
Abstract
Abstract
Imaging of the eye plays an important role in ocular therapeutic discovery and evaluation in preclinical models and patients. Advances in ophthalmic imaging instrumentation have enabled visualization of the retina at an unprecedented resolution. These developments have contributed toward early detection of the disease, monitoring of disease progression, and assessment of the therapeutic response. These powerful technologies are being further harnessed for clinical applications by configuring instrumentation to detect disease biomarkers in the retina. These biomarkers can be detected either by measuring the intrinsic imaging contrast in tissue, or by the engineering of targeted injectable contrast agents for imaging of the retina at the cellular and molecular level. Such approaches have promise in providing a window on dynamic disease processes in the retina such as inflammation and apoptosis, enabling translation of biomarkers identified in preclinical and clinical studies into useful diagnostic targets. We discuss recently reported and emerging imaging strategies for visualizing diverse cell types and molecular mediators of the retina in vivo during health and disease, and the potential for clinical translation of these approaches.
Introduction
While ophthalmic imaging instrumentation is capable of imaging retinal morphology with unprecedented resolution, a challenge remains to detect subclinical retinal changes, which occur before advanced retinal disease. Subtle cellular and molecular changes may occur in the retina before the point at which disease can be detected by current ophthalmic diagnostic imaging. Furthermore, development of strategies for imaging events, which occur at the molecular level, may aid efforts to more closely track disease progression and evaluate a response to therapeutics. Toward this objective, a number of preclinical and clinical studies using a number of molecular profiling techniques such as mass spectrometry and sequencing have confirmed that molecular changes can precede retinal structural changes in a number of diseases responsible for vision loss, including age-related macular degeneration, glaucoma, diabetic retinopathy, and retinopathy of prematurity.11–20 Therefore, there is a strong and clinically unmet need to translate imaging strategies capable of detecting disease biomarkers in the patient.
The development of strategies, which bridge the discovery of retinal molecular biomarkers associated with disease susceptibility [e.g., mitochondrial dysfunction in retinal ganglion cells (RGCs) before apoptosis], advancement [e.g., the dry to wet age-related macular degeneration (AMD) transition], and regression due to effective treatment (e.g., responsiveness to antivascular endothelial growth factor therapy) with advances in imaging methods hold the potential to revolutionize ophthalmology. In this review, we will discuss strategies for interrogating the retina at the cellular and molecular level using ophthalmic imaging instrumentation and targeted contrast agents as they pertain to imaging specific disease-relevant cell types, along with their potential for clinical translation.
Molecular Imaging of RGCs
RGC dysfunction, apoptosis, and/or necrosis have been observed in a number of retinal diseases and insults, including glaucoma, ischemic disease, and ocular injury.21–23 Using conventional imaging techniques, RGC dysfunction cannot be detected before cell death and even RGC death may not be detectable until over 20% of RGCs have been lost. 23 Similarly, visual field measurements detect retinal damage following widespread RGC apoptosis, and may not allow for early detection of diseases like glaucoma. Therefore, methods for detection of dysfunctional RGCs before their death, or at the very least detection of enough apoptosing or necrosing RGCs to lead to substantial visual deficits, are needed for improved diagnosis of RGC-related diseases. Identification of RGC deficits earlier in the time course of retinal disease would allow for timely therapeutic interventions with potentially improved outcomes in the patient.
Important progress has been made in the detection of RGC apoptosis with improved sensitivity. Using a technique developed by Cordeiro and colleagues named detection of apoptosing retinal cells (DARC), single-cell detection of RGC apoptosis has been demonstrated in experimental animal models of retinal diseases, and efforts to evaluate DARC in clinical trials have commenced.24–29 This imaging approach takes advantage of plasma membrane redistribution in apoptosis, which involves the translocation of the phosphatidylserine (PS) phospholipid from the inner to outer membrane leaflet, at which point, PS is accessible to extracellular targeting ligands. In DARC, fluorescently labeled Annexin V is administered via intraocular injection, and binds specifically to PS on apoptosing RGCs, 30 which can be detected by ophthalmic fluorescence imaging instrumentation (Fig. 1). Another innovative approach for detecting apoptosis with high specificity and sensitivity involves the use of caspase enzyme-activatable fluorophores. Piwnica-Worms and colleagues developed this technique, which utilizes a peptide-based fluorescent probe called TcapQ for in vivo detection of RGC apoptosis.31–33 TcapQ is sensitive to active caspases such as caspase 3 involved in RGC apoptosis, and indicates the presence of active effector caspases. The peptide is administered intravitreally, and contains a modified cell-penetrating Tat peptide demonstrated to exhibit efficient RGC internalization in animal models. 34 The peptide also contains a short peptide sequence, which is cleaved by caspases. On one end of the cleavable sequence, a fluorophore is coupled to the peptide, and on the other end, an organic fluorescence quencher is conjugated, which prevents emission of fluorescence from TCapQ unless the peptide is cleaved by caspase, liberating the fluorophore from its quencher. This concept has been further developed into a second-generation near-infrared probe, KcapQ. 35 KcapQ has a modified peptide sequence to maintain high signal-to-background ratios due to improved quenching and caspase cleavage efficiencies, as well as reduced potential for toxicity making it a useful probe for imaging RGC death. A highlight of DARC and CapQ techniques are their amenability to quantitative imaging instrumentation and image processing. With appropriate imaging instrumentation, it will be possible to quantify apoptotic RGCs in the retina to standardize diagnosis and monitoring.
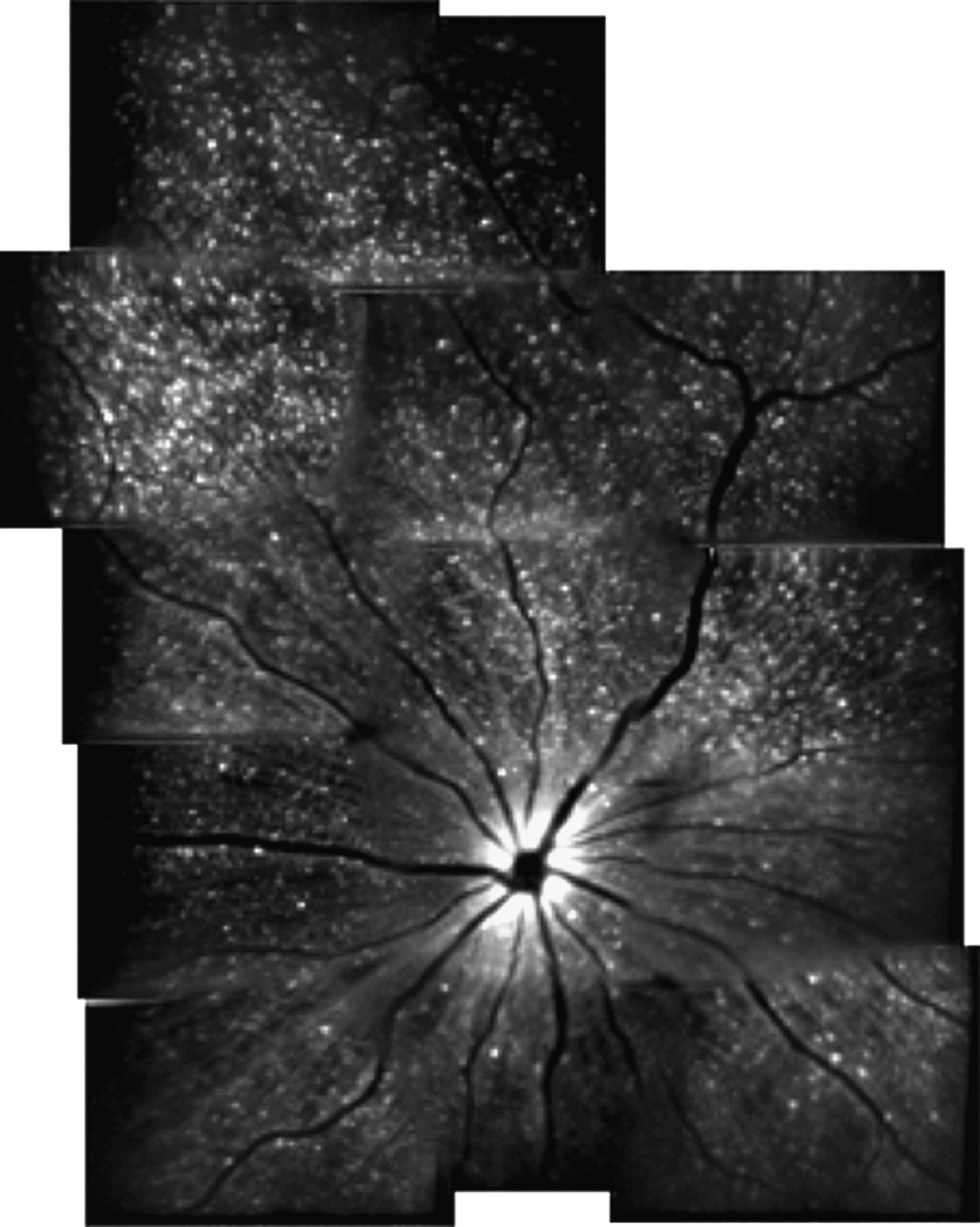
The detection of apoptosing retinal cells imaging approach for detecting retinal ganglion cell (RGC) apoptosis in animal models of ocular disease. Representative montage in vivo image of RGC apoptosis in a rat treated with intravitreally injected staurosporine. Imaging was accomplished using a confocal scanning laser ophthalmoscope with argon laser (488 nm) excitation of intravitreally injected Alexa Fluor 488-Annexin V conjugates, allowing visualization of apoptosing RGCs (hyperfluorescent white dots). Reproduced with permission from Cordeiro. 24
The National Eye Institute, along with a number of clinicians and scientists, have collectively underscored the need for earlier diagnostic measurements for assessing RGC health, 26 and to that end, a technique for early detection of apoptosis is imperative. The 2 aforementioned approaches, DARC and T- or KCapQ, have potential for clinical translation. DARC is entering clinical trials, and radiolabeled Annexin V has been used in over 30 clinical trials for diseases such as myocardial infarction, ischemic brain injury, and a number of cancers using radiological techniques with no significant indications of tissue toxicity. 26 Therefore, the DARC approach has strong potential for clinical translation, and if incorporated into standard ophthalmic practice, this molecular imaging approach will likely pave the way for effective neuroprotective strategies to halt or stabilize RGC dysfunction and death. Likewise, the CapQ approach may prove to be clinically translatable following further assessments of long-term potential for toxicity and off-target effects due to the lack of cell-type specificity for the cationic Tat peptide, 34 as well as biodistribution and clearance, due to the observation that TCapQ can be transported to the optic nerve. 34 Both approaches are amenable for imaging by widely adopted retinal imaging instrumentation, which will facilitate translation and address an important need in the field by detecting RGC death early in disease.
A promising opportunity for molecular imaging to play a role in RGC-related diseases lies in the imaging of RGC dysfunction before cell death. The aforementioned techniques utilizing Annexin V and CapQ only enable imaging of RGC apoptosis, and do not enable detection of sick RGCs before cell death. Methods for detection of molecular processes associated with dysfunctional RGCs would provide an opportunity for therapeutic intervention to prevent cell death and subsequent visual deficits. Oxidative stress has been implicated as a possible contributor to RGC death in injury and glaucoma attributable to generation of reactive oxygen (ROS) and nitrogen species, 36 and several approaches from other fields used to image ROS products may be useful in detection of early RGC dysfunction. For example, molecular probes are available for imaging singlet oxygen (Singlet oxygen sensor green37–40 ), superoxide (dihydroethidium 41 ), and hydrogen peroxide (peroxalate nanoparticles and numerous other probes42–44 ). Of these probes, only hydrogen peroxide has been successfully imaged in vivo using targeted imaging probes, as demonstrated using a mouse model of lipopolysaccharide-induced inflammation. 42 Therefore, while these imaging agents have not been tested for their utility in the retina or even in vivo in many cases, their potential compatibility with ophthalmic imaging equipment warrant their further consideration for detecting molecular insults in RGC-related diseases that contribute to cell death. Other potential molecular imaging targets for consideration in these diseases are RGC axonal transport deficits, mitochondrial dysfunction, as well as glutamate and calcium levels, as abnormalities involving these targets have been implicated in RGC dysfunction and death.45–48 Several imaging probes described in the literature may be useful for interrogating these targets in vivo. Fluorescently labeled proteins, such as the brain-derived neurotrophic factor, cholera toxin subunit, dextrans, and lectins, can be utilized to monitor the efficiency of RGC uptake and transport, although specialized imaging equipment and/or multiple modalities may be required for such approaches, and the species used for axonal tracing have not been extensively tested for their toxicity.47,49–51 The mitochondria-selective JC-1 dye has been used to monitor changes in mitochondrial membrane potential, which is a function of the dye's fluorescence emission spectra. 52 Novel sensors for glutamate have been developed, including the E glutamate optical sensor, which contains a glutamate-binding receptor subunit and a fluorophore, which changes its intensity upon a glutamate interaction.53,54 Calcium sensor dyes, such as Fura2, calcium green, and indo-1, have been developed for imaging intracellular calcium and can be adapted for in vivo applications. 55 These dyes generally feature an acetoxymethyl ester, which enables their intracellular uptake, and through ratiometric optical imaging techniques and specially configured imaging instrumentation such as 2 photon microscopy, intracellular, and tissue Ca2+ levels can be determined. 56 Therefore, an abundance of molecular imaging probes yet to be applied toward ocular disease diagnosis for glaucoma and other RGC-related diseases hold great promise in improving the level of detail achieved in ophthalmic diagnosis. An important hurdle to implementation of these approaches in the clinic will be to determine quantitative baseline metrics for the imaging parameters in healthy patients, such that disease thresholds for events such as defective axonal transport, mitochondrial dysfunction, and ROS generation and concentrations in the retina can be objectively defined for diagnostic procedures.
Molecular Imaging of the Retinal Pigment Epithelium
The retinal pigment epithelium (RPE) is an important cell layer for retinal health that is located between the retinal photoreceptor outer segments and choriocapillaris. The RPE is a postmitotic monolayer that serves as the outer portion of the blood–retina barrier, which is necessary to prevent diffusion of harmful components in circulating blood into the retina. Additionally, the RPE is involved in clearing the photoreceptor outer segments of toxins produced during the visual cycle, transporting nutrients and metabolites from the choroid, and absorbing light energy. Defects in the RPE structure and function can lead to a number of retinal degenerative and aging diseases such as retinitis pigmentosa, 57 Stargardt disease, 58 and AMD. 59 The spectral domain OCT and associated image processing techniques have been critical in improving our understanding of the RPE structure and function in health and disease. Regarding other imaging modalities used for imaging the RPE, in vivo reflectance imaging of the RPE is difficult due to the overlapping photoreceptor layer, which obscures it, but the RPE can be visualized noninvasively on account of intrinsic autofluorescence of RPE molecules, and changes in this autofluorescence profile over time can be used in diagnosis and monitoring of RPE-related diseases.60,61 Recently, the adaptive optics scanning laser ophthalmoscope (SLO) was modified for imaging the RPE mosaic with the cellular and subcellular resolution.62,63 Therefore, imaging instrumentation is well-suited for imaging the RPE and is poised to make a transition whereby it could accommodate molecular imaging contrast agents. Although targeted molecular imaging agents for interrogating the RPE have yet to be extensively studied, some areas of exploration in this arena are discussed.
Autofluorescence imaging techniques for imaging intrinsic RPE molecules will continue to play an important role in preclinical studies as well as diagnosis of RPE-related diseases.64–67 One of the major imaging targets in this area, lipofuscin, is a byproduct of photoreceptor phagocytosis that is stored in granules on the basal side of the RPE and is composed of digested lipid and protein aggregates. 64 In normal human RPE, lipofuscin constitutes 20%–33% of the cells total cytoplasmic space, while in disease conditions such as geographic atrophy, there is found to be elevated amounts of lipofuscin accumulation directly adjacent to the area of disease.64,68 The presence of lipofuscin in RPE can be detected as early as 1 year of age, and has been shown to progressively increase with age. 69 A2E, a bisretinoid from the accumulation of all-trans retinal product of the visual processing cycle of the photoreceptors, is an abundant, specific component of lipofuscin useful for targeted molecular imaging.64,69,70 This bisretinoid is increased in disease and has been shown to disable RPE function through photo-oxidative damage, complement activation, and membrane degradation. 67 A2E is an intrinsically fluorescent protein that can be imaged by direct optical imaging at an excitation wavelength of 488 nm and an emission ranging from 565 to 725 nm. 69 On the apical side of the RPE, melanin, another intrinsically fluorescent protein, accumulates and can be used for fluorescence imaging. Melanin serves as a protective function against light scattering, radiation, oxidative stress, and photo-toxic damage.67,71 Near-infrared autofluoresence (NIA), with an excitation wavelength of 787 nm, is used to image melanin changes with an emission of >800 nm. 71 NIA shows less change with age as compared to lipofuscin and has a more widespread distribution, whereas lipofuscin has a more focal appearance at lesion sites. 71 Nonetheless, melanin-based NIA can provide some insight into RPE health since NIA decreases have been detected in genetic retinal degenerative diseases.71–73 To continue to implement autofluorescence imaging techniques in the clinic, it will be valuable to establish baseline and threshold autofluorescence levels (e.g., quantitative intensity values for a given optical imaging instrument) for standardized illumination and detection wavelengths with defined cohorts of patients and healthy controls to define uniform procedures. For example, spectral imaging has been utilized in a limited group of AMD patients to demonstrate that quantitative ratiometric imaging of Bruch's membrane autofluorescence, sub-RPE deposits, and lipofuscin using distinct illumination and detection settings may reveal disease-specific biomarker signatures, which may be useful in AMD diagnosis and monitoring. 74
Beyond autofluorescence imaging, several RPE-related molecular targets may warrant further consideration for development of clinical diagnostic approaches, including biomarkers of oxidative stress as discussed for RGCs, which have long been utilized in vitro in conjunction with microscopy to characterize RPE dysfunction and may be useful as in vivo imaging tools.75,76 Oxidative stress has been shown to contribute to many age-related diseases, such as AMD, and to light-induced damage of the RPE. 76 In vitro studies have shown that inhibiting mitochondrial electron transport chain action can reduce ROS and preserve the normal RPE phenotype. 76 This suggests that ROS may be a good early indicator of disease-related changes in the RPE. A key diagnostic target for RPE-related diseases, primarily AMD, may lie in the formation of drusen between Bruch's membrane and the RPE with aging and other factors. Drusen is an extracellular heterogeneous aggregation of proteins and lipids that form with age. Its accumulation is seen in almost all aged eyes; however, drusen can change in its appearance and is thought to be directly involved in AMD pathogenesis. Drusen is classified clinically by its size and appearance. Hard drusen is any drusen less than 63 μm in size, however, if it appears hard and flat in a fundus measurement, it can be up to 125 μm.77–79 Soft drusen is greater than 63 μm in size and can be further characterized as distinct and indistinct. Distinct soft drusen has a uniform density appearance, whereas indistinct appears to have decreasing density from the center outwards.77,79 Using size, number, and the extent of confluency of drusen, as determined by fundus imaging, risk can be determined for AMD pathogenesis.77–79
Drusen can be identified as areas of hyperfluorescence in a fluorescein angiogram and components of drusen may be a potential target for molecular imaging modalities, for possibly enhancing molecular characterization of AMD and identifying additional risk factors, for example, drusen types and components, which hasten transition from dry to wet AMD. Since drusen develops with age, it is thought that its accumulation could be an age-related deficit of RPE filtration. 79 Farkas et al. stated that some components of drusen include denatured mitochondria, cytoplasmic debris, pigment granules, and photoreceptor remnants.80,81 Additionally, esterified cholesterol and carbohydrate moieties such as N-acetylglucosamine and sialic acid have been identified in drusen, and might be targeted by small molecule synthetic probes. 78 Protein components that have been identified include ubiquitin, integrins, Tissue Inhibitors of Metalloproteinases, Advanced Glycation End-Product, and β amyloid, which might be targets for antibody-coupled imaging contrast agents. 78 Of equal potential for molecular imaging approaches involving RPE, complement system activation is altered, resulting in reduced cellular C-reactive protein-binding affinity, which disturbs extracellular RPE clearance, leading to build up of drusen. 82 These changes are all potential targets for molecular imaging probes, and may be beneficial for determining disease progression in AMD or identify areas of risk related to drusen. One major issue in developing probes to drusen components is the lack of animal models for testing. Dry AMD, which constitutes 85%–90% of AMD cases, is characterized by focal areas of soft drusen at the macula. 83 However, rodents do not have a macula and do not form focal regions of drusen build up. Wang and Neufield identified a potential animal model, the smoking mouse, which has similar components of drusen. 83 In the smoking mouse, drusen-like deposits can be found at 8 months in a more uniformly distributed pattern than the human drusen. 83 It is hoped that this model and others will be used to speed up the development of imaging probes for the molecular imaging of RPE. A major question to be addressed before advancing this line of investigation will be to examine contrast agent accessibility to RPE and drusen, and to evaluate classical measures of biodistribution and toxicity in an already compromised tissue microenvironment. Furthermore, as drusen characteristics (morphology, frequency) can be highly variable between patients, it may be difficult to establish quantitative thresholds to aid in diagnostic procedures, although efforts to standardize drusen detection, instrumentation, and imaging processing procedures have been reported. 84
Molecular Imaging of Endothelial Cells
Retinal and/or choroidal endothelial cell dysfunction occurs in a number of diseases, including retinopathy of prematurity, diabetic retinopathy, and choroidal neovascularization, all leading causes of blindness. In these diseases, endothelial cells participate in a number of changes, such as expression of inflammatory proteins and loss of tight junction molecules, which hold blood vessel linings together, as well as proliferation and migration to form abnormal neovascular structures (i.e., ocular angiogenesis). 85 Vascular leakage resulting from poor retinal endothelial barrier integrity and angiogenesis are significant retinal complications, and imaging techniques such as fluorescence angiography (FA), indocyanine green angiography (ICGA), and OCT are routinely used in the clinic to monitor these complications.86,87 However, these structural imaging techniques may often detect pathology only beyond subclinical disease stages, at which therapies might be more effective in preventing vision loss. Therefore, molecular imaging of endothelial cells could be utilized to identify molecular targets that are expressed in dysfunctional endothelial cells before advancement of complications and pathology.
Endothelial cell surface biomarkers of inflammation and/or angiogenesis are promising candidates for development of targeted contrast agents for ophthalmic imaging approaches, as these targets are accessible to injected contrast agents from the bloodstream and can be imaged in conjunction with FA or ICGA, thus integrating well into current ophthalmic imaging techniques. In addition, many such biomarkers are expressed focally on inflammatory endothelial cells and not adjacent, healthy endothelial cells, providing higher signal to noise. Furthermore, many of these targets have been extensively investigated using molecular imaging contrast agents in other fields, such as cardiovascular medicine and oncology. The C-C chemokine receptor 3 (CCR3) is a potentially important biomarker of choroidal neovascularization (CNV) in neovascular AMD, as demonstrated by CCR3 expression on choroidal neovascular endothelial cells in animal models and human CNV specimens.88,89 CCR3 binds to a number of chemokines and is typically associated with eosinophils, but in neovascular AMD receptor, expression was observed specifically on choroidal neovascular endothelial cells as detected in vivo using quantum dot nanocrystals linked to CCR3-targeted antibody fragments. Importantly, CCR3 imaging in the choroid revealed subclinical CNV at a stage before which it could be detected by FA, underscoring the power of molecular imaging to complement and enhance conventional ophthalmic imaging strategies. 88 Another useful target for imaging retinal vascular disease, endoglin (CD105), is an endothelial cell surface glycoprotein upregulated on proliferating endothelial cells in preretinal or choroidal neovascular lesions, and can be targeted using antibodies.90–93 Endoglin-targeted antibodies have already shown promise in targeting proliferating endothelial cells in animal models of laser-induced choroidal neovascularization as well as patient specimens ex vivo.94,95 Integrins such as αVβ3 have been successfully imaged in cardiovascular disease 96 and cancer,97–101 and should prove useful should they be investigated in retinal diseases using similar antibody and peptide-targeted approaches, due to the established role of integrins in retinal vascular biology. 102 The intercellular adhesion molecule 1 and the vascular cell adhesion molecule 1 (VCAM-1) can be targeted using a number of nanoparticle-, antibody-, and peptide-mediated approaches for vascular imaging in a number of diseases.103–106 Jayagopal et al. have developed fluorescent quantum dot nanocrystals conjugated to targeting antibodies or peptides to interrogate VCAM-1 expression and other proteins in mouse models of laser-induced choroidal neovascularization (Fig. 2) and other experimental models of disease, and imaging these targets with sufficient signal to noise is feasible in a number of approaches using magnetic resonance imaging (MRI), optical imaging, positron emission tomography, and radiography.107,108 VCAM-1 is an especially relevant target for imaging inflammation due to focally increased expression on inflammatory or neovascular endothelial cells, with lack of detectable surface expression on healthy or quiescent endothelial cells in diseases such as neovascular AMD and proliferative diabetic retinopathy.109,110 A limitation of endothelial cell-targeted imaging approaches is the inability of the currently used imaging probes for accessing intracellular endothelial targets. However, Jayagopal et al. have recently developed gold nanoparticles for imaging intracellular RNA biomarkers, such as mRNA and miRNA, in mammalian cells, 111 and are adapting their approach for imaging of RNA biomarkers in retinal endothelial cells in vivo. This approach may address limitations of current approaches such that currently inaccessible, but clinically relevant molecular targets can be interfaced for imaging and/or therapeutic purposes.

In vivo imaging of vascular cell adhesion molecule 1 (VCAM-1) expression in a mouse model of laser-induced choroidal neovascularization (LCNV) using custom VCAM-1 targeting peptides conjugated to quantum dot (QD) fluorescent semiconducting nanocrystals.
Several other endothelial cell-related targets in the retina are useful targets for direct or indirect molecular imaging, including hypoxic biomarkers, matrix metalloproteinases (MMPs), and tight junction molecules. Hypoxia is an important biomarker associated with ocular angiogenesis in a number of diseases. The deprivation of local tissue oxygen supply can be optically imaged either by targeting relevant biomarkers, such as carbonic anhydrases, using antibodies or small molecules related to sulfonamides,112,113 can be imaged indirectly by using novel spectral imaging techniques using phosphorescence lifetime-based imaging agents,114–118 or can be imaged in conjunction with fluorescent nitroimidazole derivatives. 119 Nitroimidazoles, such as pimonidazole, form adducts with intracellular proteins preferentially in hypoxic cells due to bioreduction with nitroreductases, causing their intracellular retention, subsequently enabling visualization of hypoxic cells with high signal to background ratios. MMPs are involved in remodeling of the tissue microenvironment, which enables cell migration in angiogenesis, among other functions, and a number of peptide-based probes have been developed to detect their function using optical imaging. In this approach, peptides containing a fluorophore and fluorophore-matched quencher are coupled on opposite ends of a short peptide, the sequence of which is engineered to be cleaved by (1) specific MMP member(s), thus resulting in fluorescence emission.120–123 This strategy has not been applicable to all MMP members due to lack of available specific cleavage peptide sequences, but the presence and absence of MMPs in the retina may be valuable for diagnosis and monitoring of angiogenesis in retinal neovascular diseases. 124 To image tight junction molecules, which are critical components of the blood–retinal barrier,125–127 established and emerging techniques are available for assessment of retinal vascular integrity via imaging of leakage. Several approaches, including vitreous fluorophotometry, FA, and dual tracer fluorescence angiography, use fluorescent tracers of varying molecular weight to monitor leakage in the retina, often using quantitative techniques.128–134 In addition, dynamic contrast-enhanced MRI has been adapted for similar analysis.135,136 By examining leakage of compounds of varying molecular weight, quantitative thresholding can be performed to quantify the extent of disease severity. However, these approaches are indirect imaging approaches examining surrogate endpoints underlying the blood–retinal barrier function, and approaches to image the loss of tight junction molecules directly in the retina may be useful for targeted drug development and diagnostic studies. It is important to note that many endothelial cell-targeted therapies described above are in development or in clinical usage, thus making possible combined imaging and therapy of retinal disease (theranostics).
Molecular Imaging of Leukocytes
Inflammation is thought to be a common component of most retinal diseases, including retinopathy, macular degeneration, glaucoma, and uveitis, as exhibited by cascades of molecular signaling pathways and leukocyte–endothelial–tissue interactions in these diseases. 137 As inflamed endothelial cells express surface proteins to recruit leukocytes to the sites of inflammation, which can be detected by molecular imaging as discussed above, much interest has also been directed toward imaging leukocytes and leukocyte subpopulations in retinal diseases as well. Early efforts for imaging leukocytes such as neutrophils in preclinical models of retinal inflammation have involved the DNA-intercalating dye acridine orange (AO), which is used to identify circulating leukocytes as hyperfluorescent dots in the retina, along with endothelial cell linings, using the SLO (Fig. 3).138–141 Studies incorporating AO fluorography of leukocytes have improved our understanding of complex spatiotemporal dynamics of leukocyte–endothelial interactions in retinal inflammatory diseases, but as AO is phototoxic and intercalates with nucleic acids within the cell, the dye is not suitable for clinical usage. 142 Efforts to image leukocyte subtypes are being investigated to allow thorough characterization of leukocyte populations in disease. Macrophages play an important role in diseases such as AMD and methods of detecting these cell types specifically have been clinically translated. Typical approaches are MRI- or optical imaging-based, and use lipoproteins, peptides, and/or antibodies to direct nanoparticles, such as superparamagnetic iron oxide particles, which are T2 MRI contrast agents, or fluorescent dyes to resident macrophages within blood vessels or tissue, as demonstrated by a number of studies involving atherosclerosis.107,143–146 Optical imaging of leukostasis through AO fluorography can be used for quantitative analysis (e.g., counting of arrested leukocytes), demonstrating that leukocyte imaging can be useful for standardized clinical diagnostic approaches.
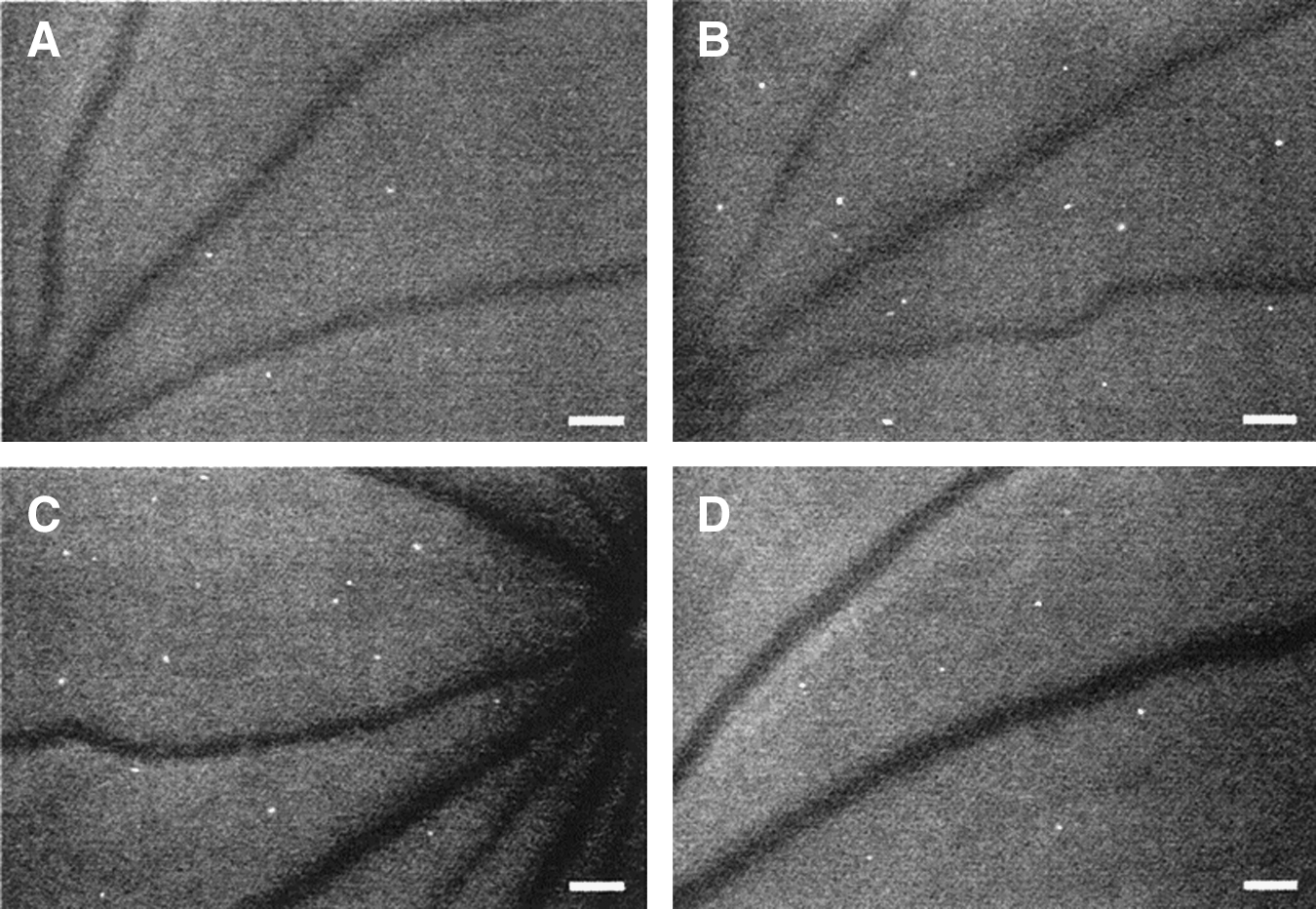
In vivo imaging of retinal leukostasis and therapeutic inhibition of leukostasis in mice using acridine orange (AO) fluorography. AO-stained leukocytes appear as hyperfluorescent white dots in the microvasculature.
Other approaches involve imaging of leukocytes using dye or nanocrystal-labeled antibodies or peptides, but the effects of these conjugates on the inflammatory response (i.e., contrast agent-induced dampening or exacerbating inflammation) have not been extensively investigated.107,108,147 Further development of biocompatible, inert imaging agents for imaging of leukocytes in vivo is warranted to enable detection of leukocyte–endothelial interactions, such as arrest, rolling, and transmigration, to develop new therapies and evaluate the effects of current therapies in the patient. Other circulating cell types of interest for imaging applications are endothelial progenitor cells (EPCs), which are thought to play important roles in vessel remodeling in angiogenesis or vessel injury in retinal diseases.148–153 EPC functions are still being elucidated and EPCs are being studied as therapies themselves or as targets for therapy. Therefore, development of targeting strategies similar to those used for leukocytes would be helpful in advancing preclinical and clinical studies involving EPC function. However, a potential limitation of these strategies may involve adverse activation of an already stimulated immune system via introduction of imaging probes and their interfacing with leukocytes and endothelial cell surface proteins. It will be important for clinical translation of leukocyte-directed imaging probes to judiciously select molecular imaging targets in conjunction with utilizing stealth or inert imaging probes to reduce the potential for such effects.
Conclusion
Through preclinical studies and emerging clinical applications, molecular imaging of the retina is poised to play an important role in disease diagnosis and monitoring, as well as assessment of therapeutic efficacy. Key considerations for improving clinical translation and incorporation of these imaging approaches will revolve around minimizing adverse effects of imaging agents, due to potential for off-target biodistribution and activation of the immune system, among many possibilities. Furthermore, imaging agents developed initially for preclinical investigations will need to be scaled up for clinical implementation using appropriate manufacturing and quality control practices used in the industry, which constitutes a major translational hurdle. Nevertheless, molecular imaging has revealed great insight into the mechanisms and mediators governing the retina in health and disease, and many of the technologies discussed in this work will likely evolve into powerful techniques in the ophthalmic practice.
Footnotes
Acknowledgments
This work was supported by the International Retinal Research Foundation, the American Health Assistance Foundation, a Core Grant in Vision Research from the National Institutes of Health (P30-EY008126), the American Diabetes Association and a departmental unrestricted grant from Research to Prevent Blindness.
Author Disclosure Statement
No competing financial interests exist.