
Abstract
Abstract
Background:
To further evaluate the effect of intravitreal bevacizumab (IVB) for the treatment of branch retinal vein occlusion in a meta-analysis of previous studies.
Methods:
Pertinent publications were identified through systemic searches of PubMed, EMBASE, and the Cochrane Controlled Trials Register up to July 2012. Data on central macular thickness and best-corrected visual acuity obtained at 4 and 12 weeks after treatment were extracted. Groups of patients receiving IVB were compared with control groups.
Results:
Four randomized controlled and 3 comparative studies were included. A publication bias was not detected by funnel plots, the Egger method, or the Begg method. Best corrected visual acuity measured at 4 and 12 weeks after baseline increased significantly in the IVB groups as compared with the control groups [4 weeks: weighted mean deviation (WMD)=−0.09; 95% confidence interval (CI): −0.12, −0.05; P<0.001; at 12 weeks: WMD=−0.21; 95% CI: −0.30, −0.12; P<0.001]. Similarly, reduction in central macular thickness at 12 weeks after baseline was significantly higher in the IVB groups than in the control groups (WMD=−29.02; 95% CI: −50.56, −7.49; P=0.008). The change in central macular thickness at 4 weeks after baseline did not vary significantly between the IVB groups and control groups (WMD=−20.48; 95% CI: −67.30, 26.34; P=0.39). All included studies taken separately reported on a significant increase in visual acuity in the IVB groups.
Conclusions:
Patients with branch retinal vein occlusion experienced a significant benefit in terms of visual improvement and reduction in central macular thickness after the intravitreal injection of bevacizumab.
Introduction
Methods
Literature search
Two reviewers independently searched the following electronic databases: PubMed, EMBASE, and the Cochrane Controlled Trials Register up to 30 July 2012. We used free text and thesaurus terms, including bevacizumab, branch retinal vein occlusion, and macular edema. Full articles were retrieved, when titles and/or abstracts met this objective. A manual cross-reference search of the bibliographies of relevant articles was conducted. The inclusion criteria of references were (1) all published studies comparing IVB alone versus other treatments for BRVO. The search included randomized controlled trials and high-quality comparative studies; (2) pretreatment and post-treatment visual acuity and macular thickness being measured and recorded in the article; and (3) the number of study participants being larger than 20. There was no language restriction. For the publications from the same group of authors, only the article with the largest number of patients treated for BRVO with IVB was used. The selected studies were appraised by 2 reviewers, who independently assessed their quality using the modified Jadad score table. 17 Methodological quality included allocation concealment, method of allocation to treatment, masking of outcome assessment, and completeness of follow-up. The postoperative outcome parameters included best-corrected visual acuity (BCVA) and central macular thickness at 4 and 12 weeks after IVB.
For all studies, we extracted the following data from the original publications: first author and year of publication; study site; study design; sample size and age of the participants; treatment method and follow-up duration; numbers of lost follow-up; treatment outcome measures, including BCVA and central macular thickness. Data extraction was conducted by 2 reviewers independently, and discordance was resolved through discussion until 100% agreement was reached on the final interpretation of the data.
The meta-analysis of the effect of IVB for macular edema secondary to BRVO was carried out by Cochrane Review Manager (RevMan; version 5.0 software). The treatment effect was estimated by means of weighted mean deviation (WMD) of BCVA and central macular thickness. Random effects models were used for the meta-analysis, taking into account the possibility of heterogeneity between studies which was tested by the Q test (P<0.10 was considered to indicate statistically significant heterogeneity) and the I 2 statistic (values of 25%, 50%, and 75% are considered to represent low, medium, and high heterogeneity, respectively). Publication bias was assessed by visually inspecting a funnel plot.
Results
A total of 75 articles were identified, out of which 56 articles were excluded due to the reasons mentioned above. It left 19 articles for full text review. Twelve of these were dropped from the study for reasons such as similarities to previous studies from the same group of authors (Fig. 1). Seven studies published between 2005 and 2012 were eventually included in the meta-analysis (Table 1).18–24
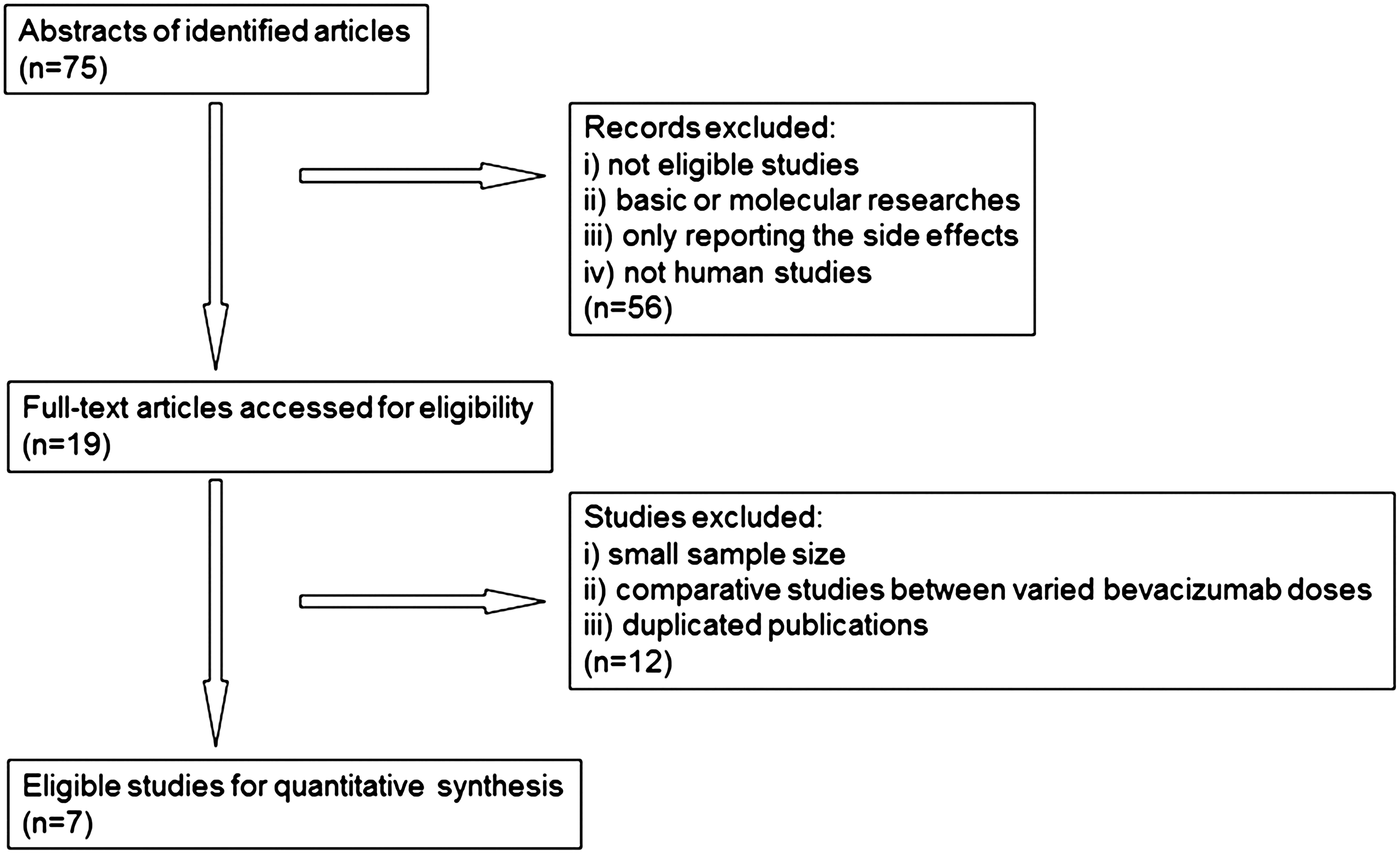
Flowchart of literature search and study selection.
IVB, intravitreal bevacizumab.
Four of these studies were randomized controlled trials and 3 investigations were retrospective comparative studies (Table 1). The sample sizes varied from 29 to 86 study participants, and the follow-up durations varied from 3 months to 12 months. Grid laser photocoagulation and intravitreal injection of triamcinolone acetonide (IVTA) or placebo application were used in the control groups. The treatment outcome estimates were provided for a total of 183 eyes in the IVB group and 213 eyes in the control group. In each study, distribution of age, gender, and history of retinal vein occlusion did not vary significantly between the IVB groups and the control groups.
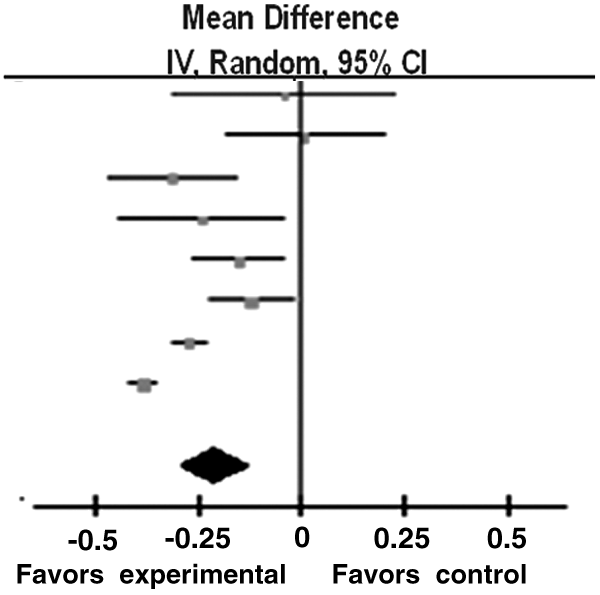
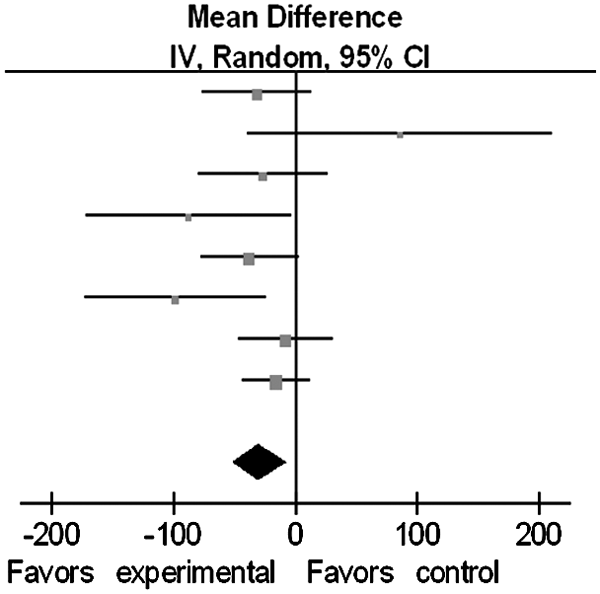
Six studies reported data on BCVA at 4 weeks after the initial treatment. BCVA was transferred to the logarithm of the minimum angle of resolution and summarized by means of meta-analysis. BCVA at 4 weeks after IVB treatment was significantly increased as compared to the control group [WMD=−0.09; 95% confidence interval (CI): −0.12, −0.05; P<0.001] (Table 2) (Fig. 2). All the 7 studies reported data on BCVA at 12 weeks after the initial treatment (Table 3) (Fig. 3). High heterogeneity between studies was detected (I2=86%) and therefore random-effects model analysis was used. Compared with the control groups, BCVA improvement was significant in the IVB groups (WMD=−0.21; 95% CI: −0.30, −0.12; P<0.001). Data on central macular thickness at 4 weeks after the initial treatment were available in 6 studies. A change in central macular thickness at 4 weeks after IVB did not vary significantly between the IVB groups and the control groups (WMD=−20.48; 95% CI: −67.30, 26.34; P=0.39) (Table 4) (Fig. 4). A high heterogeneity between the studies was detected (I2=80%). Random-effects model analysis showed that the effect of reduction in central macular thickness did not differ significantly between the IVB groups and the control groups. All 7 studies reported on the central macular thickness measured at 12 weeks after the initial treatment with low heterogeneity (I2=35%) (Table 5) (Fig. 5). Random-effects model analysis showed that the reduction in central macular thickness at 12 weeks after initial treatment IVB was significantly higher in the IVB group than in the control groups (WMD=−29.02; 95% CI: −50.56, −7.49; P=0.008).

Comparison of best corrected visual acuity at 4 weeks after initial treatment between intravitreal bevacizumab (IVB) group and control group in published studies (from top to bottom): Hou et al. (2009), 20 Kim and Park (2009), 18 Moradian et al. (2011), 19 Ramezani et al. (2012), 22 Russo et al. (2009), 23 Cekiç et al. (2010), 21 and Cekiç et al. (2010). 21 CI, confidence interval.
Comparison of best-corrected visual acuity at 12 weeks after initial treatment between IVB groups and control groups in published studies (from top to bottom): Hou et al. (2009), 20 Kim and Park (2009), 18 Moradian et al. (2011), 19 Ramezani et al. (2012), 22 Russo et al. (2009), 23 Cekiç et al. (2010), 21 and Cekiç et al. (2010). 21

Comparison of central macular thickness at 4 weeks after initial treatment between IVB groups and control groups in published studies (from top to bottom): Hou et al. (2009), 20 Kim and Park (2009), 18 Moradian et al. (2011), 19 Ramezani et al. (2012), 22 Russo et al. (2009), 23 Cekiç et al. (2010), 21 and Cekiç et al. (2010). 21
Comparison of central macular thickness at 12 weeks after initial treatment between IVB groups and control groups in published studies (from top to bottom): Hou et al. (2009), 20 Kim and Park (2009), 18 Moradian et al. (2011), 19 Ramezani et al. (2012), 22 Russo et al. (2009), 23 Cekiç et al. (2010), 21 and Cekiç et al. (2010). 21
Heterogeneity: Tau2=0.00; Chi2=8.29, df=6 (P=0.22); I2=28%.
Test for overall effect: Z=4.57 (P<0.00001).
CI, confidence interval.
Heterogeneity: Tau2=0.00; Chi2=8.29, df=6 (P=0.22); I2=28%.
Test for overall effect: Z=4.55 (P<0.00001).
Heterogeneity: Tau2=3105.41; Chi2=29.64, df=6 (P<0.0001); I2=80%.
Test for overall effect: Z=0.86 (P=0.39).
Heterogeneity: Tau2=314.90; Chi2=10.83, df=7 (P=0.15); I2=35%.
Test for overall effect: Z=2.64 (P=0.008).
Separating the patients who underwent IVTA from the whole control group, BCVA after IVB treatment was significantly increased as compared to the control group at 4 weeks (WMD=−0.08; 95% CI: −0.12, −0.04; P<0.001), 12 weeks (WMD=−0.19; 95% CI: −0.31, −0.06; P=0.003), and 24 weeks (WMD=−0.18; 95% CI: −0.21, −0.14; P<0.001) after initial treatment. Central macular thickness in the patients who underwent IVB treatment did not vary significantly from the macular thickness in the IVTA patients at 4 weeks (WMD=9.2; 95% CI: −21.4, 39.9; P=0.55), 12 weeks (WMD=−13.1; 95% CI: −34.2, 8.1; P=0.23), and 24 weeks (WMD=−21.8; 95% CI: −71.8, 28.2; P=0.39) after initial treatment.
Based on funnel plots for the analysis of visual acuity, no obvious evidence of publication bias was found for the treatment outcome estimates (BCVA and central macular thickness at 4 weeks after initial treatment) (Figs. 6 and 7). Since, however, the number of enrolled studies was low, we additionally applied the Egger method and Begg method to measure a publication bias. Both methods did not reveal a significant publication bias (BCVA at 4 weeks after initial treatment, Egger method: P=0.15, Begg method: P=0.13; central macular thickness at 4 weeks after initial treatment, Egger method: P=0.71, Begg method: P=0.74).
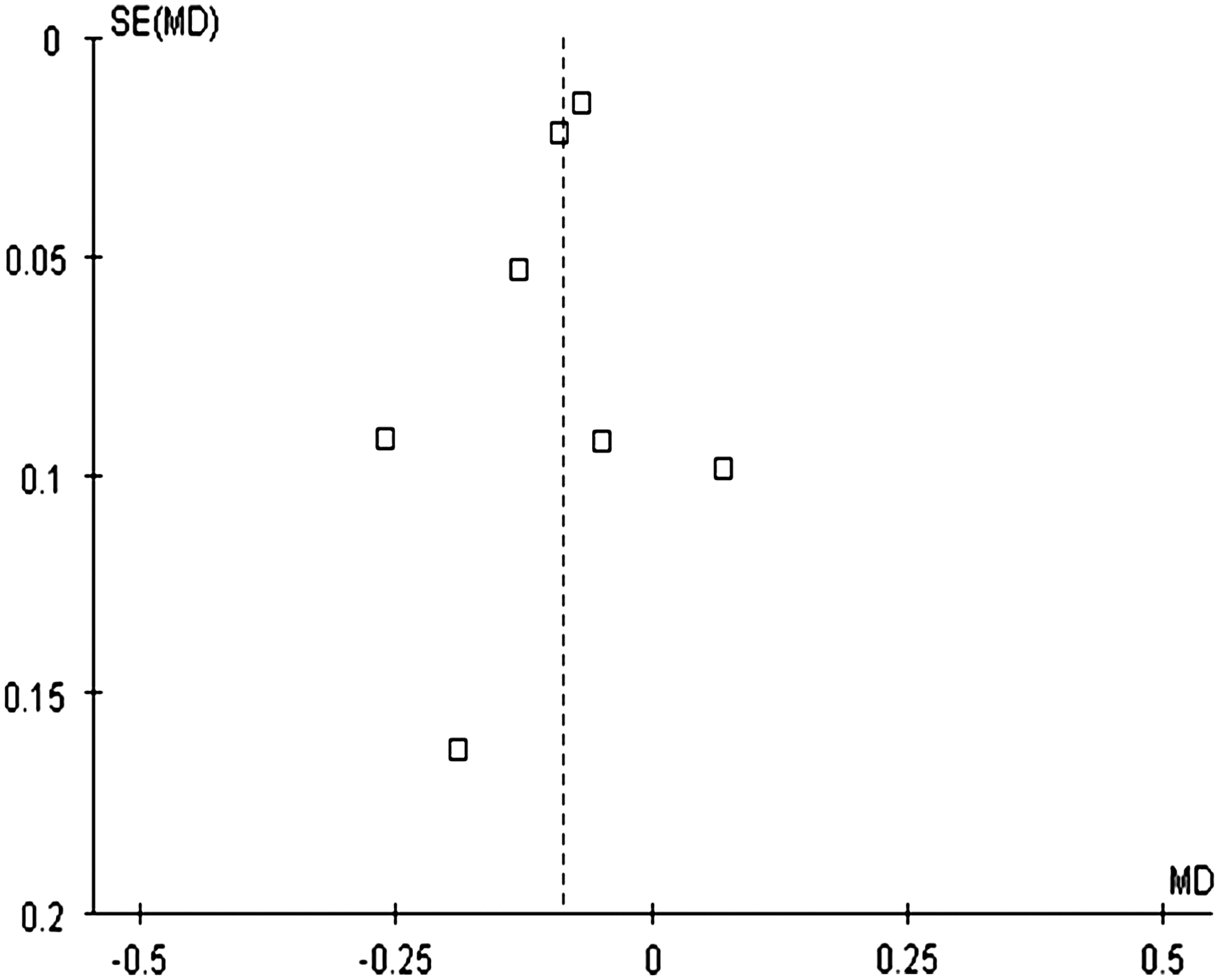
Funnel plots with respect to best-corrected visual acuity at 4 weeks after initial treatment. Standard error (SE); mean deviation (MD).

Funnel plots with respect to central macular thickness at 4 weeks after initial treatment.
Discussion
Including 4 randomized controlled studies and 3 comparative investigations into our meta-analysis revealed that BCVA measured at 4 weeks and at 12 weeks after baseline was significantly higher in the IVB groups than in the control groups (4 weeks: P<0.001; at 12 weeks: P<0.001). Similarly, reduction in the central macular thickness at 12 weeks after baseline was significantly higher in the IVB groups than in the control groups (P=0.008), while the change in central macular thickness at 4 weeks after baseline did not vary significantly between the IVB groups and control groups (P=0.39). The results of our meta-analysis suggest that IVB led to an increased visual acuity and corresponding reduction in central macular thickness for a period of 3 months after the injection.
These results are in agreement with other small-scaled studies on the intravitreal use of bevacizumab for the therapy of BRVO, which did not fulfill the criteria to be included into the meta-analysis.10–16 The findings in our meta-analysis were also in agreement with investigations on the intravitreal application of bevacizumab as therapy of other retinal or macular edematous and neovascular diseases such as diabetic macular edema, proliferative diabetic retinopathy, retinopathy of prematurity, central retinal vein occlusion, and others.25–27
Since the number of participants in the examined studies was relatively low, our meta-analysis could not address the frequency of side effects of the IVB treatment. Previous large-scaled studies on several thousand study participants had revealed that the risk of the main complication, that is, an injection-associated intraocular infection, ranged between 1:1,000 and 1:3,000. 28 These studies also suggested, that the risk for this complication was mainly independent of the underlying retinal disease.
The main potential limitation of our meta-analysis was that the number of studies which fulfilled the inclusion criteria of this meta-analysis and which were eventually included into the analysis was relatively low as was the number of study participants. This led to a relatively low number of patient months in the meta-analysis. The studies, however, originated from several continents, and all studies, also taken separately, led to the same conclusion of a significant benefit in terms of visual improvement and reduction in macular edema after the intravitreal injection of bevacizumab. Another limitation of this meta-analysis was that the studies used different optical coherent tomographs and that best corrected visual acuity was tested with visual charts varying between the studies. Since, however, the same techniques and procedures were applied within the studies, the respective study groups and control groups were examined under the same protocol.
In conclusion, patients with branch retinal vein occlusion experienced a significant benefit in terms of visual improvement and reduction in macular edema after the intravitreal injection of bevacizumab.
Footnotes
Acknowledgment
This study was supported by the Beijing Novel Program (No:2009B04).
Author Disclosure Statement
Financial interest: Jost B. Jonas: Consultant for Allergan, Inc.; Merck & Co., Inc.; Alimera Co.; Patent holder with CellMed AG, Alzenau, Germany; all other authors: None.