
Abstract
Abstract
Purpose:
We aimed to compare the efficacy of topical daptomycin (DAP) with that of vancomycin (VA) in the treatment of keratitis caused by methicillin-resistant Staphylococcus aureus (MRSA).
Methods:
One hundred colony-forming unit MRSA bacteria were injected intrastromally into both corneas of 28 rabbits. Sixteen hours after injection, the rabbits' eyes were treated with 1 drop of topical DAP (10 or 50 mg/mL), VA (50 mg/mL), or isotonic saline for 19 doses. Their eyes were examined for clinical severity before and after treatment.
Results:
The minimum inhibitory concentration values of VA and DAP against the bacterial strain were found to be 2 and 0.5 μg/mL, respectively. The mean pre- and post-treatment clinical scores of the eyes did not differ significantly among the groups. However, the mean difference between the post- and pretreatment clinical scores was significantly lower in the 50 mg/mL DAP group than in the other groups (P=0.042). A marked decrease in bacterial load was detected in all treatment groups compared to the control group (P=0.002). Although there were no significant differences in bacterial load among the treatment groups, the 50 mg/mL DAP group showed the greatest decrease. The mean % epithelial erosion rate tended to be higher in the 50 mg/mL VA group than in the other groups (P=0.31).
Conclusions:
Topical DAP significantly reduced the bacterial load and showed activity against MRSA comparable to that of fortified VA in this experimental model.
Introduction
S
Due to the limited therapeutic options available, methicillin resistance is a significant problem in S. aureus isolates. Methicillin-resistant Staphylococcus aureus (MRSA) is increasingly being isolated in cases of bacterial keratitis, in which fortified vancomycin (VA), a glycopeptide antimicrobial, is the current standard of care. 3 However, VA is not stable in an aqueous solution. 2 Moreover, topical VA formulations prepared using saline were reported to irritate the eye due to their low pH, leading to noncompliance. 2 These negative aspects have meant that alternative, easy to use, effective, and less toxic antimicrobial agents for eye tissues are required.
Daptomycin (DAP), a cell membrane-targeting cyclic lipopeptide antimicrobial, is effective against Gram-positive bacteria, including MRSA. 5 It is produced by Streptomyces roseosporus and blocks synthesis of the bacterial membrane through transmembrane tube formation in lipoteichoic acid in the cell wall. 6 It also has postantibiotic activity within 6 h after treatment. 7 All S. aureus isolates are susceptible to DAP, and the MIC50 value of DAP against S. aureus was reported to be 0.094 mg/L. 8 The elimination half-life of DAP was found to be significantly longer compared with VA in a rabbit endophthalmitis model. 9 DAP could therefore be considered for the treatment of ocular infections caused by S. aureus, particularly MRSA.
To date, the antimicrobial potential of topical DAP has not been studied in corneal infection models. In this study, the in vivo activity and safety of 2 doses of topical DAP were investigated and compared to those of VA in an experimental MRSA keratitis model in rabbits.
Methods
Animals
A total of 28 specific pathogen-free New Zealand white male rabbits, weighing ∼2.0–2.5 kg, were used. Animals were treated in accordance with the Association for Research in Vision and Ophthalmology (ARVO) statement for Use of Animals in Ophthalmic and Vision Research. This study was approved by the animal research local ethics committee. A bilateral infection model was used in accordance with the ARVO guidelines to minimize the number of animals used. Bilateral infection in the central cornea does not produce a level of visual disability sufficient to disrupt the normal daily activity.3,10
Preparation of the MRSA strain
An ATCC MRSA 43300 standard strain was used for the keratitis model. A frozen stock of the isolate was inoculated onto blood agar and was incubated overnight at 37°C. After incubation, several colonies were inoculated into sterile saline to give a turbidity of 0.5 McFarland standards [1–2×108 colony-forming units (CFUs) per mL]. The suspension was serially diluted to a 10−4 level, equivalent to ∼100 CFU/10 μL, to be used to infect the corneas of the rabbits. The accuracy of the inoculums was confirmed by inoculating the serial 10-fold dilutions onto blood agar plates in duplicate.
Antimicrobial susceptibility of the strain
The minimum inhibitory concentrations (MICs) of VA and DAP against the MRSA strain used for the keratitis model were determined using the BD Phoenix Automated Identification System (Becton Dickinson) according to the recommendations of the manufacturer, and were evaluated according to the Clinical and Laboratory Standards Institute (CLSI) criteria. 11
Rabbit keratitis model
Each rabbit was systematically anesthetized through intramuscular injection of xylazine (10 mg/mL, Basilazin; Bavet) and ketamine hydrochloride (35 mg/kg, Ketalar; Pfizer). For topical anesthesia, 1–2 drops of 0.5% proparacaine hydrochloride (Alcaine; Alcon) were instilled into each eye. The eyes were held steady with a clamping forceps, and 10 μL of MRSA suspension containing ∼100 CFUs was injected directly into the corneal stroma using a 30-gauge needle on a 0.1-mL gas-tight syringe under a binocular microscope (Olympus SZ61) (Fig 1, top left and top right).
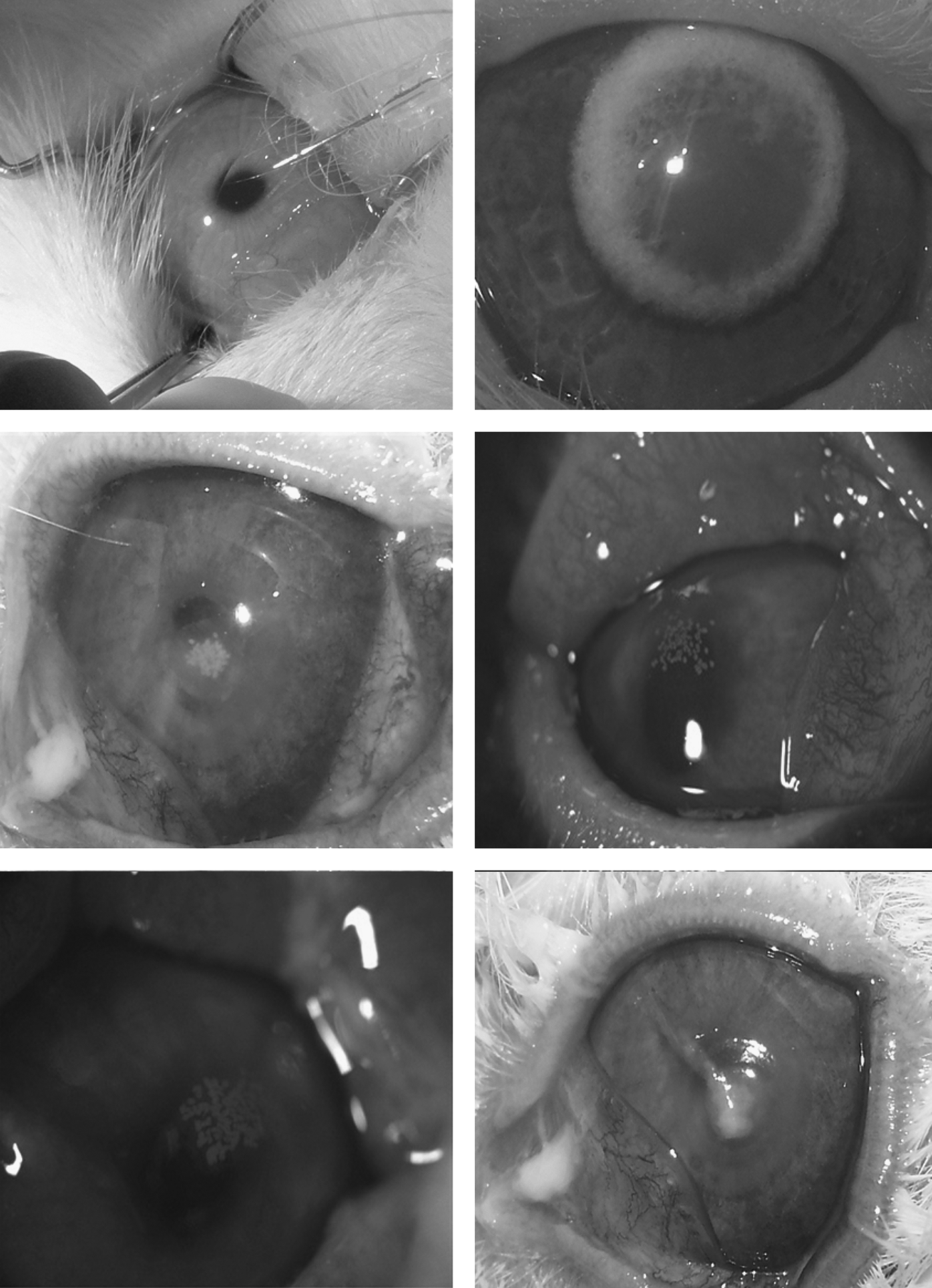
Intrastromal injection technique (top left) and corneal stromal hydration immediately after the procedure (top right). Representative images of infected eyes after treated with topical daptomycin (DAP) 10 mg/mL (middle left), DAP 50 mg/mL (middle right), vancomycin (VA) 50 mg/mL (bottom left), and isotonic saline (bottom right).
Examination and scoring of the eyes
Rabbits' eyes were examined by slit-lamp biomicroscopy by 2 blinded experienced observers at 16 h (pretreatment) and 25 h (post-treatment) after intrastromal injection. Eight parameters (iritis, corneal edema, chemosis, conjunctival injection, hypopyon, corneal infiltration, fibrin, and epithelial erosion) were assessed to determine the severity of infection. Each parameter was scored from 0 (normal) to 4 (maximal severity) for each eye of the rabbits by each observer. The 8 scores for each eye were added to give a total score with a theoretical maximum of 32. The final score for each eye represented the average of the scores of the observers.3,10
Treatment protocol
Treatment began immediately after the first examination and scoring, which were completed 16 h after injection. The rabbits were randomized into 4 treatment groups (7 rabbits per group) by an investigator who was not involved in the examination and scoring. The groups received 10 mg/mL DAP (obtained by dilution of a commercially available 50 mg/mL DAP preparation 1:5) (Cubicin®; Novartis), 50 mg/mL DAP, 50 mg/mL VA (vancomycin HCl, 500 mg; Abbott), or isotonic saline (control). One drop was applied to each eye every 15 min for the first 5 doses and then every 30 min for the remaining 14 doses (19 doses in total over 8.25 h).3,10
Euthanasia and tissue harvesting
After the treatment and the final slit-lamp examination, the rabbits were euthanized with an intravenous overdose of sodium pentobarbital (100 mg/kg; Sigma-Aldrich) at 25 h postinfection. Rabbit corneas were excised using a uniform sterile 7.5-mm Hessburg-Barron vacuum trephine (Altomed). Each of the right eyes was placed into a separate sterile container for bacteriological evaluation. The left eyes were fixed in 10% formaldehyde for histopathological examination.
Bacterial evaluation of the corneas
The right corneas of the rabbits were placed in sterile containers and weighed. The corneas were fragmented using a sterile lancet and 2 mL of sterile saline was then added. The containers were vortexed and 10-fold serial dilutions were prepared using sterile saline to give 10−1, 10−2, 10−3, 10−4, and 10−5 dilutions of corneal suspension to assay bacterial growth. Then, 10 μL of each suspension was inoculated onto 5% sheep blood agar plates in duplicate. All of the corneal suspensions were stored at room temperature. After overnight incubation of the blood agar plates at 37°C, the colonies were counted and calculated as CFU/g. One isolate from each group was identified as MRSA using the BD Phoenix Automated Microbiology System for confirmation. In addition, 1 mL of each of the corneal suspensions, which was negative in the culture, was inoculated into blood culture bottles and incubated in the BACTEC 9120 automated blood culture system (Becton Dickinson) for 7 days to confirm the negativity. MIC values of the strains isolated from each post-treatment group were determined to rule out any changes in susceptibility to VA and DAP during the treatment using the BD Phoenix automated system.
Histopathological examination
Excised corneas in 10% buffered formalin were embedded in paraffin blocks. Sections (4 μm thick) of all corneas were stained with hematoxylin and eosin (H&E) and were examined for stromal edema, corneal epithelial erosion, stromal polymorphonuclear leukocyte (PMNL) infiltration, and fibrin by a blinded pathologist using a light microscope. Epithelial erosion was determined as a percentage of the total length using an oculometer with the light microscope. The other parameters were scored from 0 (normal) to 3 (severe) for each cornea.3,10
Statistical analysis
Data analysis was performed using SPSS 17.0 for Windows (SPSS, Inc.). Whether the continuous variables were normally distributed was assessed using the Shapiro–Wilk test. The Levene test was used to evaluate the homogeneity of variances. Data are shown as mean±standard deviation or median [interquartile range (IQR)], where appropriate. Group means were compared by 1-way analysis of variance (ANOVA). The Kruskal–Wallis test was used to compare median values. When the P values for the 1-way ANOVA and Kruskal–Wallis test statistics indicated statistical significance, a post hoc Tukey's honestly significant difference test or the Conover's nonparametric multiple comparison test was used to determine which groups differed from which others. The Wilcoxon signed-rank test was used for intragroup comparisons. A P value<0.05 was considered to indicate statistical significance. Bonferroni adjustment was used for all multiple comparisons to prevent type I errors.
Results
MIC values
The MIC values of VA and DAP against the bacterial strain were found to be 2 and 0.5 μg/mL, respectively, indicating that the MRSA strain was susceptible to these antimicrobial agents according to the CLSI criteria. In addition, the MIC values of the strains of each post-treatment group were the same as the pretreatment ones.
Clinical scores
The mean pretreatment clinical scores of the right versus left eyes of the rabbits in the 10 mg/mL DAP, 50 mg/mL DAP, 50 mg/mL VA, and control groups were 7.64 versus 8.21, 8.00 versus 7.00, 8.14 versus 8.71, and 8.43 versus 7.86, respectively. The respective post-treatment scores were 10.93 versus 11.07, 9.36 versus 8.35, 12.07 versus 13.14, and 12.64 versus 14.00, respectively. The mean pre- and post-treatment clinical scores of the eyes did not differ significantly between the groups. However, the mean difference between the post- and pretreatment clinical scores was significantly lower in the 50 mg/mL DAP group than in the other groups (P=0.042). Table 1 shows the mean pre- and post-treatment clinical scores of the groups and significance levels. Figure 1 shows the representative keratitis pictures of the eyes in each group.
The comparison of clinical scores of the eyes before and after treatment among the groups, Wilcoxon signed-rank test, according to Bonferroni adjustment of P<0.00625 was considered to be statistically significant.
The comparison of clinical scores of the eyes after treatment compared to baseline among the groups according to laterality, 1-way ANOVA, according to Bonferroni adjustment of P<0.0125 was considered to be statistically significant.
DAP, daptomycin; VA, vancomycin; ANOVA, analysis of variance.
Microbiological evaluation
MRSA was isolated from the corneal cultures of all rabbits, except for one rabbit in the 10 mg/mL DAP group. A marked decrease in bacterial load was detected in all treatment groups compared to the control group (P=0.002). The mean (median [IQR]) bacterial loads (CFUs×106) in the 10 mg/mL DAP, 50 mg/mL DAP, 50 mg/mL VA, and control groups were 0.002 (0.04), 0.00004 (0.004), 0.32 (5.99), and 12.0 (22.4), respectively. There were no significant differences in bacterial load among the treatment groups. However, the 50 mg/mL DAP group showed the greatest decrease. Table 2 shows the bacterial loads and bacterial growth rates of the groups in detail.
There was a statistically significant difference between the DAP 10 mg/mL and DAP 50 mg/mL groups (P<0.001).
There was a statistically significant difference between the DAP 10 mg/mL and VA 50 mg/mL groups (P<0.01).
There was a statistically significant difference between the DAP 10 mg/mL and control groups (P=0.003).
There was a statistically significant difference between the DAP 50 mg/mL and control groups (P<0.05).
There was a statistically significant difference between the DAP 50 mg/mL and VA 50 mg/mL (P<0.001).
There was a statistically significant difference between the VA 50 mg/mL and control groups (P<0.001).
Kruskal–Wallis test.
One-way ANOVA.
PMNL, polymorphonuclear leukocytes; CFU, colony-forming units; IQR, interquartile range.
Histopathological evaluation
There were no significant differences among the groups in terms of histopathological parameters, including stromal edema, epithelial erosion, fibrin, and stromal PMNL infiltration. Table 2 shows the epithelial erosion, stromal edema, and stromal PMNL infiltration characteristics of the groups and significance levels. Figure 2 shows the histopathological features of corneal sections stained with H&E.
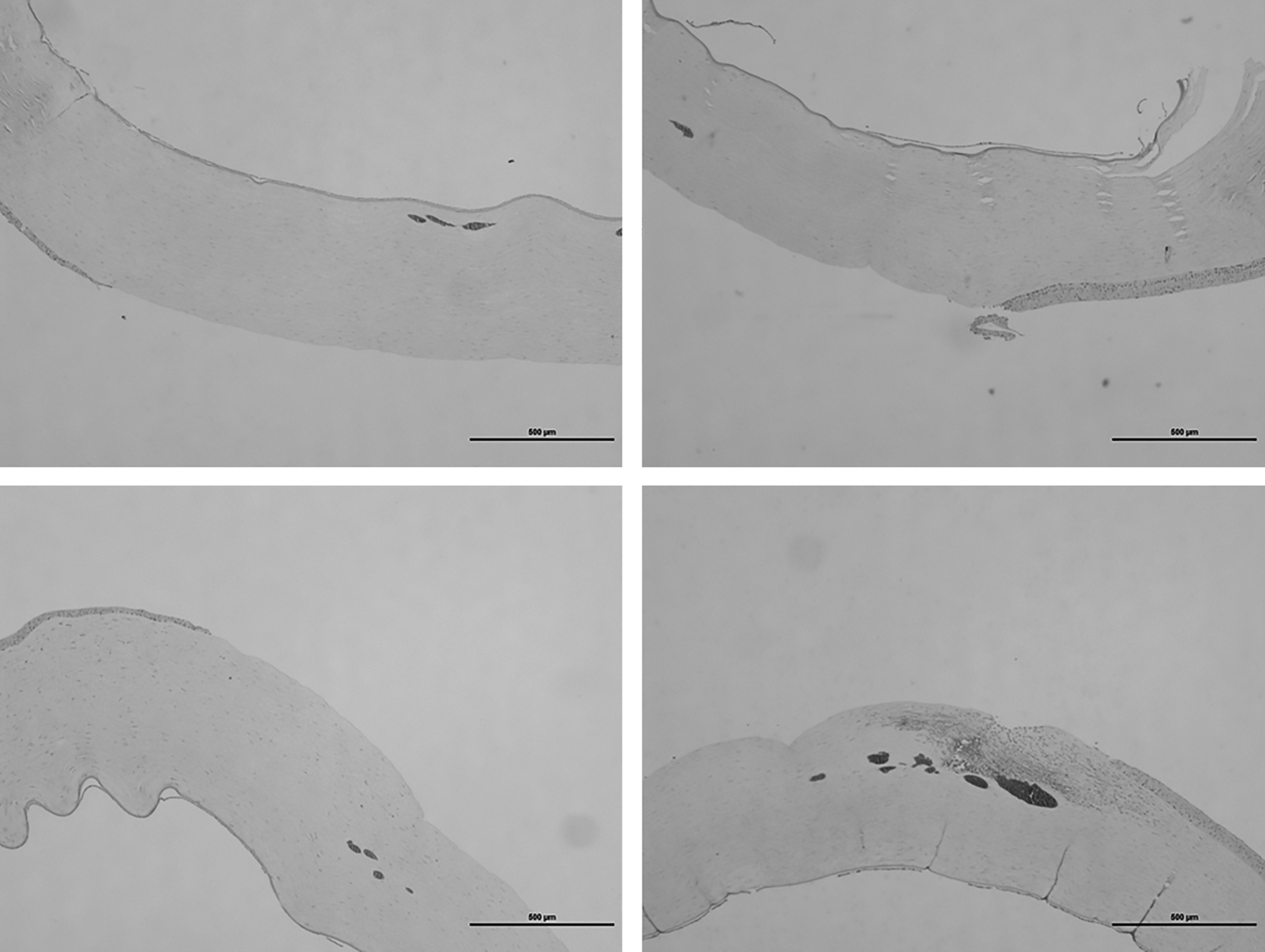
Histology of corneal sections stained with hematoxylin and eosin. A cornea treated with DAP 10 mg/mL (top left), DAP 50 mg/mL (top right), VA 50 mg/mL (bottom left), and isotonic saline (bottom right). Note that the increased infiltration of polymorphonuclear neutrophils into the corneal stroma in the control group compared to treatment groups.
Mean±(median [IQR])% epithelial erosion values were 33.50±12.31 in the 10 mg/mL DAP group, 35.19±30.94 in the 50 mg/mL DAP group, 53.86±25.02 in the 50 mg/mL VA group, and 32.30±23.29 in the control group. The mean % epithelial erosion rate tended to be higher in the 50 mg/mL VA group than in the other groups (P=0.31). The mean % epithelial erosion scores were similar in the other 3 groups.
Discussion
Bacterial keratitis is a sight-threatening infection of the cornea that needs to be treated promptly and effectively. Accurate management is based on proper identification of the causative microorganism and determination of the most appropriate antimicrobial option(s). Corneal infections caused by MRSA are usually difficult to treat due to a limited number of effective antimicrobials. In addition to this, serious side effects of currently available fortified antibiotic agents 12 may reduce patient compliance. This study presents the first evidence of therapeutic activity of DAP against MRSA in an in vivo keratitis model. We found that, DAP was found to be more effective than VA, the current golden standard therapeutic agent in MRSA keratitis, in reducing the bacterial load. Another finding of the present study was less epithelial toxicity of DAP compared to VA by means of histopathologically confirmed epithelial erosion. Therefore, DAP may be a safe and effective alternative option in the treatment of MRSA keratitis.
Fluoroquinolones have been used for treating susceptible strains of MRSA, however, S. aureus has also become increasingly resistant to fluoroquinolones through mutations in the genes for DNA gyrase and topoisomerase IV. 13 Several recent studies reported high rates of in vitro resistance of MRSA to fluoroquinolones.14,15 Besides, the CLSI states that staphylococci may develop resistance during prolonged therapy with quinolones, so isolates that are initially susceptible may become resistant within 3–4 days after the initiation of therapy. 11 Topical VA remains the mainstay of MRSA keratitis treatment because of the relative absence of antibiotic resistance. However, S. aureus with reduced susceptibility to VA has been identified. 16 Because some evidence shows that routine VA prophylaxis is effective in elective intraocular surgery, particularly in clear corneal phacoemulsification, 17 ophthalmologists are recommended to follow the advice of the Centers for Disease Control and Prevention 13 and the American Academy of Ophthalmology to avoid the routine use of VA for prophylaxis to prevent the spread of resistance. 13 Moreover, topical VA drops are not commercially available, necessitating their preparation in an inpatient pharmacy, require refrigeration to maintain stability, and are toxic to the corneal epithelium and may thus delay wound healing. In addition to these drawbacks, the recent emergence of rare mutant MRSA strains that are no longer susceptible to VA mean that there is a continuing need to identify new antimicrobial agents.
Recent studies have shown that DAP may be an effective agent against most clinically significant Gram-positive pathogens, including VA-resistant enterococci 18 and MRSA.19,20 Sakarya et al. 21 reported that DAP seems to penetrate well into the aqueous humor and cornea after topical administration in a multiple-drop regimen. The present study tested the efficacy of 2 concentrations of topical DAP in comparison to topical fortified VA and a saline control for the treatment of MRSA keratitis. None of the treatments reduced clinical scores of rabbit eyes at 25 h postinfection; however, both DAP concentrations significantly reduced the number of bacteria recovered from corneas compared to 50 mg/mL VA. In accordance with our results, Lefévre et al. 9 found that intravitreal DAP (1 mg/mL) was at least as effective at reducing bacterial numbers as VA in a rabbit model of endophthalmitis caused by MRSA. We used 10 and 50 mg/mL DAP because solubility limitations make topical treatment with DAP at doses higher than 50 mg/mL impractical. 21
Since there are no susceptibility standards for interpreting bacterial susceptibility in ocular infections, the MIC and disc susceptibility criteria for systemic administration are used to select the antimicrobial agent to treat bacterial keratitis.10,22,23 However, some reports provide evidence of a relationship between the MIC values of topically applied agents and clinical outcomes in cases of bacterial keratitis.24,25 Therefore, the MIC value of an agent is accepted to be an important measure for evaluating the efficacy of topically applied antimicrobials in the treatment of bacterial keratitis. In the present study, the MIC value of DAP was found to be lower compared with VA (0.5 vs. 2 μg/mL), suggesting that the strain was susceptible to both antimicrobials, and that a lower concentration of DAP was needed for treatment.
In cases of keratitis, epithelial erosion 26 and stromal edema 27 may be observed during the clinical course of the illness, independent of the causative microorganism. The levels of epithelial erosion and corneal edema are among the determining factors defining both the severity of infection and development of vision loss.26,27 In addition, topical fortified VA has a well-known therapeutic complication, corneal epithelial toxicity, which should be followed up carefully to decide whether to continue or stop the drug. In the present study, stromal edema scores were similar among the groups. In addition, the epithelial erosion rates in the 2 DAP groups and the control group (32%–35%) tended to be lower than that in the VA group (53%). These findings demonstrate both the epithelial toxicity of fortified VA and the therapeutic safety of DAP, despite its high dose, in accordance with previous studies of DAP.5,28
In conclusion, 50 mg/mL DAP reduced the bacterial load and controlled the disease severity more than VA in this experimental MRSA keratitis model. The epithelial toxicity of DAP seems to be less pronounced than VA by means of mean epithelial erosion values. Although this study was a preliminary investigation and further studies are necessary, DAP was shown to be a reasonable alternative to VA in the treatment of MRSA-related corneal infections.