
Abstract
Abstract
Purpose:
To investigate the effect of diquafosol tetrasodium on tear and visual function in short break-up time (sBUT) dry eye (DE).
Methods:
This interventional nonrandomized comparative study involved 11 eyes in 11 patients with sBUT DE (symptom-positive sBUT group) and 13 eyes in 13 volunteers with BUT values≤5 s without DE symptoms (symptom-negative sBUT group). Tear function was assessed by measuring BUT and Schirmer values. Serial measurements were made of visual acuities (using a functional visual acuity measurement system) and higher-order aberrations (using a wavefront sensor). The parameters were compared before and 1 month after diquafosol tetrasodium instillation. Any changes in symptomatology after administration were also recorded.
Results:
After diquafosol tetrasodium administration, BUT values tended to increase in the symptom-positive sBUT group (P=0.07) and significantly increased in the symptom-negative sBUT group (P<0.05). LogMAR functional, minimal, and maximal visual acuities and higher-order aberrations significantly decreased after diquafosol tetrasodium administration in the symptom-positive sBUT group (P<0.05), while there were no significant changes in these values in the symptom-negative sBUT group (P>0.05). Diquafosol tetrasodium administration provided relief of DE symptoms in 75% of patients in the symptom-positive sBUT group.
Conclusions:
Diquafosol tetrasodium appeared to improve tear film stability and visual function in sBUT DE.
Introduction
Increasing attention has been directed toward mucins as the foundation of a stable tear film; indeed, mucins play an important role in the maintenance of an optimal tear film over the ocular surface. 1 The mucins on the ocular surface comprise secretory mucins and transmembrane mucins. 2 One of the former, MUC5AC, is a gel-forming polymetric glycoprotein biosynthesized in goblet cells, and stored in them, in the conjunctival epithelium, and it aids tear retention in cooperation with transmembrane mucins. 3 The mucins identified as transmembrane mucins on the ocular surface are typified by MUC1, MUC4, and MUC16, which are produced by the corneal and conjunctival epithelia. 4 These 3 transmembrane mucins, which are similar in structure, and aid water retention with their hydrophilic sugar chain, help to prevent adhesion between the palpebral conjunctiva and corneal epithelium, and aid phylaxis by forming a glycocalyx barrier with the secretory mucins. Watanabe et al. reported that the secretory mucins are necessary for the spreading and retention of water on the ocular surface. 1 The expression of mucin is altered in squamous metaplasia and DE conditions,5–7 and this alteration may reduce the surface tension of the aqueous layer on the ocular surface and cause instability of the tear film. Disruption of the mucin layer may lead to DEs with instability of the tear film.
Short break-up time (sBUT) DE, which may be associated with decreased goblet cell density, has been reported to be associated with little or no corneal epithelial damage, but to be strongly symptomatic.8,9 DE symptoms may present as eye fatigue, discomfort, or heaviness, but also as visual blur or discomfort during daily activities despite a normal tear volume and absence of corneal staining. Recent studies have revealed visual deterioration in DEs,10–15 and it is thought that the stability and regularity of the ocular surface are the major factors in the formation of clear visual images.16–24 Dynamic changes in the tear film have received attention as the possible cause of such visual deterioration. The surface regularity index and surface asymmetry index—as measured by corneal topography and by wavefront and tear stability analysis systems—have been shown to be significantly worse in patients with DEs than in normal subjects.25–29 Functional visual acuity measurement has also been reported to be useful in the assessment of visual quality in DE patients.27,30–35 Functional visual acuity has been suggested to reflect an individual's performance in relation to certain daily activities involving visual tasks, detecting masked impairment of visual function due to ocular surface tear conditions in DE patients who complain of decreased visual acuity despite normal conventional visual acuity. The FVA measurement system is a device to measure changes in continuous visual acuity over time.
The induction of mucin production from the ocular surface may increase the stability of the tear film, and diquafosol tetrasodium, a P2Y2 receptor agonist, has been shown to have a stimulatory effect on tear and MUC5AC secretion by the conjunctiva in both rat and rabbit.36,37 It also stimulates the gene expression of transmembrane mucins in human corneal epithelial cells. 38 We hypothesized that administration of diquafosol tetrasodium might increase not only the stability of the tear film, but also visual performance, in sBUT DE. To test this hypothesis, we investigated its effects on tear function and optical quality by means of a wavefront aberration analyzer, and its effects on visual performance by means of functional visual acuity measurements.
Methods
Patients
Eleven patients (3 males, 8 females; mean age: 49.3±6.6 years; range: 41 to 61 years) with sBUT DE at Wada Eye Clinic were enrolled in this study. In each patient, the right eye was studied. The sBUT DE was diagnosed by the presence of DE symptoms of dryness, foreign body sensation, eye pain, photophobia and blurred vision, and a BUT value of less than 5 s with no positive fluorescein staining scores (symptom-positive sBUT group). Fluorescein stain scoring of the ocular surface was based on the Japanese DE diagnostic criteria. 39 Thirteen right eyes in 13 volunteers (8 males, 5 females; mean age: 49.2±7.2 years; range: 35 to 59 years) with BUT values≤5 s without DE symptoms, who came to Wada Eye Clinic for the prescription of glasses or routine ophthalmic examination, served as controls (symptom-negative sBUT group). Exclusion criteria for subjects in both symptom-positive and negative sBUT groups included the presence of ocular trauma, blepharitis, ocular allergy, meibomian gland disease, abnormality of the nasolacrimal drainage apparatus, permanent occlusion of lacrimal puncta or temporary punctal plug occlusion, and contact lens wearing. Absence of lid-related diseases was based on absent hyperemia at lid margin, regular lid margin, and normal oily expressible secretion at the center of the upper lid. The 3% diquafosol tetrasodium instillation (Santen Pharmaceutical Co., Ltd) was carried out 6 times a day for 1 month in the symptom-positive and symptom-negative sBUT groups. Only diquafosol tetrasodium administration 6 times a day was implemented. No other concurrent lubricant was additionally used.
The study followed the Tenets of the Declaration of Helsinki. Informed consent was obtained from each patient to participate in the current study. An ethics board approval was obtained from Ryougoku Eye Clinic for the examination procedures and the study protocol.
Tear function evaluation
The Schirmer test was performed without topical anesthesia. A standardized strip of filter paper (Showa Yakuhin) was placed in the lateral canthus away from the cornea and left in place for 5 min with the eye closed. Readings were reported in millimeters of wetting per 5 min.
Standard BUT measurement was performed after instillation of a 1-μL volume of a preservative-free solution of 1% fluorescein into the conjunctival sac by means of a micropipette. The patient was then instructed to blink several times for a few seconds to ensure adequate mixing of the dye. The interval between the last complete blink and the appearance of the first corneal black spot in the stained tear film was measured 3 times, and the mean value of the measurements was calculated. A BUT value≤5 s was considered abnormal. A cobalt blue filter was used to measure the BUT values.
Tear function examinations were performed in the symptom-positive and symptom-negative sBUT groups before the administration and after 1 month of treatment. The interval from the last diquafosol drop was longer than 30 min at the examinations after 1 month of treatment.
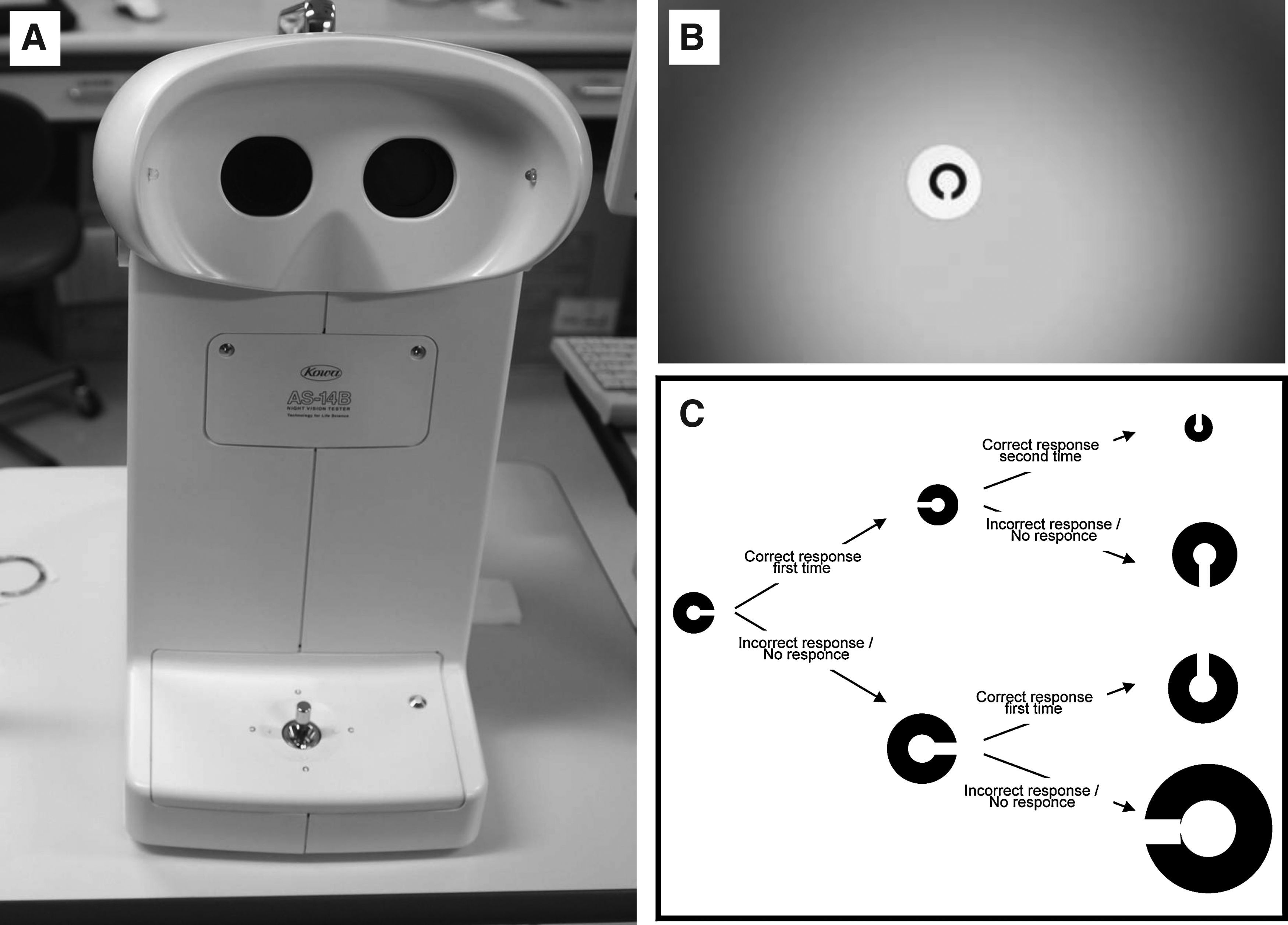
Functional visual acuity measurement system
A functional visual acuity measurement system (Kowa) was used to examine the changes with time in the continuous visual acuity (Fig. 1A).32–35 The Landolt optotypes are presented on the monitor of the equipment (Fig. 1B), and their sizes change depending on the correctness of the responses. In brief, the optotypes are displayed automatically, starting with smaller ones. When the response is correct, even smaller optotypes are presented. If the responses are incorrect, larger optotypes are presented automatically (Fig. 1C). Visual acuity is continuously measured from the baseline best corrected Landolt visual acuity. The functional visual acuity measurement system can measure visual acuity from 150/100 to 20/200. When there was no response within the set display time, the answer was assumed to be an error, and the optotype enlarged automatically.
Functional visual acuity measurement system.
The outcomes were recorded as starting visual acuity, logMAR functional visual acuity, visual maintenance ratio, and maximal and minimal visual acuities. Starting visual acuity was defined as the baseline visual acuity, which is the value of the standard best corrected visual acuity measured by the functional visual acuity measurement system. Functional visual acuity was defined as the mean value of time wise change of the visual acuity during the overall examination, not the value at one time-point during the examination. The visual maintenance ratio is the ratio of functional VA divided by the value of baseline VA.34,40 In brief, the visual maintenance ratio was calculated as follows: visual maintenance ratio=(lowest logMAR visual acuity score – functional visual acuity at 60 s)/(lowest logMAR visual acuity score – baseline visual acuity). The maximal and minimal visual acuities were defined as the highest and lowest visual acuities recorded during the examination. 41
Functional visual acuity was measured during a 60-s period without instillation of topical anesthesia. Subjects were instructed to be allowed to blink naturally during the measurement period. Patients delineated the orientation of the automatically presented Landolt rings by manipulation of the joystick. Functional visual acuity testing was carried out after tear function testing.
Functional visual acuity measurements were performed in the symptom-positive and symptom-negative sBUT groups before the administration and after 1 month of treatment. The interval from the last diquafosol drop was longer than 30 min at the examinations after 1 month of treatment. One expert examiner examined the functional visual acuity measurement test under the blindness as to which patients were control or not.
Sequential measurement of wavefront aberrations
Serial measurements of ocular higher-order aberrations were performed by means of Hartmann-Shack wavefront aberrometer (Topcon Corp.). Higher-order aberrations were measured during a blink-free 10-s period without instillation of topical anesthesia. The higher-order aberration data were analyzed quantitatively for the central 4-mm-diameter zone up to the fourth order by expanding the set of Zernike polynomials. From the Zernike coefficients, the root mean square (RMS) was calculated to represent the wavefront aberrations. S3 and S4 are the RMS of the third-order and fourth-order Zernike coefficients, respectively. Coma-like aberrations (S3), spherical-like aberrations (S4), and total higher-order aberrations (S3+S4) were calculated.
Higher-order aberrations were measured in the symptom-positive and symptom-negative sBUT groups before the administration and after 1 month of treatment. The interval from the last diquafosol drop was longer than 30 min at the examinations after 1 month of treatment. The same examiner as the functional visual acuity testing measured the higher-order aberrations under the blindness as to which patients were control or not.
Questionnaire concerning DE symptoms
A VAS scale was used for the assessment of symptomatic improvement after diquafosol tetrasodium administration in the symptom-positive sBUT group. The 0 point referred no improvement whereas 100 points referred to complete symptomatic improvement.
Statistical analysis
Data were reported as mean±SD. The pretreatment values obtained for tear function, functional visual acuity, and wavefront aberration in the symptom-positive and symptom-negative sBUT groups were analyzed by Student t-test. A paired t-test was performed for the comparison of tear functions, functional visual acuity, and wavefront aberration parameters after and before the administration of diquafosol tetrasodium.
SPSS software version 12.0J for Windows (SPSS, Inc.) was used as the statistical analysis software. A P value of less than 5% was considered statistically significant.
Results
Tear function assessments
The pretreatment tear functions of the symptom-positive and symptom-negative sBUT groups are shown in Table 1. There were no significant differences in both the BUT and Schirmer values in the symptom-positive and symptom-negative sBUT groups (P>0.05).
Student t-test aP<0.01 between the symptom-positive and symptom-negative groups.
BUT, tear film break-up time; sBUT, short tear film break-up time.
Figure 2 shows the mean BUT and Schirmer values before and 1 month after administration of diquafosol tetrasodium in the symptom-positive and symptom-negative sBUT groups. The BUT values were significantly increased in the symptom-negative sBUT group after the administration (P<0.05). The BUT values showed a nonsignificant increase tendency in the symptom-positive sBUT group with (P=0.07). The Schirmer values showed no significant differences with diquafosol tetrasodium.
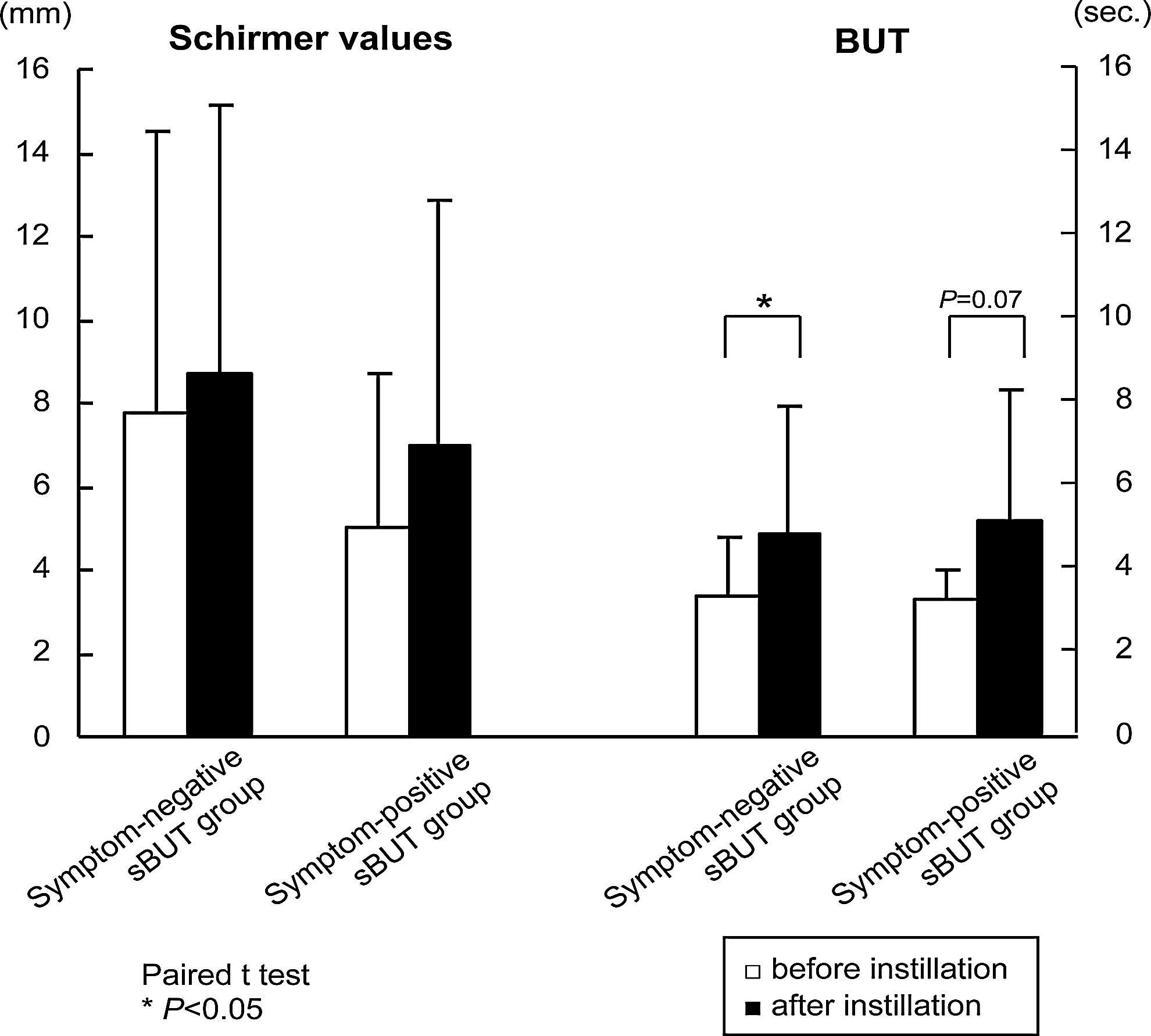
Tear function parameters before and after instillation of diquafosol teterasodium. The BUT values were significantly increased in the symptom-negative short break-up time (sBUT) group after the administration (P<0.05). The BUT values showed a nonsignificant increase tendency in the symptom-positive sBUT group with (P=0.07).
Functional visual acuity parameters
Table 1 shows the mean pretreatment values for starting visual acuity, functional visual acuity, visual maintenance ratio, and maximal and minimal visual acuities for each group. The mean logMAR starting visual acuity values for the symptom-positive and symptom-negative sBUT were 0.02±0.09 and 0.02±0.13, respectively (no significant differences between the groups; P>0.05). No significant differences were observed in functional visual acuity parameters in the symptom-positive and symptom-negative sBUT groups (P>0.05).
Figure 3 shows data for the mean starting visual acuity, functional visual acuity, visual maintenance ratio, and maximal and minimal visual acuities in the symptom-positive and symptom-negative sBUT groups before and after the administration of diquafosol tetrasodium. The mean logMAR starting visual acuity values obtained before and after the administration were 0.02±0.09 and 0.02±0.06 in the symptom-positive sBUT group, and 0.02±0.13 and 0.02±0.13 in the symptom-negative sBUT group, respectively (no significant difference within either group; P>0.05). The mean logMAR functional visual acuity values before and after the administration were 0.22±0.25 and 0.14±0.24 (significantly different, P<0.05) in the symptom-positive sBUT group, and 0.15±0.23 and 0.13±0.20 (not significantly different, P>0.05) in the symptom-negative sBUT group, respectively. The mean visual maintenance ratio values before and after the administration were 0.90±0.14 and 0.96±0.08 in the symptom-positive sBUT group, and 0.97±0.07 and 0.97±0.05 in the symptom-negative sBUT group, respectively. The visual maintenance ratio value obtained after the administration tended to be higher than that obtained before in the symptom-positive sBUT group (P=0.07). The mean logMAR maximal visual acuity values before and after the administration were 0.06±0.20 and −0.02±0.16 in the symptom-positive sBUT group and −0.01±0.19 and −0.13±0.32 in the symptom-negative sBUT group, respectively. The mean minimal visual acuity values before and after the administration were 0.43±0.36 and 0.37±0.39 in the symptom-positive sBUT group, and 0.34±0.33 and 0.31±0.31 in the symptom-negative sBUT group, respectively. Both the mean logMAR maximal and minimal visual acuity values after the administration were significantly lower than those obtained before in the symptom-positive sBUT group (P<0.05). The mean numbers of blinks before and after the administration were 13.0±9.4 and 17.2±10.2 in the symptom-positive sBUT group, and 6.8±5.2 and 9.1±7.7 in the symptom-negative sBUT group, respectively. No significant differences were observed before and after the administration in both groups (P>0.05). Figure 4 shows the sequential changes in visual acuity values during the measurement period in a representative case which showed a clear improvement after diquafosol tetrasodium instillation.

Functional visual acuity parameters before and after instillation of diquafosol tetrasodium. Functional, maximal, and minimal visual acuities significantly improved after the administration of diquafosol tetrasodium in the symptom-positive sBUT group (*P<0.05).

Representative case: color-coded maps showing total aberration and sequential changes in visual acuities before and after instillation of diquafosol tetrasodium. A 44-year-old man's color-coded map of higher-order aberrations (root mean square [RMS; μm]; 4.0 mm pupil) (left column) and sequential changes in visual acuities (right column). Changes in the map before (above) and after (below) diquafosol tetrasodium instillation reveal reduction in higher-order aberrations and improvements in visual acuities. Green line: functional visual acuity score. Blue line: starting visual acuity score. Red line: visual acuity change with time.
Ocular higher-order aberration parameters
Table 1 shows the mean pretreatment values obtained for coma-like aberration, spherical-like aberration, and total higher-order aberrations. Significant differences were observed in spherical-like aberration and total higher-order aberrations in the symptom-positive and symptom-negative sBUT groups (P<0.05).
Figure 5 shows the mean values for coma-like aberration, spherical-like aberration, and total higher-order aberrations in the symptom-positive and symptom-negative sBUT groups before and after diquafosol tetrasodium. The mean coma-like aberrations before and after the administration were 0.105±0.005 and 0.099±0.004 in the symptom-positive sBUT group, and 0.100±0.007 and 0.094±0.006 in the symptom-negative sBUT group, respectively. The corresponding values for spherical-like aberrations were 0.088±0.005 and 0.074±0.002 in the symptom-positive sBUT group, and 0.070±0.010 and 0.062±0.004 in the symptom-negative sBUT group. The corresponding total higher-order aberrations were 0.132±0.005 and 0.127±0.003 in the symptom-positive sBUT group, and 0.119±0.008 and 0.122±0.005 in the symptom-negative sBUT group. The mean values for coma-like, spherical-like aberrations and total higher-order aberrations were significantly lower after the administration in the symptom-positive sBUT group (P<0.05, P<0.01, P<0.05, respectively). Figure 4 shows color-coded maps of the total high-order aberration across a 4.0-mm pupil in a representative case, which showed a clear improvement in the high-order aberration map after diquafosol tetrasodium instillation.

Higher-order aberrations before and after instillation of diquafosol tetrasodium. Coma-like and spherical-like aberrations improved after administration of diquafosol tetrasodium in the symptom-positive sBUT group (*P<0.05 and **P<0.01, respectively).
Symptomatic changes
The mean VAS scale improvement was 35.8±19.4 points. The diquafosol tetrasodium instillation provided symptomatic DE relief in 75% of the patients in the symptom-positive sBUT group. None of the patients in the symptom-positive sBUT group and subjects in the symptom-negative sBUT group complained of any adverse events of diqufosol teterasodium solution in this study.
Discussion
Diquafosol tetrasodium, a P2Y2 receptor agonist, is a new preparation of eye drops that stimulates tear and mucin secretion, which improves tear film stability.36–38,42,43 However, a PubMed search revealed no clinical report of effects of diquafosol tetrasodium on the visual function in DEs. We, therefore, conducted this study to assess whether diquafosol tetrasodium has beneficial effects on tear film stability and/or optical quality (using the wavefront aberrometer) and on visual performance (by using the functional visual acuity measurement system) in sBUT DE. Some reports suggest that sBUT DE represents an early milder form of DE.44–46 However, we experience the necessity of DE treatments in sBUT DE patients with strong DE symptoms. It seems that sBUT DE patients tend to increase recently in office workers with video display terminal work and contact lens users. We investigated the effect of cumulative dosing of diquafosol tetrasodium over a month on the ocular surface in DEs.
The presence of DE with epithelial damage in the central optical zone of the cornea is an important causal factor for impaired visual performance. 34 The present study suggests that not only epithelial damage, but also decreased tear film stability leads to visual deterioration. In a previous study, we suggested that functional visual acuity was decreased in sBUT DE, and that it improved following treatment by punctal plug insertion.33,47 We also previously reported that functional visual acuity correlated significantly not only with the ocular surface vital staining scores, but also with tear stability. 33 A positive correlation between tear stability and functional visual acuity suggests poor visual performance in sBUT DE despite no or minimal epithelial damage. 34 The absence of a stable tear film between blinks may result in reduction of optical quality. These patients show evidence of instability of the tear film without corneal staining, which suggests that instability of the tear film without a breakdown in the corneal epithelium is responsible for the visual degradation seen.
In this study, we also examined eyes that had sBUT values but no DE symptoms. We found that their pretreatment functional visual acuity parameters in the symptom-positive sBUT group were not significantly different (P>0.05), while spherical and total higher-order aberrations showed significantly lower compared to the symptom-positive group (P<0.01). Since the functional visual acuity measurement was performed under natural blinking, frequent blinking might have normalized the tear film, so that the significant differences of visual performance were not observed between both groups. On the other hand, dryness induced by blink suppression during the wavefront aberration measurement might directly affect the values obtained for optical quality. The time to first tear breakup is one parameter of tear film instability, but there are frequently variations in the location of first breakup or the extent of breakup. Higher Schirmer values in the symptom-negative sBUT group may play a role to maintain the tear stability at the optical area on the ocular surface. The breakup pattern and speed of tear film might be different between the symptom-positive and symptom-negative sBUT groups, which may contribute the better optical quality even under the blink suppression in the symptom-negative sBUT group. In our observations, more patients with symptom-positive sBUT DE disease have lower corneal break up patterns, which can also explain the differences in higher order aberrations.
Concerning the effects of diquafosol tetrasodium on tear functions, the BUT values tended to be increased after its administration in the symptom-positive sBUT group and were significantly increased in the symptom-negative sBUT group. This difference between the symptom-positive and symptom-negative sBUT groups may reflect the severity of tear dysfunctions in those groups. Since diquafosol tetrasodium was able to improve BUT values, it is possible that administration of this agent might help prevent DEs by maintaining a healthy tear film. Nilfoforoushan et al. investigated the effect of preservative free artificial tear on visual acuity in symptomatic and asymptomatic DEs, and found the temporal improvement in vision in both groups. 48 They suggested that both symptomatic and asymptomatic DE patients have some element of dryness but these changes were enough to cause symptoms only in symptomatic DE patients. We propose a hypothesis that the eye with the sBUT values but no DE symptoms is a preparative stage of DE with milder destruction of goblet cells. In the preparative stage of DE, diquafosol tetrasodium instillation may promote mucin secretion, which works on the construction of healthy tear film in 1 month. Therefore, the symptom-negative sBUT group had better improvement in BUT values than the symptom-positive sBUT group. On the other hand, it must be conceded that instillation for 1 month may not have been long enough to effect a consistent improvement in tear stability in sBUT DE. Therefore, further research on the effects of longer administrations of diquafosol tetrasodium on tear function parameters in DEs may be necessary, although we should point out that a 1-month administration provided symptomatic relief. In this study, no adverse events of diquafosol tetrasodium solution were observed. However, we sometimes experience the patients' complaints of the production of debris and smarting pain due to the instillation.
Here, we found that visual function was significantly improved after administration of diquafosol tetrasodium in the symptom-positive sBUT group, as detected by improvements in functional, minimal, and maximal visual acuities, and in coma-like and spherical-like aberrations. On the other hand, no such significant changes in visual function were observed in the symptom-negative sBUT group. After administration of diquafosol tetrasodium, optical quality would be expected to improve due to improved optical regularities in synchrony with the increased BUT values in both the symptom-positive and symptom-negative sBUT groups. Both optical quality and visual function improved only in the symptom-positive sBUT group. These differences between the groups may be related to the difference of severity of the visual deterioration in the pretreatment state. We presume that the deteriorated visual function improved following administration of diquafosol tetrasodium due to the better quality of the tear film in the symptom-positive sBUT group.
Concerning the blink number during the functional VA measurement, we obtained the outcomes contrary to our expectations that the blink numbers tended to increase regardless the better tear film stability after the administration in both symptom-positive and negative sBUT group. We focused attention on debris, which is one of the side effects of diquafosol teterasodium instillation. We sometimes experience that patients' complain of debris after the instillation of diquafosol teterasodium. We presume that the increase of mucin alone may not work to spread tears regularly and extensively over cornea when tear volume is insufficient. Debris, which may be produced by the excessive mucin, possibly causes nerve stimulation and induces blinks. Accordingly, aqueous instillation may be necessary in order to demonstrate and supply an additional benefit of diquafosol teterasodium instillation in DE patients with low tear volume. Further histogenetical studies may be required to make sure if debris is produced by the excessive secretion of mucin.
In conclusion, we found that diquafosol tetrasodium instillation was effective for the improvement of visual function in sBUT DE. Diquafosol tetrasodium may work by improving tear stability and optical quality. Diquafosol tetrasodium has the potential to be an effective drug targeting tear and mucin secretion that may allow a healthy tear film to be constructed on the ocular surface. Further research will be required to investigate the effect of longer administrations of this drug on optical quality and tear stability.
Authors' Contributions
Conception of design (M.K., M.D., K.T.); analysis and interpretation (M.K., M.D.); writing the article (M.K.); critical revision of the article (M.D., K.T.); final approval of the article (M.K., M.U., T.K., M.D., K.T.); data collection (M.K.); provision of materials, patients, or resources (M.K., M.U., T.K.); statistical expertise (M.K.); obtaining funding (M.K.); literature search (M.K.); and administrative technical, or logistic support (M.D., K.T.).
Footnotes
Author Disclosure Statement
Santen Pharmaceutical Co., Ltd., was not involved with the scientific content of the research projects or the writing of the article. K.T. indicates travel support paid to him and research support paid to the university in the form of a grant from Santen Pharmaceutical Co., Ltd. K. T. and M. K. hold patent rights for the methodology and apparatus for the measurement of functional visual acuity (US patent no: 7470026). Other authors have no financial interest related to this article.