
Abstract
Abstract
Purpose:
To compare tissue distribution of dye-drug surrogates after intravitreal (IVT) and suprachoroidal (SCS) delivery to determine the influence of drug lipophilicity and choroidal circulation.
Methods:
Thirty-two pig eyes were collected immediately after euthanasia. Sixteen eyes were perfused for 30 min through one long posterior ciliary artery with nondye containing nutrient media. An IVT or SCS injection was performed with either a 100 μL balanced salt solution (BSS, n=8), 1% sodium fluorescein (NaF, n=12) or 0.12% lipophilic carbocyanine dye (DiI, n=12). Globes were maintained at 37°C for 15 min, and then snap-frozen and dissected. Aqueous extraction and measurement of NaF or DiI concentration was performed using spectrophotometry and spectrofluorometry, respectively.
Results:
After SCS delivery of NaF scleral, iris-ciliary body, choroidal and vitreous dye levels were higher in nonperfused eyes compared to perfused eyes. After DiI SCS or IVT delivery, no significant differences were found in dye tissue concentrations in perfused eyes compared to nonperfused eyes. Following perfusion, a better and even drug distribution was found in the retinal pigmented epithelium (RPE)-choroid following IVT and SCS delivery of the hydrophilic drug and after IVT injection of the lipophilic drug compared to nonperfused eyes.
Conclusions:
Choroidal circulation reduces the tissue drug concentration of the hydrophilic drug suggesting an early clearance mechanism after SCS delivery. SCS injections of lipid and hydrophilic drugs allowed direct drug delivery to the retina and RPE-choroid with limited exposition to the anterior segment.
Introduction
Topical drug delivery does not efficiently reach the posterior segment of the eye and ocular delivery of intravenous drugs is limited by the blood–retinal barriers or toxic systemic doses. 4 Although intravitreal (IVT) injection may deliver adequate drug levels to the retina, repeated injections are associated with complications such as retinal detachment, endophthalmitis, cataracts, and increased intraocular pressure.2,3,5,6 Transscleral delivery of ocular drugs may avoid complications associated with an intraocular injection; however, its main limitations are the poor targeting and the limited diffusion of large biological agents. 7
The suprachoroidal space (SCS) is a potential space located between the sclera and the choroid that is limited anteriorly in the region of the scleral spur and posteriorly by the transscleral connections of the short posterior ciliary vessels to the choroid.8–10 The SCS can expand to accommodate a fluid or drug formulation and has become a recent focus of ocular drug delivery research.6,11 Anatomically, there are several advantages of the SCS for drug delivery. The location of the SCS adjacent to the target site may provide adequate drug concentration in the desired tissues limiting exposure to other regions of the eye, while at the same time avoiding major drug barriers such as the sclera and conjunctival blood vessels and lymphatics.3,7,9,12–14
Understanding the ocular barriers and clearance mechanisms involved in SCS drug delivery is essential to determine the pharmacokinetics of various classification of medications. Barriers to drug delivery have been described as static, metabolic, and dynamic.4,15 With SCS drug delivery, static barriers would include porous tissues of the choroid, interfibrillar spaces in the Bruch's membrane, tight junctions in the retinal pigmented epithelium (RPE), and the intercellular spaces of the retina. 16 Dynamic barriers include drug clearance mechanisms through choroidal circulation and active transport in the RPE. Finally, metabolic barriers reduce drug penetration to the retina by promoting drug degradation mainly in the RPE. 17
The permeability of Bruch's membrane, the choroid, and the RPE have been extensively studied. 5 The choroidal stroma does not seem to play much of a role in static barrier function. It has numerous fenestrations, pinocytotic vesicles, and a lack of tight junctions, thus allowing for relatively easy movement of substances. 17 However, the effect of choroidal circulation as a dynamic drug barrier is not well understood, because of the difficulty of isolating choroidal circulation in experimental systems. The choroid, due to its high blood perfusion serves as a sink in which the drug concentration is assumed to be zero in some of the models of ocular drug transport.18,19 Furthermore, the difference in osmotic pressure between the vitreous and the choroid and the difference in hydrostatic pressure between the suprachoroid and the episcleral tissue generate outward bulk fluid flow. 20
The purpose of this study is to evaluate the effect of choroidal circulation and drug lipophilicity on ocular tissue concentrations after SCS delivery compared to IVT drug delivery. As a model system, we used an arterially perfused ex vivo porcine model, a well described model that has been used for the measurement of metabolic, drug delivery and pharmacokinetic parameters in ocular studies.21–23 This model retains the dynamics of blood flow; therefore, it allows the study of the choroidal circulation and its effects in drug distribution and clearance mechanisms after suprachoroidal drug delivery.
Methods
Ex vivo arterially perfused pig eyes
Use of animals in this study adhered to the ARVO Statement for the Use of Animals in Ophthalmic and Visual Research and was approved and monitored by the North Carolina State University Institutional Animal Care and Use Committee. Thirty-two pig eyes of either sex were collected immediately after euthanasia, placed on ice, trimmed of excess adnexal tissue, and within 15 min of euthanasia, were prepared for perfusion. Sixteen eyes were arterially perfused according to the method described previously.23,24 Briefly, a long posterior ciliary artery was identified and cannulated using a 27 gauge cannula (Anterior Chamber Cannula; Oasis, Glendora, CA). Cyano-acrylate tissue adhesive (Pacer Technology, Rancho Cucamonga, CA) was used to fixate the cannula to the external sclera. Eyes were perfused with nondye containing tissue culture media (Dulbecco's phosphate-buffered saline; Mediatech, Inc, Manassas VA). The perfusion solution was saturated with oxygen by bubbling it with 95% oxygen and 5% carbon dioxide, while being stirred for 30 min before perfusion and oxygenation of the media continued throughout the experiment. Perfusion was started at a flow rate ∼0.25–0.8 mL/min using a peristaltic pump (Mini-Pump; Control Company, Friendswood, TX). Adequate arterial perfusion was determined by observing flow of media exiting vortex veins.
Perfused (n=16) and nonperfused eyes (n=16) were then placed with the cornea facing upward in a custom-made perfusion chamber resembling a jacket-heated beaker in a water bath at 37°C (Isotemp; Fisher Scientific, Suwanee, GA). During the entire process, eyes were kept moist with a balanced salt solution (BSS; Alcon Laboratories, Fort Worth, TX) by applying 50 μL to the corneal surface approximately every 2 min.
Fluorescence microscopy of choroidal perfusion
To visualize and confirm the adequate perfusion of the choriocapillaris in eye receiving arterial perfusion, 2 eyes were arterially perfused (same conditions as previously described) with a solution of 0.12% lipophilic carbocyanine dye (DiI; AnaSpec Campus Drive, Fremont, CA). Globes were then dissected and a flat mount of the choroid was created. Images of the choroid were taken with a fluorescence microscope using a rhodamine filter set (Leica Microsystems, Inc., Buffalo Grove, IL).
IVT and SCS injections
Perfused and nonperfused eyes had IVT and SCS injections performed according to the following schedule:
Control
(n=8): 4 perfused eyes, 4 nonperfused eyes. An IVT or SCS injection was performed using 100 μL of BSS.
Sodium fluorescein (NaF)
(n=12): 6 perfused eyes and 6 nonperfused eyes. An IVT or SCS injection was performed with 100 μL 1% sodium fluorescein (Akorn, Inc., Lake Forest, IL).
DiI
(n=12): 6 perfused eyes and 6 nonperfused eyes. In this group, an IVT or SCS injection was performed with 100 μL of 0.12% DiI.
IVT injections
Hundred microliters of the selected dye or BSS was injected into the center of the vitreous body using a 27 gauge needle (Kendall, Mansfield, MA), through a superior pars plana injection located 5 mm posterior to the limbus.
SCS delivery
A 2-mm full-thickness scleral incision was made 5 mm posterior to the superior limbus to expose the SCS. A 27 gauge cannula (Anterior Chamber Cannula; BD Visitec, Waltham, MA) was placed 1 mm into the SCS through the scleral incision with the opening of the cannula directed posteriorly. The cannula was removed 10 s after the injection, which allowed for the material to dissect into the tissue planes before the cannula was removed.
Fifteen minutes after injection, all globes were snap-frozen by placing them into liquid nitrogen and stored at −80°C until processing.
Eye dissection, tissue processing, and analysis
After injections, frozen eyes were dissected on a cooled ceramic tile placed on dry ice and 2-methylbutane (Sigma-Aldrich, St. Louis, MO), to avoid thawing of the globe during dissection. Each globe was sectioned longitudinally along the visual axis to divide the eye into 2 parts: the injected side (superior) and the opposite side (inferior). The cornea, aqueous humor, lens, iris-ciliary body (ICB), vitreous, neuroretina, RPE-choroid, and sclera were collected from each ocular section. To prevent transfer of drugs between tissues, the surgical instruments were rinsed with phosphate-buffered saline (PBS; Trevigen, Gaithersburg, MD) followed by methanol (Fisher Scientific, Fair Lawn, NJ), followed by PBS and blotted dry. All the samples were weighed and stored at −80°C until further processing.
NaF group
Ocular tissues were allowed to thaw at room temperature, and then mixed with 1 mL of PBS (pH 7.4) and vortexed for 10 min. Tissues were then homogenized using a hand homogenizer (Fisher Scientific, Suwanee, GA) in an ice bath. The aqueous layer was separated from the tissue matrix by centrifugation at 10,000g for 10 min and the supernatant was analyzed using spectrophotometry and a 96-well plate (Costar, Corning, NY). A standard solution of NaF was prepared in PBS with a concentration range of 30 μg/mL to 0.12 μg/mL. Fluorescence was determined in a spectrophotometer (Versamax Microplate reader, Sunnyvale, CA) at excitation and emission wavelengths of 530 and 590 nm, respectively.
DiI group
Thawed ocular tissues were mixed with 1 mL of isopropanol (Acros Organics, Morris Plains, NJ) and the tubes were shaken on an orbital shaker (Fisher Scientific, Suwanee, GA) for 15 min. The aqueous layer was then separated from the tissue matrix by centrifugation at 10,000g for 10 min and the supernatant was analyzed using spectrofluorometry and a 96-well plate. A standard solution of DiI was prepared in isopropanol with a concentration range of 3 μg/mL to 5 ng/mL. Fluorescence was determined using a spectrofluorometer (Flouroskan Ascent Fl, Helsinki, Finland) at excitation and emission wavelengths of 530 and 590 nm, respectively.
Concentrations of the dye (NaF and DiI) were reported as μg of dye per gram of tissue.
Data and statistical analysis
A Shapiro–Wilk normality test was done to confirm tissue dye concentration values followed a normal distribution. Mean dye tissue concentrations were compared using a 1-way ANOVA with the Tukey's post hoc analysis method. Differences were considered significant at P<0.05. Results and probabilities were calculated using computerized statistical software (JMP 10; SAS, Inc., Cary, NC).
Results
Fluorescence microscopy of choroidal perfusion
Following arterial perfusion, fluorescence microscopy showed that the choroid preserved the normal plexus structure with a complete perfusion of the capillary choroidal network (Fig. 1).

Fluorescent photomicrography (×20). Following arterial perfusion with a solution of DiI, the capillaries of the choriocapillaris appear as a well-perfused continuous meshwork with intervascular spaces denoted as columns or septa.
Dye tissue concentrations—nonperfused versus perfused eyes
Control group
No dye concentration was detected in any tissue either after IVT or SCS delivery in both perfused and nonperfused eyes (data not shown).
NaF group
(Table 1) In nonperfused eyes injected intravitreally, there was significantly higher NaF concentration in the vitreous, neuroretina, and RPE-choroid (P<0.001) compared to all other ocular tissues. Following SCS drug delivery in nonperfused eyes, there was a significantly higher NaF concentration in the RPE-choroid and sclera (P<0.01) than in all other ocular tissues.
Data are expressed as mean±SD (n=3).
P<0.05 significant differences nonperfused versus perfused eyes.
NaF, sodium fluorescein; IVT, intravitreal; SCS, suprachoroidal space; ICB, iris-ciliary body; RPE, retinal pigmented epithelium; SD, standard deviation.
In perfused eyes following IVT injections, there was a significantly higher NaF concentration in the vitreous and neuroretina (P<0.001) compared to all other ocular tissues (Table 1). After SCS drug delivery in perfused eyes, there was a significantly higher NaF concentration in the RPE-choroid (P=0.01) compared to all other ocular tissues.
When comparing tissues in perfused versus nonperfused eyes, in eyes injected intravitreally, there were no significant differences in the NaF concentration in any tissue studied. However, following SCS injections, there were significantly lower NaF concentrations in ICB (P<0.03), RPE-choroid (P<0.04), vitreous (P<0.03), and sclera (P<0.03) in the perfused eyes compared to the respective tissues in the nonperfused eyes.
DiI group
(Table 1) Following IVT injection in the nonperfused eyes, there was a significantly higher DiI concentration in the vitreous (P<0.001) compared to all other ocular tissues, and following SCS DiI delivery in the nonperfused eyes, there was a significantly higher concentration of DiI in the RPE-choroid compared to all other tissues (P<0.001).
In perfused eyes injected IVT, there was a significantly higher DiI concentration in the vitreous and sclera (P<0.015) compared to all other ocular tissues, and following SCS DiI delivery in the perfused eyes, there was a significantly higher concentration of DiI in the RPE-choroid compared to all other tissues (P<0.001).
When comparing perfused and nonperfused ocular tissues, there were no significant differences between DiI concentrations after either IVT or SCS injection.
Effect of choroidal circulation on drug distribution
To study the effect of the choroidal circulation on the drug distribution from the injected area (superior) to the inferior area (noninjected area), we compared the dye concentration between the superior and inferior sections of the eye. (Table 2)
Data are expressed as mean±SD (n=3).
P<0.05 significant differences superior versus inferior sections.
NaF group
In nonperfused eyes injected intravitreally, significantly higher NaF concentrations were found in the superior vitreous (P=0.007), superior RPE-choroid (P=0.03), and superior retina (P=0.0012) compared to the inferior sections. In perfused eyes injected IVT, significantly higher NaF concentrations were found in the superior vitreous (P=0.02) and retina (P=0.03) than in the inferior sections.
Following NaF SCS delivery in nonperfused eyes, significantly higher NaF concentrations were measured in the superior RPE-choroid (P=0.0015) and retina (P<0.001) compared to the inferior sections. However, in the perfused eyes, no significant differences in superior and inferior NaF concentrations were found in any tissue.
DiI group
In the nonperfused eyes injected intravitreally, significantly higher DiI concentrations were measured in the superior vitreous (P=0.0019), superior RPE-choroid (P=0.04), and superior sclera (P=0.01) than in the inferior sections. In perfused eyes, significantly higher DiI concentrations were measured in the superior vitreous (P=0.0023) and sclera (P=0.04) compared to the inferior sections.
Following SCS delivery in the nonperfused eyes, there were significantly higher DiI concentrations in the superior vitreous (P=0.02), superior RPE-choroid (P=0.016), and superior sclera (P<0.0001) than in the inferior sections. However, when the DiI concentrations were measured in perfused eyes, significantly higher DiI concentrations were observed in superior RPE-choroid (P=0.0023) and sclera (P=0.04) compared to the inferior sections.
Comparison of retina and RPE-choroid concentrations
Because the targeted tissues in the treatment of posterior segment disease are commonly the retina and choroid, we compared dye concentrations in these tissues after IVT and SCS injection in perfused eyes.
NaF group
In the perfused eyes, there were significantly higher retinal NaF concentrations after IVT injections compared to SCS delivery in both superior (P=0.01) and inferior retinal tissue (P=0.03). However, in the RPE-choroidal tissue, there were no significant differences between the eyes injected IVT and into the SCS in both superior and inferior sections. (Fig. 2)
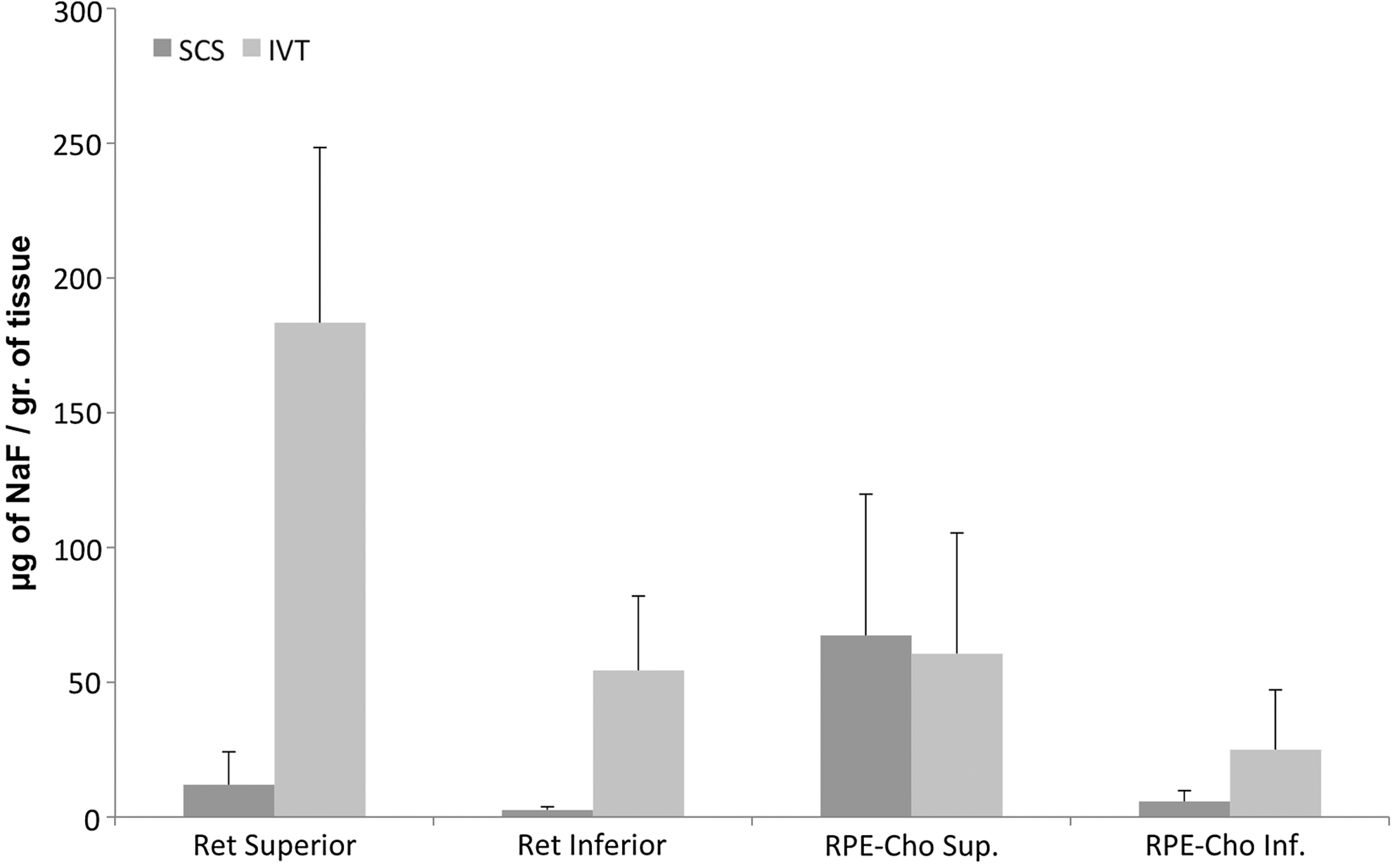
Retinal and retinal pigmented epithelium (RPE)-choroid sodium fluorescein concentrations (μg of NaF/gram of tissue) following intravitreal (IVT) and suprachoroidal space (SCS) injections in perfused eyes. IVT injection of NaF showed significantly higher retinal concentrations compared to SCS injection in both superior and inferior sections.
DiI group
In the perfused eyes, there were no significant differences in the retinal DiI concentrations between the eyes injected IVT or into the SCS in both superior and inferior sections. However, the RPE-choroid DiI concentration was significantly higher in eyes injected into the SCS compared to the IVT injections in both superior (P=0.0023) and inferior sections (P=0.0065). (Fig. 3)

Dye tissue concentrations (μg of DiI/gram of tissue) following IVT and SCS injections in perfused eyes. There were significantly higher RPE-choroid concentrations after SCS injections compared to IVT delivery in both superior and inferior sections.
Exposure of the anterior segment to dye
To study the anterior segment exposure to dye after SCS and IVT injections, dye concentrations were evaluated in the cornea, aqueous humor, lens, and ICB.
NaF group
In perfused eyes, there was a significantly higher NaF concentration in the ICB in eyes injected IVT compared to SCS (P<0.009). (Fig. 4)
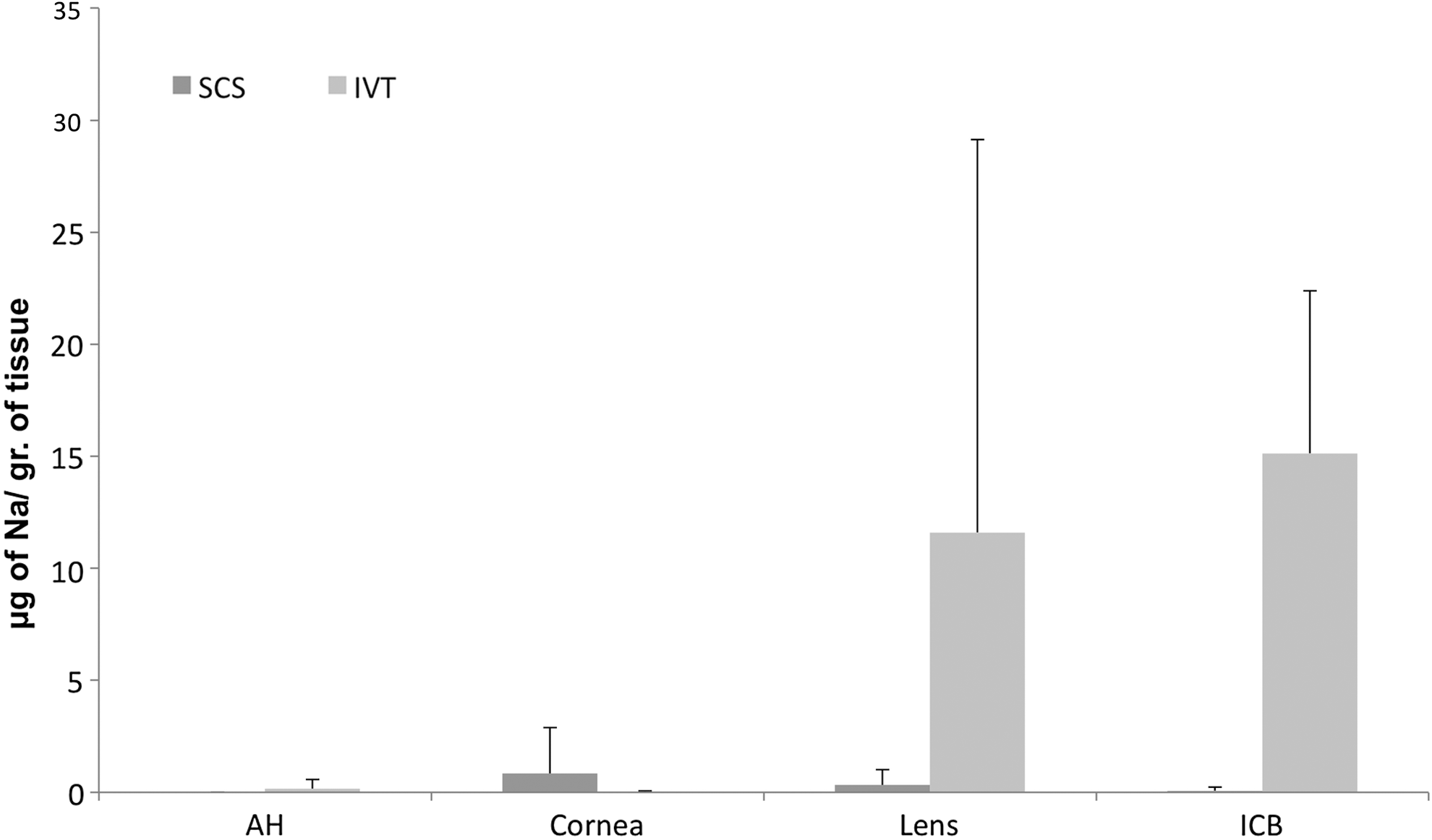
Anterior segment NaF concentrations (μg of NaF/gram of tissue) following IVT and SCS injections in perfused eyes. Intravitreal injection of NaF showed significantly higher NaF concentrations in the iris/ciliary body in eyes injected IVT compared to SCS delivery.
DiI group
In perfused eyes injected intravitreally, a significantly higher DiI concentration was observed in the lens (P<0.0217) and cornea (P<0.01) compared to SCS delivery. (Fig. 5).
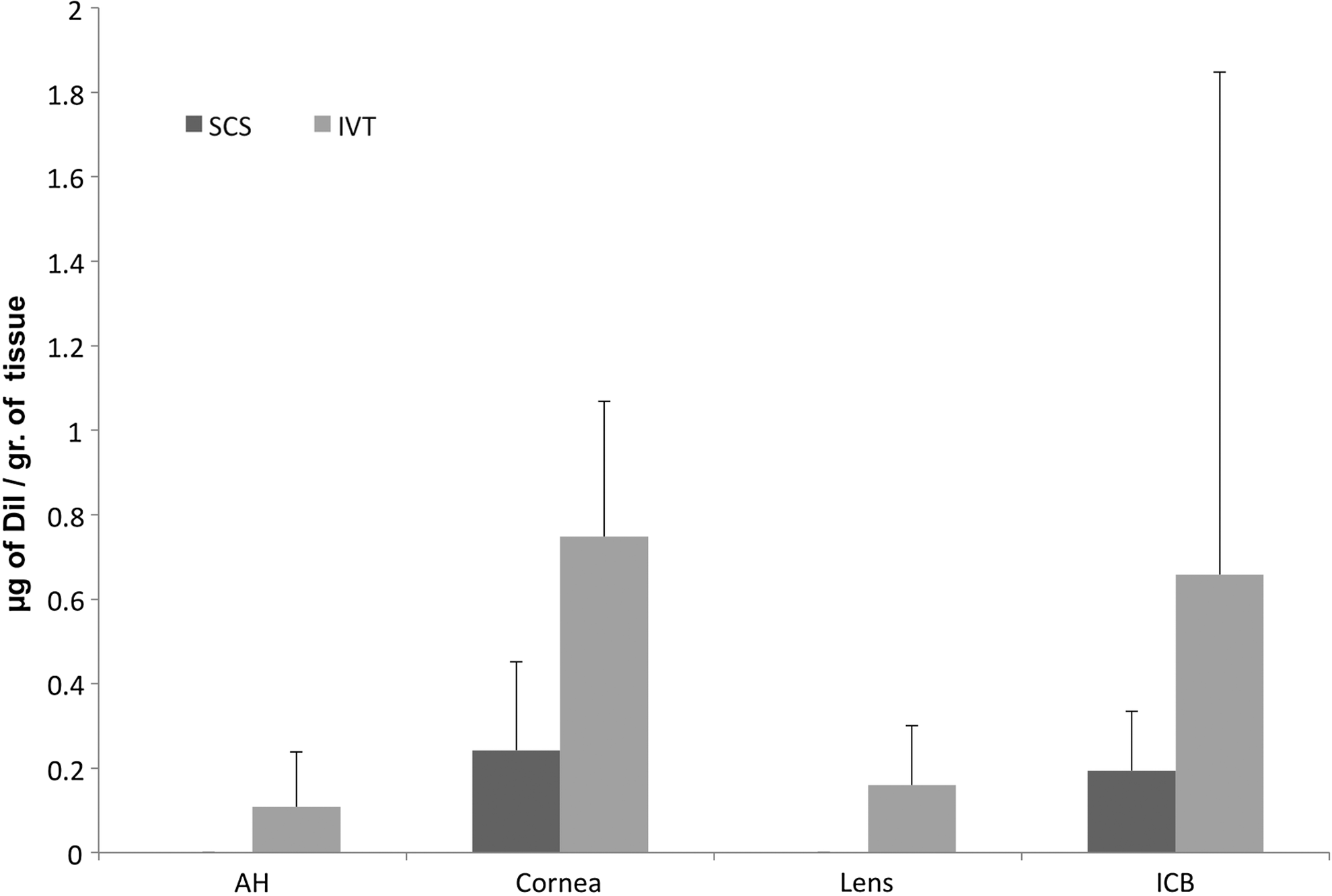
Dye tissue concentrations (μg of DiI/gram of tissue) following IVT and SCS injections in perfused eyes. In perfused eyes injected intravitreally, significantly higher DiI concentrations were observed in the lens and cornea compared to SCS delivery.
Discussion
SCS drug delivery has been identified as a potentially effective method to treat posterior segment eye diseases.3,7 This route of therapy may offer the ability to target the choroid and retina by delivering the drug adjacent to the choroid; however, it involves several tissue-related barriers and elimination factors.5,17,18,25 Specifically, the relative contribution of the role of choroidal blood flow as clearance mechanism is not completely understood.5,26
To evaluate the selective role of the different factors involved in drug clearance, Robinson et al. 26 applied cryotherapy to treat the choroid in a rabbit model. Four weeks after cryotherapy, a chorioretinal scar developed with theoretic obliteration of the choroid and retinal vasculature. 26 With the selective elimination of conjunctival lymphatic/blood vessels and/or the choroid circulation, they evaluated vitreous drug levels following sub-Tenon's injection of triamcinolone acetonide. Vitreal drug levels were not higher in rabbits that received cryotherapy as compared to those with an intact choroidal blood flow, which suggested that the choroidal flow does not contribute significantly to drug elimination during transscleral delivery. 26 In this model, the normal choroidal-retinal anatomy is disrupted focally in the superotemporal quadrant. In our work, we used the arterially perfused model, which allowed us to individually isolate choroidal circulation, while maintaining the normal integrity of the neuroretina, RPE, and choriocapillaris as shown in Figure 1.
To evaluate the effect of choroidal vascular circulation on drug diffusion, we compared the tissue dye concentration between perfused and nonperfused eyes. Significantly, lower ICB, RPE-choroid, vitreous, and sclera NaF tissue concentrations were found in the perfused eyes compared to nonperfused eyes suggesting that the hydrophilic NaF injected into the SCS is rapidly cleared by the choroidal circulation. Although it has been described that the choroidal tissue fluid can leave the eye through the sclera, either in or around perivascular spaces, posterior studies in vivo using hydrophilic contrast agents and magnetic resonance imaging have shown that after IVT implants, the hydrophilic contrast is mainly eliminated through the choroidal circulation as found in our study after SCS delivery.18,20 In contrast, we did not find differences in tissue dye concentrations in nonperfused eyes compared to perfused eyes following NaF delivered intravitreally or with the lipophilic IVT or SCS DiI injections.
We also evaluated the effect of choroidal circulation on drug distribution from the superior to the inferior section of the posterior segment. Mains et al. 27 studied the ability of time-of-flight secondary ion mass spectrometry to characterize the spatial distribution of dexamethasone within ocular tissues 1 h after IVT injection in perfused versus nonperfused ovine eyes. They found a better drug distribution in perfused eyes and concluded that the drug movement is not caused solely by diffusion, but also by circulation systems operating within the eye. 27 In our work, we did not detect differences in the vitreous dye distribution between perfused and nonperfused eyes. However, after perfusion, we found a better dye distribution through the RPE-choroid in both lipophilic and hydrophilic dyes injected intravitreally suggesting that choroidal circulation may improve drug distribution throughout the RPE-choroid after IVT injections.
Following SCS injection of the hydrophilic dye in perfused eyes, we observed a more even distribution between the superior and inferior ocular sections. In contrast, SCS injection of the lipophilic drug showed regional differences in distribution, with drug levels being higher on the dosed side than the opposite side for the RPE-choroid in both perfused and nonperfused eyes. As studied in transscleral delivery, drug molecules entering the SCS space may move directly in the direction of the choroidal stroma and retina, but may also move in a lateral direction or remain bound to components of the choroidal stroma.28,29 Our results may suggest that the lipophilic drug delivered in the SCS remains bound to components of the choroidal stroma, which is in line with previous studies that studied the influence of drug lipophilicity and the choroid-Bruch's layer in human, bovine, porcine, rabbit, and rat in vitro models.5,30 The choroid-Bruch's layer was found to bind lipophilic drugs preferentially and it is a greater barrier for the transport of lipophilic molecules toward the retina, possibly due to the presence of melanin and lipid plasma membranes of the endothelial cells.5,31
To evaluate the posterior segment targeting ability of SCS drug delivery, we studied distribution of IVT versus SCS delivery in perfused eyes. First, we analyzed the dye concentrations in the target tissues, and finally, the dye exposure to the anterior segment. We observed a significantly higher concentration of the hydrophilic NaF in the retina following IVT injection compared to the SCS delivery. Tyagi et al. 32 studied in vivo the distribution of NaF following SCS, IVT, and subconjunctival using ocular fluorophotometry. Contrary to our observations, NaF dye concentrations in the choroid-retina were significantly higher 2 min after suprachoroidal injection when compared to IVT injection in rats. 32 These differences can be explained, in part, by the extreme differences in the ocular size between the rat and pig (with the pig more similar in size to the human eye), 33 the different techniques used (spectrophotometry vs. noninvasive fluorophotomery), and the specific tissue studied. In our study, the retinal and RPE-choroidal tissue were studied individually, whereas in Tyagi's work, both tissues were analyzed together. Finally, Tyagi's article used an in vivo model, whereas in our work, we used an arterially perfused ex vivo model. Previous studies in NaF and carboxyfluorescein permeabilities of isolated dog, rabbit, and bovine RPE-choroid have shown that retina to choroid (outward) permeability was significantly larger than choroid to retina (inward) permeability at RPE-choroid, suggesting an active transport across RPE from the retina to the choroid.2,34–36
Regarding the lipophilic dye, we observed a significantly higher concentration of DiI in the RPE-choroid following SCS injection compared to the IVT delivery. One of the greatest advantages described of the suprachoroidal injection is the ability to deliver large amounts of drug to the choroid and Bruch's membrane. This could be particularly relevant to the treatment of AMD, since the thickening of Bruch's membrane and drusen formation are some of the earliest events in the pathogenesis of the disease. 37 Lipophilic and positively charged solutes may form a slow release depot in the choroid-Bruch's layer; however, if the retina is the intended target, there is a further reduction in lipophilic drug transport because of the presence of the choroid- Bruch's membrane and RPE. 5
After IVT injections, a significantly higher dye concentration was detected in the lens and cornea for the lipophilic drug and in the ICB for the hydrophilic drug compared to the same dye injected suprachoroidally. Patel et al. studied the targeting ability of the SCS compared to IVT injections using NaF and ocular fluorophotometer. 3 They detected following SCS delivery, a sharp concentration peak just posterior to the retina with significantly lower concentrations in the vitreous suggesting targeting of the SCS delivery. 3 Olsen et al. studied the pharmacokinetics of IVT injections versus microcannula suprachoroidal injections of Bevacizumab in a porcine model, at 12 h, they found similar RPE/choroid concentrations with both techniques, while the vitreous and anterior chamber measurements were dramatically lower in the suprachoroidal group that the IVT group. 14
The arterially perfused eye model was pioneered by Gouras and further refined by Niemeyer.38,39 In previous ocular perfusion studies, perfusion of one of the ciliary arteries has been shown to maintain the viability of the eye over a prolonged time period, with slow deterioration of the Bruch's membrane,24,40 maintenance of oxygen and glucose consumption indicating retinal tissue perfusion, 27 and functional blood–retinal barrier.39,41
This study has several limitations, including the use of an ex vivo model that could question the normal function of the RPE tight junction. A previous work studied the potential effect on drug penetration in postmortem eyes versus live eye by determining the integrity of ZO-1 protein expression. This work confirmed the normal function of the RPE tight junction for at least 3 h. 42 Another limitation is the very short period of time studied. Diffusion experiments have shown that the melanin-binding effect increases the lag time, since the steady state permeation begins only after the equilibrium between the free and melanin-bound drug has been achieved. 2 For this reason, the permeability of lipophilics drug through the RPE-choroid to the retina in our work (15 min) may be lower than true steady state permeability and it is difficult to determine whether the drug would penetrate further into the retina. It would be interesting in the future to extend the post-treatment time. Finally, during the arterial perfusion, the conjunctival tissue was trimmed, therefore limiting the final clearance by lymphatics and blood conjunctival vessels. However, in this study, we have also demonstrated the applicability of an arterially perfused ex vivo eye model to isolate the effect of choroidal circulation to better understand the effect of choroidal circulation on drug diffusion and as a clearance mechanism.
In summary, this study suggests that a hydrophilic drug injected into the SCS undergoes early clearance related to the presence of choroidal circulation, which may affect the desired drug concentration in the target tissue. Choroidal circulation affects the drug movement and distribution through the RPE-Choroid after IVT and SCS delivery.
Author Disclosure Statement
No competing financial interests exist.