
Abstract
Abstract
Purpose:
To assess whether dorzolamide 2%–timolol 0.5% (D/T) and/or brimonidine 0.2%–timolol 0.5% (B/T) alters retinal vascular autoregulation (RVA) and seated ocular perfusion pressure (sOPP) in primary open angle glaucoma (POAG) patients who demonstrate retinal vascular dysregulation (RVD) on timolol 0.5% alone.
Methods:
In this prospective, observer-masked, crossover study, 21 POAG patients with untreated intraocular pressure (IOP) >21 mmHg were treated for 6 weeks with timolol 0.5%. Subsequently, we measured inferior temporal retinal artery blood flow in the left eye with subjects seated and then while reclined for 30 min using the Canon Laser Blood Flowmeter. Subjects with a change in retinal blood flow in response to posture change outside of the range previously found in healthy subjects were designated as having RVD and randomized to either D/T or B/T for 6 weeks and re-tested. This was followed by treatment with the opposite medication.
Results:
Seven of the 21 subjects demonstrated RVD in response to posture change following timolol 0.5%. Multiple linear regression analysis indicated that lower sOPP was the main determinant of RVD (P=0.033). After treatment with D/T, all 7 converted from RVD to normal RVA status (P=0.001). Four of 6 subjects showed a similar return to normal RVA following B/T (P=0.066). Mid-morning sOPP was 41.1±5.5 mmHg post-timolol, 46.3±6.5 mmHg post-D/T, and 38.6±6.0 mmHg post-B/T (D/T vs. B/T, P=0.026).
Conclusions:
D/T significantly improved RVA in POAG patients exhibiting RVD while on timolol 0.5% alone. D/T also increased sOPP compared to B/T. There was no significant difference (P=0.37) between D/T and B/T in improving RVA.
Introduction
Several investigators have postulated that wide fluctuations in retinal blood flow with positional change may produce ischemia–reperfusion injury to the retina, leading to retinal ganglion cell loss and axonal degeneration, hallmarks of glaucomatous optic neuropathy.3–7 Consistent with this postulate, other investigators have reported that low OPP8–10 and fluctuations in OPP11,12 are important risk factors associated with the severity of glaucomatous damage in POAG. Coupled with a lack of retinal vascular autoregulation (RVA), fluctuations in OPP would lead to daily repetitive ischemic insults that would then be followed by reperfusion damage to neuronal tissue.
A link between faulty RVA and disc hemorrhage (DH) in POAG has been suggested although the exact mechanism of DH is not clear. 13 If DH is a marker of retinal vascular dysregulation (RVD) in POAG, then the evidence that DH is a risk factor for conversion from ocular hypertension to POAG 14 and for progression of pre-existing disease15–19 suggests that normalization of blood flow regulation may reduce glaucomatous progression.
We have begun to investigate the effect of topical IOP-lowering agents on RVD in POAG. In a retrospective study 20 we found that normal tension glaucoma patients not using brimonidine exhibited marked increases in retinal blood flow while reclining compared to while seated. In contrast, the same patients using brimonidine showed hemodynamic changes consistent with normal autoregulatory control of retinal blood flow.
In the current prospective study, we sought to determine the effects of treatment with fixed combination dorzolamide hydrochloride 2%–timolol maleate ophthalmic solution 0.5% (D/T) and fixed combination brimonidine tartrate 0.2%–timolol maleate ophthalmic solution 0.5% (B/T) compared to the effect of timolol 0.5% alone on RVD in POAG patients with a history of untreated IOP >21 mmHg. We chose these agents because experimental evidence has indicated that each has vasoactive properties.21,22 In addition, pharmacokinetic studies of both agents23,24 have shown that clinical dosing results in concentrations sufficient to elicit vasoactive responses in the retina and optic nerve. On the other hand, there is a clear consensus in the literature 25 that treatment with timolol alone does not have any significant effects upon the retinal circulation. Our hypothesis was that either D/T or B/T or both would be effective at improving RVA in POAG patients with RVD while treated with timolol 0.5% alone.
Methods
Patients
This was a prospective, observer-masked, 2-period crossover study of POAG patients with a history of untreated IOP >21 mmHg and reproducible Humphrey (Zeiss-Humphrey Instruments, Inc., San Leandro, CA) 24-2 standard threshold visual field loss in the left eye using the Swedish Interactive Threshold Algorithm (SITA). Patients were recruited from the practices of 3 of the authors (D.J.R., A.V.T., L.R.P.) at Massachusetts Eye and Ear Infirmary, Boston. The research followed the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board at Massachusetts Eye and Ear Infirmary. Written informed consent to participate was obtained from each subject. The study was registered with clinicaltrials.gov (identifier: NCT00824824).
Patients with POAG aged 40 to 80 years were eligible for the study. Eligible subjects had a history of an untreated IOP >21 mmHg in the left eye and a pattern standard deviation ≥1.0 in this eye. The left eye was used as the study eye. Patients being treated with more than 2 IOP lowering medications concurrently were excluded. All eligible subjects had open angles on gonioscopy with the filtering portion of the trabecular meshwork visible for 360° in both eyes. All subjects also had at least 2 reliable (fixation loss ≤33%, false positives ≤20% and false negatives ≤20%) Humphrey 24-2 SITA standard threshold visual fields showed reproducible glaucomatous loss in the left eye. Patients with evidence of exfoliation or pigment dispersion syndrome in either eye were excluded. Subjects with diabetic retinopathy or a history of ocular laser or incisional surgery in either eye were also excluded. In order to facilitate the retinal blood flow measurements, only subjects with refractive error within the range −10 to +10 diopters, no lens opacities greater than 1+ cortical spokes or 2+ nuclear sclerosis, and pupillary dilation of at least 6 mm following mydriasis were included.
Initial testing
Before the initial testing visit, subjects ceased using their current IOP-lowering medications and were run in for 6 weeks on timolol 0.5% BID OU. All testing visits began at 10:00 AM. IOP was measured in both eyes with the subject seated using Goldmann applanation tonometry (Haag Streit USA, Mason, OH). Pupillary dilation was achieved by instilling one drop of tropicamide 1% in the left eye. A baseline measurement of the systolic, diastolic, and mean brachial artery blood pressure (MAP) in the left arm along with the heart rate (HR) was made using a Keller Vital Signs Monitor (Keller Medical Specialties, Antioch, IL) after the subject was seated for 15 min. Baseline seated OPP (sOPP) was estimated using the standard formula: sOPP=2/3 MAP − IOP. The factor two-thirds adjusts for the decline in blood pressure between the brachial and ophthalmic artery with the subject sitting. 26 Measurement of the baseline arterial blood column diameter and centerline blood speed, with automatic calculation of the blood flow rate was made using a Canon CLBF 100 Laser Blood Flowmeter (Canon, Inc., Tokyo, Japan). 27 In each subject, a site along the inferior temporal retinal artery in the left eye adjacent to the optic disc was used for baseline measurements. This measurement site was chosen because evidence from both visual field data and retinal nerve fiber layer thickness data suggests that the regions inferior and inferior temporal to the disc are most often involved in early glaucoma. 28
Following the baseline measurements, the subjects assumed a posture typically used for face-on X-rays, reclining on their right side with their head supported by a foam wedge making an angle of 24° from the horizontal. Subjects reclined for 30 min while brachial blood pressure and HR were automatically measured in the left arm at 5-min intervals. Laser Doppler blood flow measurements were obtained from the same arterial site that was used at baseline after ∼15 and 30 min of reclining. A 30-min reclining time is used to ensure that a new set of equilibrium conditions is reached. Previous studies26,29 have indicated that a period of at least 5 to 8 min is required for the retinal vasculature to adjust to an altered OPP. Immediately following the 30-min laser Doppler measurement, with the subject still reclining, the IOP in the left eye was measured using Perkins handheld applanation tonometry (Haag Streit USA). In the reclined position, OPP was estimated using the experimentally derived formula: OPPreclining=MAPreclining−IOPreclining, where MAPreclining is the MAP measured in the left arm with the subject reclining on the right side. 30 In a clinical trial comparing Goldmann and Perkins applanation tonometry, 31 measured IOP was, on average, 1 mmHg lower in Perkins compared to Goldmann tonometry. As such, there is minimal impact on the calculation of OPPreclining due to any differences between Goldmann and Perkins tonometry. Subsequently, the subjects rose and blood pressure, HR, and laser Doppler measurements (15 min after rising) were repeated with the subjects sitting.
Randomization
Only those patients who exhibited RVD continued in the study. We determined whether RVD was present in the following way. The percentage change between the retinal blood flow measured while reclining for 30 min and the baseline retinal blood flow measured while seated was calculated. In our initial study, 1 we found that among healthy subjects the change in the blood flow while reclining compared to baseline was +6.5%±12%. For this study, we defined the normal range of blood flow autoregulation as±2 standard deviations about the mean percentage change found in the control group in the initial study (6.5%±24.0%); that is, as −17.5% to +30.5%. Patients with a change in retinal blood flow induced by posture change outside this range were randomized to either D/T BID OU or B/T BID OU for 6 weeks. The coefficient of variation for individual retinal blood measurements using our technique is relatively low (10%–15%) 27 and we have previously reported that assessments of retinal vascular autoregulatory status (both normal and abnormal) are reproducible. 1
Post-treatment testing
After 6 weeks of treatment with one of the fixed combination medications, patients returned for a second testing visit at 10 AM. The same testing protocol described above was repeated. Measurements of arterial blood column diameter and centerline blood speed, with automatic calculation of the blood flow rate, while seated and while reclining, were made at the same arterial site that was used at the initial testing visit. This was followed by 6 weeks of treatment with the opposite fixed combination medication BID OU. Then, a third measure of ocular parameters and presence or absence of RVD took place again beginning at 10AM.
Sample size calculation
Prior to the study, we estimated that 20 POAG patients would be needed to assess whether either fixed combination agent was effective at improving RVA in patients with RVD on timolol 0.5% alone. This calculation assumed that 50% of the enrolled patients would have RVD on timolol 0.5% alone and that the subsequent treatments altered RVA in a dichotomous manner for 80% to 100% of the patients. 32 The study was not powered to assess any differences in RVA responses between the treatments with the 2 fixed combination agents.
Statistical analysis
Results obtained after 30 min of reclining were used for comparisons with the baseline seated measurements. Stepwise multiple linear regression analysis was used to determine which factors were related to the presence or absence of RVD in the patients at the initial testing visit. Chi-squared tests were used to assess the significance of the performance of the fixed combination medications in improving RVA in the patients who exhibited RVD at the initial testing visit. Analysis of variance with post hoc tests was used to determine the significance of differences in the measured parameters following D/T, B/T, and timolol 0.5% alone. Results are expressed as mean±standard deviation. All tests were 2 tailed, and P values less than 0.05 were considered to be statistically significant.
Results
A total of 21 POAG patients participated in the study. Their demographic and ocular characteristics determined at the initial testing visit are shown in Table 1. The data are stratified according to the presence or absence of RVD following a treatment period of 6 weeks with timolol 0.5% BID OU. Seven of the 21 patients had RVD in response to posture change following timolol with blood flow increases ranging from 70% to 102% (n=3) or blood flow decreases ranging from −22% to −33% (n=4) while reclining versus seated.
Mean deviation: Humphrey 24-2 full-threshold visual field mean deviation.
Pattern standard deviation: Humphrey 24-2 full-threshold visual field pattern standard deviation.
Unpaired t-test.
RVA, retinal vascular autoregulation; C, Caucasian; AA, African American; MAP, mean brachial arterial pressure; IOP, intraocular pressure; sOPP, seated ocular perfusion pressure.
Univariate analyses showed no statistically significant differences in the 10 factors listed in Table 1 between the patients with or without RVD. There was a statistical trend (P=0.06), however, toward a lower sOPP (41.1±5.3 mmHg) in the group with RVD compared to the group with normal RVA (46.9±6.6 mmHg). Table 2 shows the results of a stepwise multiple linear regression analysis aimed at determining which factors were related to the presence or absence of RVD in this group of POAG patients. The optimum model includes sOPP and patient age, and indicates that lower sOPP is significantly (P=0.033) associated with the presence of RVD.
Table 3 shows the percentage changes in the retinal arterial blood flow while reclining compared to sitting following the 6 week of treatment with timolol 0.5% alone, D/T, and B/T measured in each of the 7 patients with RVD following timolol 0.5% alone. All 7 patients showed a return of the posture-induced change in retinal blood flow following D/T to levels within the range consistent with normal RVA (P=0.001). Specifically, the blood flow changes induced by posture change at 30 min ranged from +3% to+28%. Measurements were obtained on only 6 of the patients following B/T. In one patient, the post-B/T measurement was not completed due to technical issues. Four of these 6 patients showed a return of the posture-induced change in retinal blood flow to levels within the range consistent with normal RVA (P=0.066). There was no significant difference (P=0.37) between D/T and B/T in improving RVA. There were no significant differences in baseline seated retinal arterial blood flow (P=0.73) following each of the 3 treatment periods (post-timolol 0.5%: 11.8±2.5 μL/min; post-D/T: 13.0±4.1 μL/min; post-B/T: 11.8±2.5 μL/min).
Measurement not completed due to technical issues.
D/T, dorzolamide 2%–timolol 0.5%; B/T, brimonidine 0.2%–timolol 0.5%.
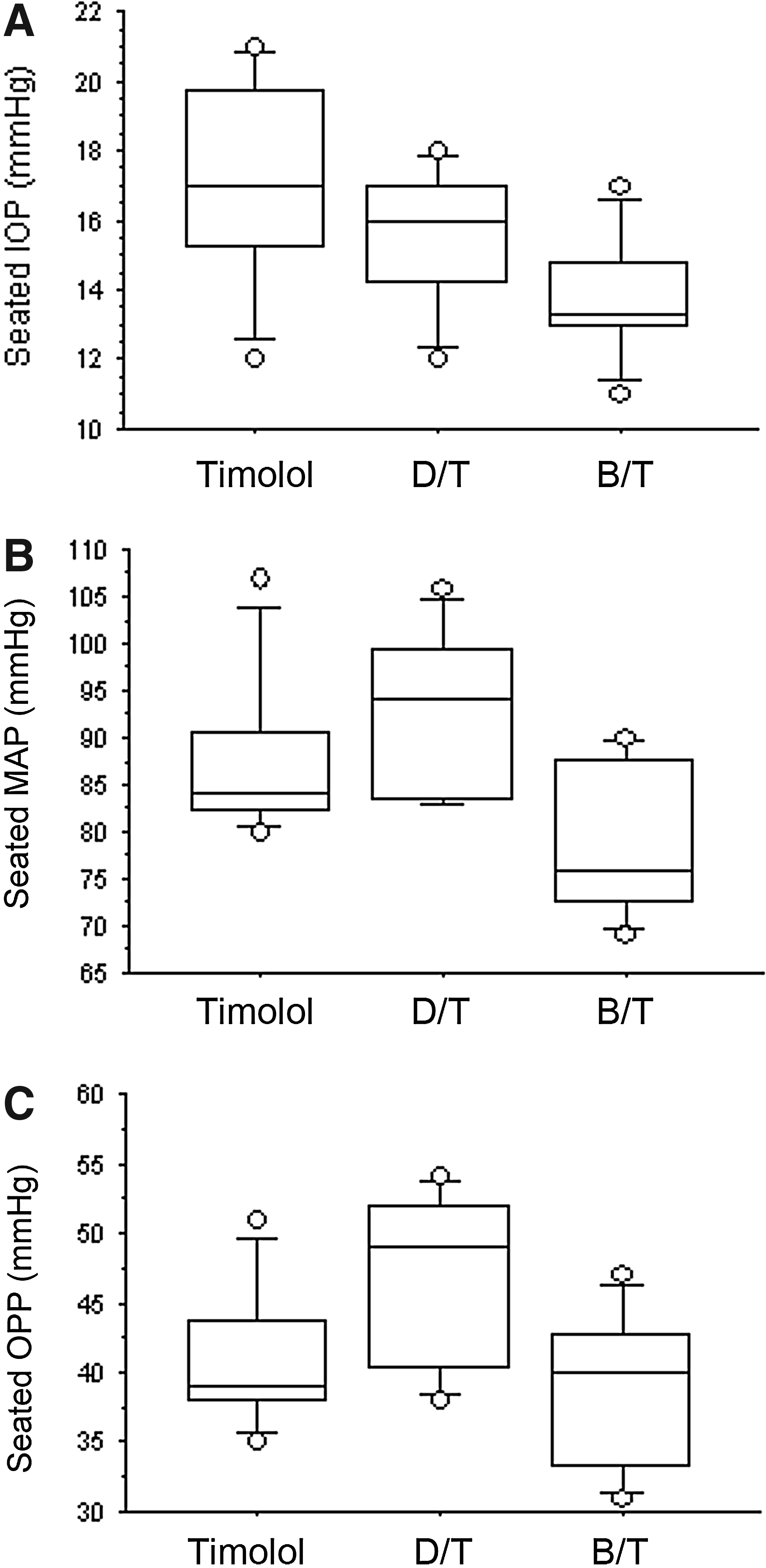
Figure 1 shows the results for seated IOP, seated MAP, and sOPP following each of the 3 treatment periods. Seated IOP was 17.1±3.1 mmHg post-timolol 0.5%, 15.6±2.1 mmHg post-D/T, and 13.7±1.9 mmHg post-B/T (timolol 0.5% vs. B/T, P=0.016). However, seated MAP was significantly higher following D/T (92.7±9.2 mmHg) than following B/T (79.1±8.5 mmHg; P=0.011). As a result, sOPP was 41.1±5.5 mmHg post-timolol 0.5%, 46.3±6.5 mmHg post-D/T, and 38.6±6.0 mmHg post-B/T (D/T vs. B/T, P=0.026).
Discussion
Our previous studies identifying RVD in POAG1,20 were conducted in patients with a known untreated maximum IOP <22 mmHg in both eyes. The results of this study show that RVD is also present in POAG patients with a history of untreated IOP >21 mmHg. Our finding that a lower sOPP was the main determinant of RVD is consistent with the results of epidemiologic and clinical trial evidence8–10 indicating that low OPP is an important risk factor for disease progression in POAG.
We found that 7 of the 21 patients tested following 6 weeks of treatment with timolol exhibited RVD. Following subsequent treatment with D/T for 6 weeks, the retinal vascular autoregulatory response to posture change in all 7 of these patients was restored to a range previously reported 1 for normal healthy subjects. While several studies have reported that dorzolamide improves ocular blood flow characteristics in POAG patients,33–37 only 2 prior studies have specifically investigated the effect of dorzolamide on retinal vascular autoregulaton. One such study 38 has shown that dorzolamide has a positive autoregulatory vasoactive effect on the retinal arterial diameter in POAG patients following artificial IOP elevation. The other study 39 reported an improvement in retinal vascular reactivity to hypercapnia after dorzolamide treatment in patients with POAG. The findings in our current study strongly suggest that dorzolamide when combined with timolol does indeed improve retinal vascular autoregulatory function.
Six of the 7 patients with RVD following treatment with timolol alone were successfully tested following treatment with B/T. The retinal vascular autoregulatory response to posture change was restored to the normal range in 4 of these 6 patients. In a previous retrospective study of patients with normal tension glaucoma, 20 we found that off brimonidine, 6 patients exhibited marked increases in retinal blood flow while reclining compared to while sitting. On brimonidine, the hemodynamic changes in all 6 patients were consistent with normal autoregulatory control of retinal blood flow. The reasons why B/T did not uniformly normalize RVD in the present study are not clear. However, combining the results of the retrospective study with the current study shows that brimonidine or B/T improved RVA in 10 of 12 POAG patients, a more realistic representation of the effectiveness of brimonidine in treating RVD.
The vasoactive properties of brimonidine are complex. Rosa et al. 22 reported results from an in vitro study of the effect of varying concentrations of brimonidine on isolated retinal arterioles. They found that smaller arterioles (50 μm in diameter) responded heterogeneously with either dilation or constriction and that the incidence and magnitude of vasoconstriction were increased with increasing brimonidine concentration. Conversely, larger arterioles (80 μm in diameter) dilated dose dependently to brimonidine. Clinical studies indicate that the net effect of this complex vasoactive behavior is that retinal blood flow remains unchanged with brimonidine treatment. Schmidt et al. 40 and Inan et al. 41 used color Doppler ultrasound and reported no differences in the circulatory parameters in the central retinal artery in POAG patients before and after brimonidine treatment. Other studies reported that brimonidine treatment did not alter intraretinal circulatory parameters in ocular hypertensive patients 42 or in healthy volunteers. 43
Our study was not powered to detect a difference in the abilities of D/T versus B/T to improve RVA since we had no a priori hypothesis as to why one fixed combination agent would be superior to the other in this regard. There was no significant difference between D/T and B/T in improving RVA.
Regarding IOP and OPP effects following treatment with D/T or B/T, the results were as expected. There was no significant difference in IOP response between the 2 fixed combination agents as has been reported. 44 However, MAP was significantly higher following D/T than following B/T. Brimonidine has been previously shown to decrease systemic blood pressure. 41 As a result, mid-morning, sOPP was significantly lower following B/T compared to following D/T. It appears that the maintenance of a higher OPP with D/T may play a role in the performance of that agent in improving RVD in POAG patients. However, B/T had the greatest IOP lowering effect of the 3 treatments. There is experimental evidence that in the subfoveolar choroidal circulation 45 and in the optic nerve head circulation 46 that a reduction in IOP itself, independent of changes in OPP, improves blood flow autoregulation. Whether or not this phenomenon also occurs in the retinal circulation remains to be demonstrated.
In this study, only one-third of the patients tested following the 6-week treatment period with timolol exhibited RVD and were then randomized. In our initial study 1 patients were either untreated (n=5) or receiving a variety of topical IOP-lowering medications (n=13) before testing. In that study, 61% of the patients exhibited RVD when tested. Only one patient in that study was treated with timolol alone, and that patient did exhibit RVD. In our current study, we cannot rule out the possibility that timolol alone improved RVA in some patients. Another possibility is that POAG patients with a history of untreated elevated IOP are less likely to have RVD than patients with normal tension glaucoma.
A potential limitation of this study was that there was no washout period between the 6-week treatment periods with D/T and B/T (4 cases) or between B/T and D/T (3 cases). However, the 6-week duration of each treatment period extended well beyond the typical 2-week washout period for dorzolamide 47 and the 3-week washout period for brimonidine 48 so that any overlap effects were unlikely. Another potential limitation of the study was that the range of blood flow changes used to determine whether or not a patient exhibited RVD with posture change was based on results from a single study. 1 The results in Table 3, however, show that in the majority of cases the blood flow changes with posture change were dramatically decreased following treatment with D/T and/or B/T compared to the changes measured following treatment with timolol 0.5%, thus minimizing the likelihood of misclassification of RVD. Finally, the study lacked racial diversity among the subjects, which limits the generalizability of the results. Only one subject was African American; the remainder were Caucasion. Strengths of this study were its prospective nature, and that the observers were masked to the order of the treatments following randomization.
While it is not feasible to assess retinal vascular autoregulatory capacity in the clinical setting, DH may be a reasonable surrogate for RVD. We have reported exaggerated posture change-induced retinal blood flow responses in glaucoma patients with a history of DHs. 1 As demonstrated in the Ocular Hypertension Treatment Study, DH is an important risk factor for the conversion from ocular hypertension to POAG. 14 For patients with a DH in the setting of high tension POAG, D/T appears to improve RVA while also producing beneficial effects on IOP and OPP. The functional visual consequences of these effects in comparison to those produced by other agents remain to be determined.
In conclusion, we found that lower sOPP was a major determinant of RVD. D/T improved RVA in POAG patients who exhibited RVD while treated with timolol alone and had the desired additional effect of increasing the sOPP compared to B/T.
Footnotes
Author Disclosure Statement
This investigator-initiated study was supported by a grant from Merck & Co., Inc. The authors retained total editorial control over the contents of the article. Dr. Rhee has received research funding from Merck & Co., Inc., that is unrelated to this study. He has also been a consultant for Merck & Co., Inc., and for Allergan, Inc. Dr. Pasquale has received research funding from Allergan, Inc., that is unrelated to this study. The other authors declare no conflict of interest. Additional support was provided by a Research to Prevent Blindness Award (LRP), the Harvard Glaucoma Center of Excellence, a Harvard Distinguished Scholar Award (LRP), and the Margolis Fund. The Glaucoma Service at Massachusetts Eye and Ear Infirmary is a recipient of a Horizon Grant from Allergan, Inc.