule drug ring (CDR) represents a novel drug delivery approach (Fig. 6). The nonbiodegradable CDR serves as a refillable reservoir in the lens capsule, capable of delivering multiple drugs to the anterior and posterior segment of the eye. After cataract surgery, there is an empty circumferential space around the intraocular lens, where the CDR is placed. Prototypes were manufactured using PMMA sheets as the reservoir material with a semipermeable membrane for controlled delivery and silicone check valves for refilling. 97 The semipermeable membrane could be placed facing the anterior or posterior segment of the eye depending on the targeted delivery site intended. The device has been studied in rabbits for posterior delivery using Avastin for the treatment of wet AMD and has shown near-zero-order release kinetics. 97
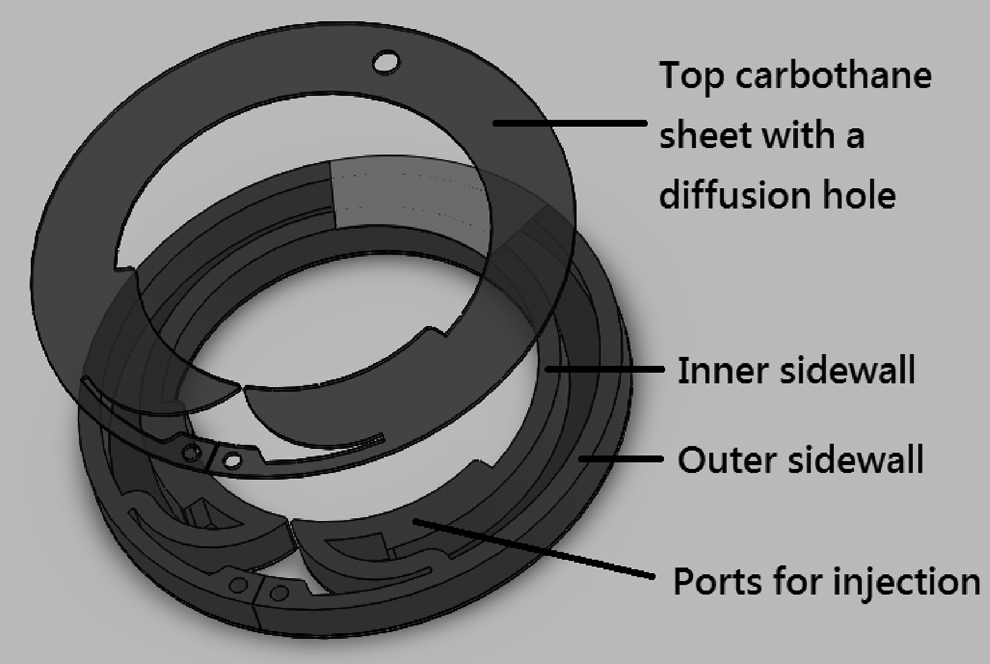
Illustration of the design of the capsule drug ring (CDR), a nonbiodegradable drug delivery device placed in the lens capsule bag around the IOL (photo courtesy of iVeena).
Microelectromechanical systems
The Microelectromechanical system (MEMS) system fabricated using MEMS engineering principles is a device/pump system that can be controlled either manually or electrically. 98 It consists of a reservoir connected to a cannula that is implanted in the subconjunctival space. The manually controlled pump includes a 1-way valve to control drug delivery. Once the drug is depleted, the reservoir can be refilled with the same or a different drug; multiple refills of the reservoir are possible, and the device can last implanted for several years. Drug is forced through the cannula as a result of hydrogen gas pressure that increases after electrolysis of water. Therefore, the rate of delivery through the cannula can be controlled by adjusting the applied current that causes the electrolysis of water. 98 Some concerns with these pumps are the development of infection during or after the surgical implant procedure. The proper placement of the tube in the anterior chamber is important to reduce any traumatic damage to the corneal endothelium, iris, papillary margin, or lens. MEMS prototypes developed by Replenish, Inc. (Pasadena, CA), using the ocular hypotensive agents 0.5% timolol or 0.004% travoprost, were implanted subconjunctivally in 2 dogs; the anterior cannula delivered the IOP-lowering agents directly into the eye.26,99 They have reported a preliminary preclinical reduction of IOP of 8-h duration and hope to extend the IOP lowering in the clinic to several months or years. 99 No complications were observed over 3 months. Although Replenish, Inc. plans to enter the trials for U.S. Food and Drug Administration approval in 2013 for a refillable and programmable pump, the final outcome is not predictable. The problem is that the commercial value for a drug delivery technology using an inexpensive generic hypotensive-lowering agent that is highly invasive and that has a higher risk to benefit profile over topical drops may meet challenges both in clinical development and in reimbursement. 99
Iontophoresis
The method of administering pharmacological agents by iontophoresis became popular at the beginning of 20th century due to the work of Leduc (1900), who introduced the term Iontotherapy. 100 Ocular iontophoresis was first investigated by the German scientist Wirtz 1908. 101 Iontophoresis is an active method of drug delivery that uses low levels of electrical current to enhance transport of drugs into and through body tissues. Iontophoresis enhances drug delivery by electrophoresis (direct electric field), electro-osmosis (convective solvent flow, i.e., liquid flow due to applied potential across a charged membrane), and electroporation (field-induced tissue alteration and pore induction). Iontophoresis has the advantage of being noninvasive and therefore avoids the risks associated with devices that require surgical implantation or intravitreal injections. An iontophoresis device has 2 electrodes: one is the donor electrode that holds the drug solution, and the other is the receiver electrode or return electrode that is placed at a point distal to the donor electrode to close the circuit.
There are the 2 routes of ocular iontophoretic drug delivery: transcorneal and trans-scleral. Transcorneal iontophoresis involves delivering a relatively high concentration of a drug to the anterior segment of the eye with the potential of treating anterior segment diseases such as keratitis, dry eyes, corneal ulcers, and ocular inflammation. 102 After transcorneal iontophoresis, the drug cannot easily reach the posterior segment of the eye due to the lens barrier. Trans-scleral iontophoresis may avoid this barrier (lens–iris diaphragm) and may deliver drugs directly into the posterior segment. Iontophoretic delivery was found to be principally dependent on the charge of drug, position of the electrode placement, duration of application, and current intensity.11,103
There have been 2 approaches for containing the drug formulation in the iontophoretic device. The first is basically an eyecup holding the drug solution, while the second approach is to use a drug-saturated gel as the delivery probe. The Eyegate® device, EyeGate II Delivery System (Fig. 7), has an annular shape with the diameter of the proximal part being lightly larger than that of the limbus, while the distal part covers 2 mm of the anterior sclera. 104 The clinical trials have been in dry eye, scleritis, and anterior uveitis. Recently, in the anterior uveitis study, two-thirds of the patients reached an anterior chamber cell score of zero with a single treatment of EGP-437 (dexamethasone phosphate) via the EyeGate II Delivery system, especially with a lower iontophoretic dose (mA-min). 105 Furthermore, minimal IOP elevation was associated with this mode of steroid delivery. 105 Vollmer and Parkinson et al. 106 used a custom-manufactured OcuPhor™ hydrogel (Iomed, Inc., Salt Lake City, Utah) composed of a polyacetal sponge that allowed for a soft flexible electrode to be placed in the inferior cul de sac. However, there are no recent ocular iontophoresis data from Iomed, Inc. Aciont is developing the Visulex-I-noninvasive ocular drug device, which is based on a comfortable, self-adhering eye applicator (resembling a scleral lens) tailored for the transcleral delivery of anti-VEGF macromolecules of up to 150 kDa to the posterior segment of the eye through iontophoresis. 107
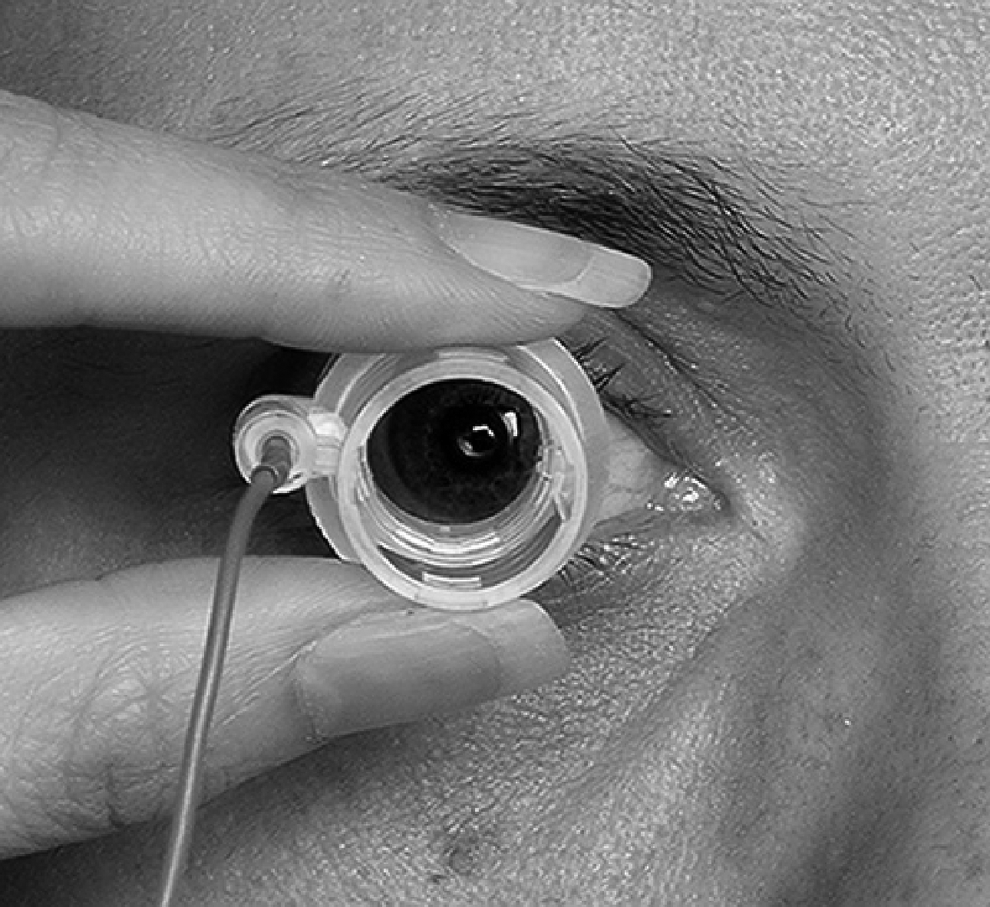
EyeGate® II Delivery System, a transscleral annular iontophoresis device currently in the clinic for uveitis and dry eye (photo courtesy of EyeGate Pharmaceuticals).
Ocular iontophoresis has effectively delivered small molecules such as dexamethasone in patients 105 and macromolecules such as Galbumin, bevacizumab, and FITC dextrans108–110 in vitro. It has been evaluated for potential gene therapy for human eye diseases, treatment of fungal keratitis, DNA delivery, and many other ocular applications.111,112
Commercialization of Drug Delivery Technology
Successful commercialization of new medical technology involves a combination of factors intrinsic and extrinsic to the invention itself. Intrinsic factors relate to the aspects of its design and material composition, such as the chemical properties of a new drug or ergonomic design of a new instrument. Extrinsic factors that affect the success of the new technology include (1) technology transfer from academia into industry; (2) capital to support further research and development; (3) regulatory guidance about the requirements governing the clinical development and the eventual approval; (4) decisions by healthcare payers about pricing and reimbursement; (5) clinical training and dissemination of knowledge regarding the new technology; and (6) the existence of competing products in the marketplace and the unmet need. A comprehensive discussion of these factors is beyond the scope of this review, and other recent articles provide in-depth discussion of these topics.113–118
When considering the potential impact of the new drug delivery technology for ophthalmology, it is important to evaluate how each of these factors may influence the commercial success of the proposed product, since commercial viability will extend beyond meeting just the regulatory approval hurdles. In summary, successful formulation for drug delivery to the anterior segment requires the following:
(a) Delivering efficacious drug concentrations to local ocular tissue targets (b) Developing and manufacturing delivery systems/new drugs that fulfill point (a) (c) Acquiring knowledge of global regulatory requirements (d) Conducting clinical trials that fulfill the regulatory requirements and meet both safety and efficacy endpoints (e) Understanding the unmet needs, the economic costs, the commercial landscape, and the reimbursement arguments, and evaluating the outcomes to patients that will allow these products to get into the market.
Summary
To maximize the efficacy and safety of these novel treatments summarized in Table 1, much of the research will be focused on achieving effective therapies for ocular diseases in a more cost-effective and therapeutically attractive manner. Whether ocular implants are placed in the cul de sac, subconjunctiva, episclera, within the anterior segment, and or in the capsule bag, the sustained release technology will continue to be of interest to pharmaceutical scientists; that is, in the segments, although they may require invasive techniques, implants bypass the physiological (clearance) and anatomical barriers to delivering constant therapeutic levels of drug directly to the site of action; the advantage is that smaller doses are needed during treatment. Novel biodegradable and nonbiodegradable implants achieved by varying the polymer composition and sphere size (e.g., nanosphere or microsphere) ocular drug delivery formulations are capable of enhancing the drug cellular penetration, protecting against degradation, and allowing long-term delivery. 119 Another area that will be thoroughly researched in the next 5 years will be developing successful translational animal models for various anterior and posterior diseases. Animal models provide us with the methods to develop the pharmacology of a new therapeutic agent; however, translational models are often limited. 120
CDR, capsule drug ring; MEMS, microelectromechanical systems.
Footnotes
Author Disclosure Statement
Dr. Molokhia is a consultant with Aciont and iVeena. Dr. Mandell is a nonpaid consultant to MIT and is an inventor on a patent filed by MIT. Dr. Wirostko is a consultant with SKS ocular, Merck and iVeena and cofounder of Jade Therapeutics, LLC, a company working on sustained delivery. In 2010, Dr. Wirostko served as the glaucoma team lead on the sPivida-Pfizer Xalatan SR device program. She holds stock in Pfizer. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. Myles Jaffe, Ph.D. provided writing assistance in the production of this manuscript.