
Abstract
Abstract
Purpose:
To evaluate long-term follow-up of the orally administered combination of flavonoids with Centella asiatica and Melilotus for treatment of diabetic cystoid macular edema (CME) without macular thickening.
Methods:
Seventy consecutive patients with type 2 diabetes and CME without macular thickening at optical coherence tomography (OCT) were prospectively and randomly enrolled in two groups of 35 subjects each (treatment and control groups). Patients in the treatment group were treated with an oral combination of diosmin (300 mg/day), with C. asiatica (15 mg/day) and Melilotus (160 mg/day). All patients underwent a complete ophthalmologic examination, OCT (Spectralis HRA-OCT), and central microperimetry (SD-SLO/OCT) at baseline, month 3, month 6, month 12, month 24, and month 36.
Results:
No differences in HbAc1 percentage, blood pressure, microalbuminuria, visual acuity, mean central retinal thickness, and stability of fixation were present between the two groups during follow up (p>0.05). Retinal sensitivity reduced in the control group only from month 6 until month 36 (p<0.001). In the treatment group, a greater retinal sensitivity was present at month 12, month 24, and month 36 (p=0.001). No side effects of treatment were observed.
Conclusion:
Oral administration of flavonoids, C. asiatica and Melilotus, in patients with CME without macular thickening provided preservation of retinal sensitivity during 36 months of follow up when compared with untreated patients.
Introduction
Methods
Seventy consecutive patients with type 2 diabetes and CME without macular thickening at OCT were prospectively and randomly enrolled in two groups of 35 subjects each (treatment and control groups). The study was approved by the ethics committee of the University Federico II of Naples and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Criteria for inclusion were absence of clinically significant macular edema at clinical examination, presence of non-ischemic CME, normal central retinal thickness (CRT) and normal foveal contour at OCT examination, and absence of any previous treatment for diabetic retinopathy in the 6 months preceding the first examination. Patients with coexisting ocular pathologies and significant media opacities that precluded fundus examination were excluded.
Patients in the treatment group were treated with an oral combination of diosmin (300 mg/day), C. asiatica (15 mg/day), and Melilotus (160 mg/day). An oral pill (VENOPLANT 20; Aesculapius Farmaceutici Srl Italia) containing the combination described earlier was given once daily during follow up. At each follow-up visit, patients were asked to report onset of other treatments and to confirm adhesion to protocol.
Data at baseline, month 3, month 6, month 12, month 24, and month 36 are presented.
At baseline and at each follow-up visit, all patients underwent a complete ophthalmic examination, including best-corrected visual acuity (BCVA) after refraction using the Early Treatment Diabetic Retinopathy Study (ETDRS) letters scale, slit-lamp examination, funduscopy and fundus photography, OCT, and central microperimetry. At baseline, fluorescein angiography was performed to exclude ischemic macular edema. At baseline and at each visit, mean value of glycosylated hemoglobin (HbA1c) and blood pressure were monitored. Normal range of HbA1c was considered between 4% and 6%. Blood hypertension was classified in normal tension (<120/80), pre-hypertension (120–139/80–89), stage 1 (140–159 systolic or 90–99 diastolic), and stage 2 (≥160 systolic or ≥100 diastolic). 10
To assess CRT, a spectral domain OCT device (Spectralis HRA-OCT; Heidelberg Engineering) was used. Active eye tracking of Spectralis OCT enables the system to have a precise automatic rescan function that places follow-up scans in precisely the same location as previous scans. CRT was considered the thickness in the central 1-mm disc, representing the foveal area. An upper limit of 270 μm for normal CRT was chosen according to the previously reported normal retinal thickness values as measured with Spectralis OCT. 11 Normal foveal contour was determined by the presence of a well-formed, U-shaped, foveal depression without marked steepening, flattening, or asymmetry. Intraretinal cysts were defined as well-circumscribed hyporeflective spaces within the fovea, measuring at least 10 μm in diameter.4,5,8 Fundus-related microperimetry was performed using SD-SLO/OCT (Ophthalmic Technologies Inc.). A 4-2-1 double-staircase strategy was used, and results were reported in decibels. The recorded fixation pattern was classified according to the Fujii classification. 12 Retinal sensitivity in the 8° central area and stability of fixation were measured at each visit.
Statistical analysis was performed using the Statistical Package for Social Sciences (version 17.0; SPSS Inc.). Repeated-measures analysis of variance (rANOVA) with Dunnett correction for multiple comparisons was used to compare intragroup and intergroup differences. Fisher exact test was used to compare the retinal sensitivity between eyes that showed an anatomical improvement and the control group at each follow-up visit. Results were considered significantly different if the p-value was<0.05.
Results
In the treatment group, the 35 patients (19 women, 16 men, 35 eyes) had a mean age of 64.8±3.6 years. In the control group, the 35 patients (21 women, 14 men, 35 eyes) had a mean age of 65.1±3.1 years. Characteristics of the 70 patients in the two groups at baseline are resumed in Table 1. No differences were present at baseline between the two groups with regard to sex, age, mean duration of diabetes, actual HbAc1 percentage and HbAc1 percentage in the last 5 years, microalbuminuria, and blood pressure.
SD, standard deviation; HbA1c, glycosylated hemoglobin.
No patient was lost to follow up. No statistically significant differences were found during follow up between the two groups with regard to HbAc1 percentage, blood pressure, and microalbuminuria (Table 2). Side effects of treatment during follow up were not observed.
BCVA, best corrected visual acuity; ETDRS, Early Treatment Diabetic Retinopathy Study; CRT, central retinal thickness; MP, microperimetry; HbA1c, glycosylated hemoglobin; Δp, statistical significance compared with baseline; Δ2p, statistical significance compared with the treatment group.
In the treated group, a reduction of mean retinal sensitivity was found during follow up, although it was not significant (p>0.05 at month 3, month 6, month 12, month 24, and month 36). On the other hand, BCVA slightly increased at month-12 and at month-24 visit (p>0.05), and returned to baseline values at month-36 visit. Intraretinal cysts were always localized in the central 3 mm ETDRS ring, in the inner nuclear layer in 31 cases (88.6%), and in the outer nuclear layer in 4 cases (11.4%). Disappearance of the retinal cysts was noticed in 7 out of 35 eyes (20%) after a mean period of 3.1±0.4 months, and persisted during follow-up (Fig. 1). When compared with control group, these 7 eyes showed no statistically different mean BCVA (75.50±3.7 ETDRS letters at baseline, p=0.8; 75.09±3.5 ETDRS letters at month 3, p=0.8; 75.61±3.1 ETDRS letters at month 6, p=0.6; 75.51±4.5 ETDRS letters at month 12, p=0.6; 75.38±4.1 ETDRS letters at month 24, p=0.5; 75.10±3.1 ETDRS letters at month 36, p=0.6) and a greater mean retinal sensitivity (16.12±0.25 dB at baseline, p=0.8; 16.41±0.32 dB at month 3, p=0.02; 16.40±0.37 dB at month 6, p=0.01; 16.61±0.31 dB at month 12, p=0.01; 16.65±0.40 dB at month 24, p=0.01; 16.63±0.32 dB at month 36, p=0.01). In the remaining 28 eyes (80%), BCVA, CRT, and retinal sensitivity did not show any significant change during follow up (p>0.05).
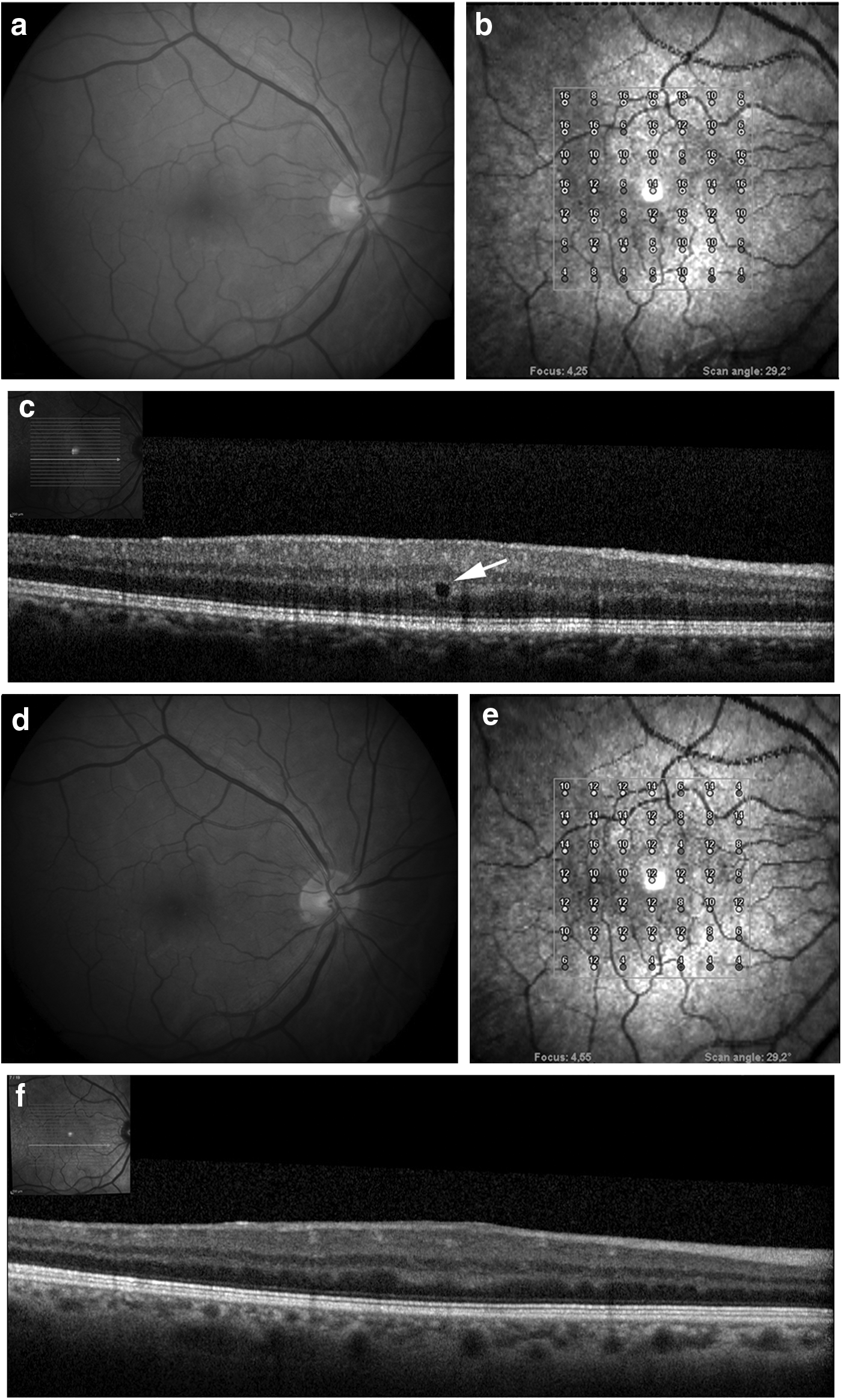
Diabetic macular edema without retinal thickening.
In the control group, stabilization of BCVA and CRT was present in 27 eyes (77.1%), worsening in 8 eyes (22.9%, p>0.05); while improvement was not observed. A reduction of mean retinal sensitivity was observed (p=0.08 at month 3 and p<0.001 at month 6, at month 12, at month 24, and at month 36).
Overall, no differences in BCVA, mean CRT, and stability of fixation were present between the two groups during follow up (p>0.05); while in the treatment group, a greater retinal sensitivity was present at month 12, at month 24, and at month 36 (p=0.001).
Discussion
Administration of flavonoids, C. asiatica, and Melilotus for diabetic macular edema without macular thickening has been previously suggested to improve macular edema and preserve retinal sensitivity in the short-term follow up. 9 In this study, the beneficial effects of such a combination in the absence of side effects were confirmed during 36 months of follow up. CME without macular thickening has been recently reported in 5.6% of eyes of 653 patients affected by different retinal pathologies. Micronized purified flavonoid fraction has been shown to reduce symptoms of pain, heaviness, and edema in patients with venous reflux in the prospective controlled multicentric RELIEF (Reflux assEssment and quaLity of lIfe improvEment with micronized Flavonoids) Study.13,14 Taken for 3 months at an early stage of diabetic retinopathy, pycnogenol, a flavonoid-rich dietary supplement, has been shown to enhance retinal blood circulation and to induce regression of edema, which favorably improves vision of patients. 15
While BCVA and fixation did not show significant changes in both groups, a significant reduction of retinal sensitivity was observed in the control group; while reduction in the treatment group was not significant. Overall, a significantly greater reduction of retinal sensitivity was found in the untreated group at month 12, month 24, and month 36. No significant differences were observed between the two groups with regard to changes in HbAc1 percentage, microalbuminuria, and blood pressure during follow up. According to these data, we may speculate that the functional preservation in the treated group could reflect the beneficial effects of the treatment. Flavonoids have also been used after retinal vein occlusion and have shown beneficial effects on visual acuity, retinal circulation times, and macular edema, 16 due to their effects on endothelial cell function, on release of fibrinolitic agents6,13,14 and to anti-VEGF effect. 17
Intraretinal cysts were localized in the inner nuclear layer (88.6%) and in the outer nuclear layer (11.4%). Increased permeability of the inner hemato-retinal barrier could be responsible for localization in the inner retina, 18 while localization in the outer retinal could be due to increased permeability of the outer hemato-retinal barrier. Large outer nuclear layer cysts and subretinal fluid accumulation appear relatively late in diabetic macular edema, and are likely responsible for reduction of retinal function after photoreceptors and inner segment/outer segment junction damage. 19
In this study, a Spectralis OCT device was used. Active eye tracking of Spectralis OCT enables the system to have a precise automatic rescan function that places follow-up scans in precisely the same location as previous scans. By this method, an exact evaluation of changes in intraretinal cysts was possible. In 7 out of 35 treated eyes (20%), disappearance of intraretinal cysts was noticed during follow up, while such an improvement was not observed in the control group. As previously suggested, the beneficial effects on retinal sensitivity and the disappearance of intraretinal cysts could be related to the combination of anti-inflammatory effect and the reduction of endothelial cell permeability. 9
Despite worsening of retinal sensitivity in the untreated group, BCVA and retinal fixation were stable in both groups. BCVA and fixation depend on the foveal area, while microperimetry tests sensitivity in a larger area surrounding the fovea. Therefore, focal macular changes could likely affect macular sensitivity, leaving BCVA and fixation unchanged in the long term. Diabetic macular edema without retinal thickening is characterized by focal alterations in an otherwise normal macular area. Focal alterations may determine a reduction of light sensitivity more than diffuse edema,20,21 as they block the light from photoreceptors even before establishment of a structural damage to the retina. Microperimetry of eyes with CME without macular thickening could, therefore, be considered a reliable method to assess functional changes during follow up.
A limitation of this study is the relatively small sample size in the two groups, mainly due to the prospective design. On the other hand, major strengths are the prospective nature, standardization of data collection, length of follow up, and high rate of follow-up visits.
In conclusion, oral administration of flavonoids, C. asiatica, and Melilotus in patients with CME without macular thickening provided preservation of retinal sensitivity during 36 months of follow up when compared with untreated patients. Such a combination could be considered a valid therapeutical option to stabilize retinal function in these cases.
Footnotes
Author Disclosure Statement
No competing financial interests exist.