
Abstract
Abstract
Purpose:
To evaluate the early functional and morphologic changes in patients with chronic central serous chorioretinopathy (CSC) after half-fluence photodynamic therapy (PDT) and to compare with fellow eyes.
Methods:
This prospective study included 32 symptomatic and 28 fellow eyes of 32 patients with chronic CSC. Indocyanine green angiography–guided half-fluence PDT (25 J/cm2) was performed. Best-corrected visual acuity (BCVA), central foveal thickness (CFT), and subfoveal choroidal thickness (SFCT) were evaluated at baseline and at days 1, 3, 7, 30, and 60 after PDT.
Results:
The mean age was 48.1±7.9 years. Baseline BCVA [logarithm of the minimum angle of resolution (logMAR)] improved from 0.56±0.23 to 0.54±0.24, 0.45±0.25, 0.38±0.23, 0.36±0.23, and 0.35±0.21 at days 1, 3, 7, 30, and 60. (P=0.91, P=0.004, P=0.002, P=0.001, and P<0.001, respectively). Baseline CFT decreased from 315±131 to 312±136, 305±136, 235±106, 174±44, and 165±36 μm at days 1, 3, 7, 30, and 60 (P=0.41, P=0.33, P=0.004, P<0.001, and P<0.001, respectively). Baseline SFCT in the symptomatic eyes was significantly greater compared with the fellow eyes (P=0.002) and changed from 517±98 to 546±109, 528±110, 495±119, 462±124, and 457±123 μm at days 1, 3, 7, 30, and 60 (P=0.02, P=0.42, P=0.07, P=0.004, P=0.003, respectively).
Conclusion:
The SFCT in the symptomatic eyes was greater in the fellow eyes at baseline. Functional and morphological chorioretinal changes started in very early period of treatment. Half-fluence PDT for chronic CSC resulted in thinner CFT and SFCT, and also showed a significant improvement in visual acuity.
Introduction
C
Given the importance of choroidal vascular hyperpermeability, long-term results of PDT investigating the effects of treatment on choroidal thickness in chronic CSC have been released by large number of studies.13–16 Some of these studies suggested that PDT reduces the choroidal vascular thickness, and maintained the remission for 1 year. 15 The outcomes of PDT for the changes in visual acuity and foveal and choroidal thicknesses were reported in long-term follow-up studies12–17 ; however, effects of PDT on retinal functions and morphology in early period after treatment are still unknown. Thus, this study aims to investigate the early changes of visual acuity, choroidal thickness, and central foveal thickness (CFT) in chronic CSC after half-fluence PDT and to compare with the fellow eyes.
Methods
Study design
This prospective, interventional, single-center study enrolled 32 eyes of 32 patients (8 women and 24 men) with chronic CSC between July 2012 and May 2013. The study design was approved by the Institutional Ethics Committee of the hospital. All procedures were conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all patients before the procedure.
Patients with persistent SRF of more than 6-month duration involving the fovea on spectral domain–optical coherence tomography (SD-OCT), active angiographic leakage in fluorescein angiography (FA), and abnormal dilated choroidal vasculature with hyperpermeability and/or punctate hyperfluorescent spots in indocyanine green angiography (ICGA) caused by chronic CSC were included in the study. Patients who had previous ocular surgery, CSC caused by high levels of corticosteroid, any kind of ocular pathology that could compromise visual acuity or cause a serous retinal detachment unrelated to CSC, or already received any forms of therapy, for example, PDT, laser photocoagulation, intravitreal injection of antivascular endothelial growth factor (VEGF) agents, were excluded from the study. Moreover, patients who had systemic hypertension, refractive errors ≥±3.0 diopters, history of ocular trauma, or glaucoma were also excluded to avoid any potentially confounding effect on the choroidal vascular system.
All patients had a complete ophthalmologic examination, including measurement of best-corrected visual acuity (BCVA) with Early Treatment Diabetic Retinopathy Study (ETDRS) chart in 4-m distance, determination of intraocular pressure, slit-lamp biomicroscopy, fundus examination, FA, ICGA, and SD-OCT at baseline. BCVA measurement and SD-OCT imaging were repeated at days 1, 3, 7, 30, and 60. BCVA was converted into logarithm of the minimum angle of resolution (logMAR) for the purpose of analysis.
The SD-OCT (Spectralis; Heidelberg Engineering, Inc., Heidelberg, Germany) using the eye-tracking system was performed to measure CFT and subfoveal choroidal thickness (SFCT) by enhanced depth imaging–optical coherence tomography (EDI-OCT) technique. CFT, which is the distance between the internal limiting membrane and the RPE at the central fovea, was automatically measured using the Heidelberg eye explorer software. SFCT is defined as the distance from the outer portion of the hyper-reflective line corresponding to the Bruch's membrane to the inner hyper-reflective line of the choroid-sclera interface at the central fovea. The measurements of SFCT were obtained with using measurement line contained in the Heidelberg eye explorer software and were performed by 2 examiners independently. If the difference between the 2 examiners was >15% of the mean of the 2 values, then there was open adjudication with the senior author. Data from a pilot study of normal eyes were previously reported, and these eyes were measured using the same techniques. 18 For EDI-OCT, an average of 100 automatic real-time frames were obtained to improve the quality of a single image. Subsequent EDI-OCT scans after PDT were performed with the follow-up mode to measure the same location.
FA and ICGA images were taken using a retinal angiograph (HRA; Heidelberg Engineering, Inc.), with a 30° field of view. In all patients, ICGA was used to confirm the diagnosis and guide the laser therapy. Choroidal abnormalities, including choroidal vascular hyperpermeability and punctate hyperfluorescent spots, were determined in middle-phase ICGA in both eyes of the patients.
For the PDT procedure, a 689-nm laser system (Carl Zeiss, Dublin, CA) with an indirect lens (Volk Area Centralis®) was used. All patients underwent a modified fluence PDT with reduced total light energy (25 J/cm2) and laser intensity (300 mW/cm2) using the standard dose of verteporfin (6 mg/m2) and standard time of laser emission (83 s). The PDT spot size was equal to the size of the lesion to cover entire lesion and determined by measuring the greatest linear dimension of the area of choroidal vascular abnormality in ICGA with a device-generated software tool. All PDT applications were performed by the same retina specialist (Zeynep Alkin).
Outcomes and statistical analysis
During a 60-day follow-up period, visual and tomographic outcomes were evaluated and compared between symptomatic eyes and the fellow eyes. For comparison of the tomographic outcomes between the symptomatic eyes and the fellow eyes, SD-OCT images that were obtained at the same time from either eye were used. Visual outcome was the change of mean BCVA in logMAR after the treatment, when compared with baseline. Tomographic outcomes included the change of SFCT and CFT. Time elapsed to the resorption of SRF and complications in the symptomatic eyes after half-fluence PDT was also recorded.
The obtained data were analyzed with frequency and descriptive statistics. The significance of changes in BCVA (logMAR), CFT, and SFCT was assessed using the Wilcoxon signed rank test. For all tests, P<0.05 was considered to be statistically significant. SPSS software version 16.0 for Windows (SPSS, Inc., Chicago, IL) was used for statistical analysis.
Results
Sixty-four eyes of 32 patients (8 women and 24 men) with a mean age of 48.1±7.9 years (range, 36–64 years) were included. Thirty-two symptomatic eyes with chronic CSC were treated with half-fluence PDT. However, 2 of the 32 patients with chronic CSC had a symptomatic disease in both eyes and 2 eyes had previous PDT, so these 4 fellow eyes were excluded from the study. Thus, 60 eyes of 32 patients were included, and for 28 patients, both eyes were analyzed. Of these 28 fellow eyes, choroidal vascular abnormalities were observed in 18 eyes (64%) in middle-phase ICGA. The area of choroidal vascular abnormality was located in the subfoveal area in all symptomatic eyes and in the subfoveal, parafoveal area or outside the fovea in the fellow eyes.
The mean duration of the current episode in the symptomatic eyes was 28.8±24 months (range, 7–72 months). SRF resolved in 30 eyes (93.7%) after half-fluence PDT; the remaining 2 eyes had persisting SRF during the follow-up period. The mean PDT laser spot size was 3.025±1.025 mm (range, 1.000–4.500 mm). Baseline clinical profiles of the patients are shown in Table 1.
SD, standard deviation; BCVA, best-corrected visual acuity; logMAR, logarithm of the minimum angle of resolution; CFT, central foveal thickness; SFCT, subfoveal choroidal thickness.
Mean BCVA (logMAR) in the symptomatic eyes and the fellow eyes was 0.56±0.23 and 0.19±0.33 at baseline, respectively. A significant difference in the baseline BCVA between the symptomatic eyes and the fellow eyes was detected (P=0.008). While BCVA (logMAR) remained significantly worse in the symptomatic eyes than that in the fellow eyes at days 1, 3, and 7, the difference decreased to nonsignificant levels at days 30 and 60 after half-fluence PDT (P=0.01, P=0.02, P=0.03, P=0.08, and P=0.11, respectively). Changes in BCVA in both of the symptomatic and fellow eyes were listed in Table 2. In the symptomatic eyes, BCVA showed a significant improvement at days 3, 7, 30, and 60, but not at day 1 (P=0.004, P=0.002, P=0.001, and P<0.001, P=0.91, respectively) compared with baseline after half-fluence PDT (Fig. 1).
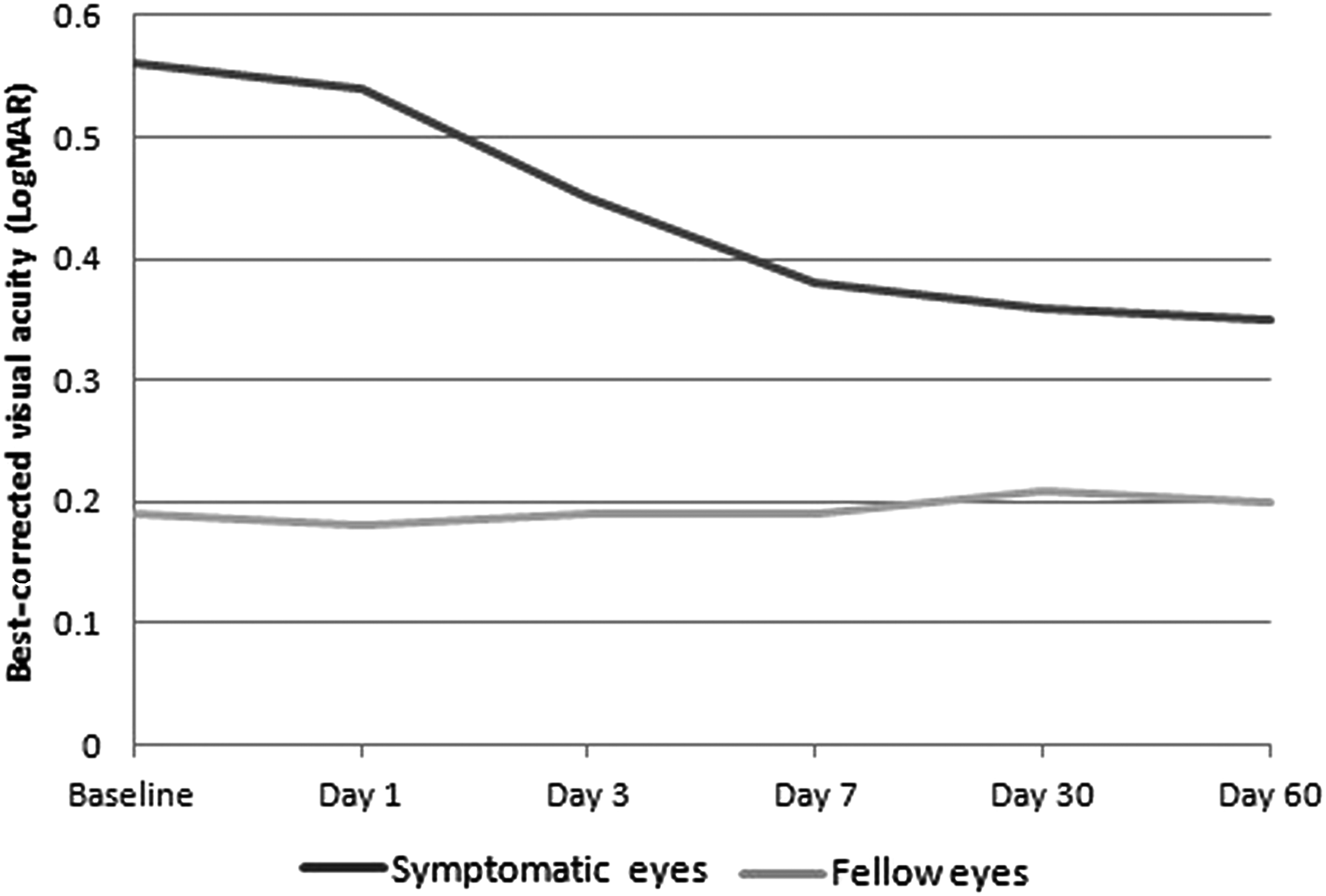
Course of best-corrected visual acuity (BCVA) in the symptomatic eyes showing an improvement starting from the first day of treatment. A significant increase in BCVA was first observed at day 3 and continued thereafter.
P-value based on Wilcoxon signed rank test of median difference equal to zero.
SD, standard deviation; BCVA, best-corrected visual acuity; LogMAR, Logarithm of the Minimum Angle of Resolution.
Mean CFT in the symptomatic eyes and the fellow eyes was 315±131 and 221±13 μm at baseline, respectively. Baseline CFT in the symptomatic eyes was significantly greater than that in the fellow eyes (P=0.03). CFT remained significantly greater in the symptomatic eyes than that in the fellow eyes at days 1 and 3; however, the difference was nonsignificant at day 7 after half-fluence PDT (P=0.01, P=0.02, and P=0.73, respectively). Then, CFT became significantly thinner in the symptomatic eyes than that in the fellow eyes at days 30 and 60 (P=0.01 and P=0.004, respectively). Changes in CFT in both of the symptomatic and fellow eyes were listed in Table 3. CFT showed a significant decrease at days 7, 30, and 60 after half-fluence PDT, but not at days 1 and 3 compared with baseline (P=0.004, P<0.001, P<0.001, P=0.41, and P=0.33, respectively) (Fig. 2).
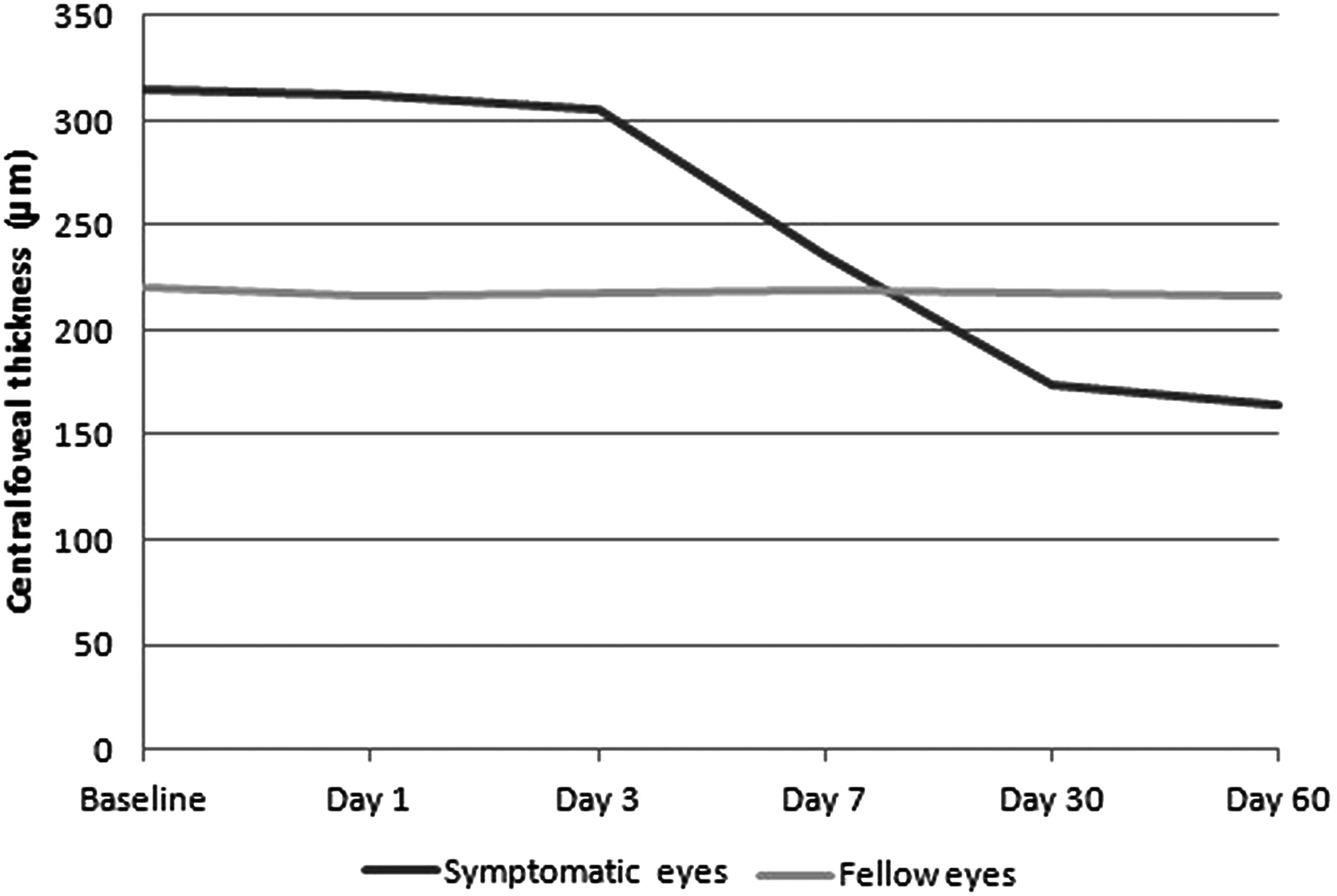
Graph shows changes in central foveal thickness (CFT) in the symptomatic eyes after half-fluence photodynamic therapy (PDT). A significant reduction in CFT in the symptomatic eyes was first observed at day 7. Fellow eyes showed a steady course during follow-up. CFT in the symptomatic eyes became thinner than that in the fellow eyes at days 30 and 60.
P-value based on Wilcoxon signed rank test of median difference equal to zero.
SD, standard deviation; CFT, central foveal thickness.
Mean SFCT in the symptomatic eyes and the fellow eyes was 517±98 and 426±115 μm at baseline, respectively. Baseline SFCT was significantly greater in the symptomatic eyes than that in the fellow eyes (P=0.002). Baseline SFCT in the fellow eyes with choroidal vascular abnormality (487±82 μm) differed significantly (P=0.004) from the SFCT (316±75 μm) in the fellow eyes without choroidal vascular abnormality, but did not differ from the symptomatic eyes (P=0.41). After half-fluence PDT, SFCT in the symptomatic eyes remained greater than that in the fellow eyes at days 1, 3, 7, 30, and 60 (P=0.001, P=0.002, P=0.01, P=0.03, and P=0.04, respectively). Changes in SFCT in both of the symptomatic and fellow eyes were listed in Table 4. After half-fluence PDT, SFCT in the symptomatic eyes showed a significant increase at day 1 (P=0.02). Then, SFCT showed a tendency to decrease for the remaining period of follow-up and a significant decrease in SFCT was observed at days 30 and 60 compared with baseline (P=0.42, P=0.07, P=0.004, P=0.003, respectively) (Fig. 3). The course of choroidal thickness changes and resorption of SRF is illustrated in Figure 4.

Changes in subfoveal choroidal thickness (SFCT) in the symptomatic eyes after half-fluence PDT. A slight increase in SFCT was observed at day 1 and then decreased until day 30, and stayed almost stable thereafter. SFCT in the symptomatic eyes was thicker than that in the fellow eyes through follow-up.
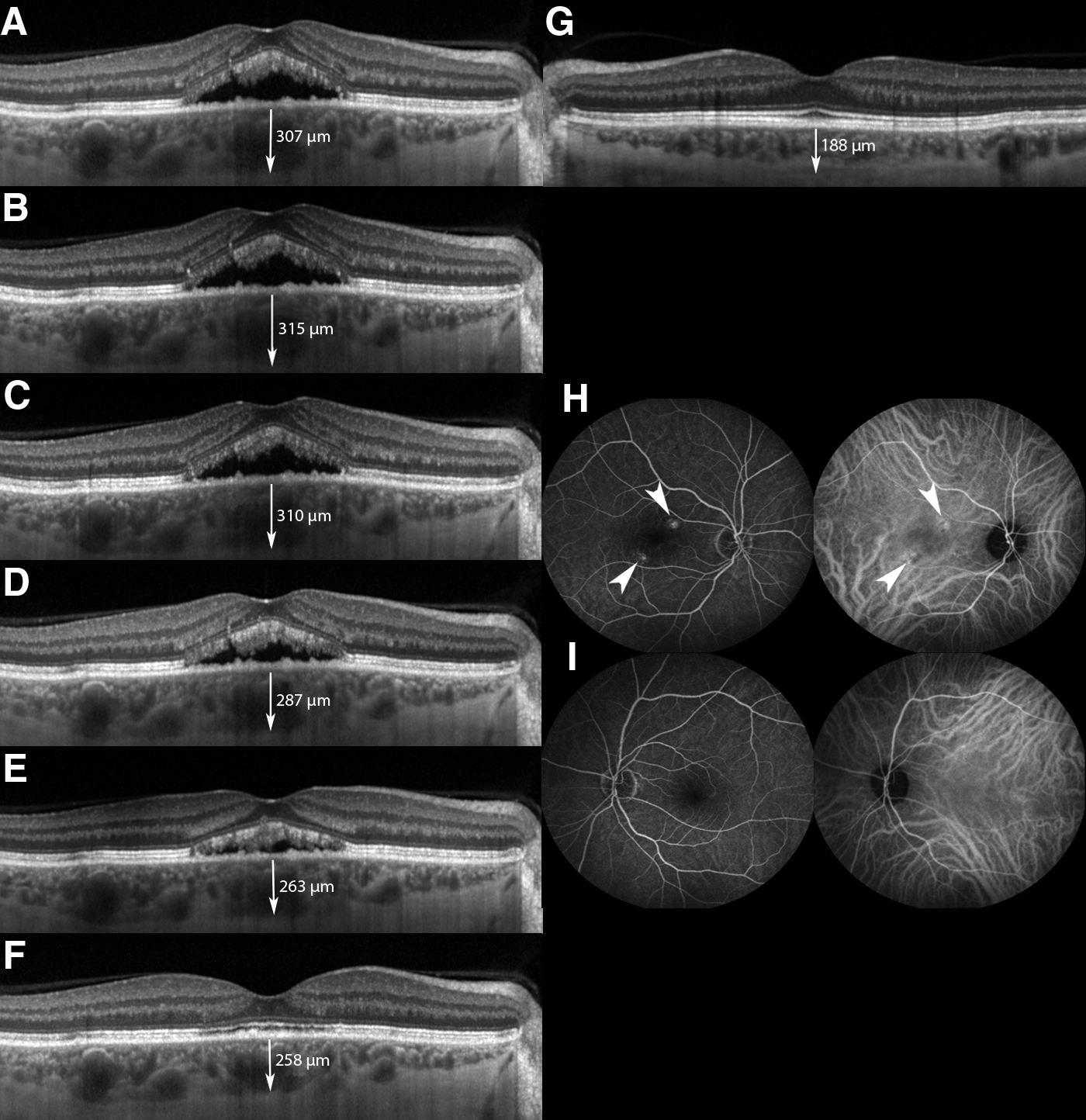
Representative enhanced depth imaging spectral domain–optical coherence tomography (SD-OCT) images of a patient who showed complete resorption of subretinal fluid (SRF) after half-fluence PDT. The arrows indicate the SFCT, the vertical distance from the outer portion of the hyper-reflective line corresponding to the Bruch's membrane to the inner hyper-reflective line of the choroid-sclera interface at the central fovea.
P-value based on Wilcoxon signed rank test of median difference equal to zero.
Discussion
In the present study, we investigated the early functional and morphologic changes after half-fluence (25 J/cm2) PDT in the symptomatic eyes with chronic CSC and compared with the fellow eyes. The results indicate that visual recovery starts as early as the first day of the treatment and progresses until the SRF resolves. Despite the complete resorption of SRF after half-fluence PDT, visual impairment that may result from degeneration or atrophy of the RPE and the retina caused lower visual acuity levels in the symptomatic eyes compared with the fellow eyes; however, difference was not significant at days 30 and 60. Additionally, the symptomatic eyes with chronic CSC were found to have thickened choroids compared with the fellow eyes. Once SRF resolves, choroid thickness seems stabilized up to 60 days. In particular, to the best of our knowledge, the current study is the first report to investigate very early functional and morphologic changes after half-fluence PDT and to compare these findings with the fellow eyes.
Although the pathophysiology of CSC remains elusive, the findings from previous studies provided strong evidence that CSC may be caused by increased hydrostatic pressure in the choroid. 19 The bilaterality of the choroidal vasculopathy in CSC was found in previous studies. 20 Kim et al. 20 reported that the rate of choroidal vascular hyperpermeability was 60% in the fellow eyes of patients with unilateral CSC. In the present study, the rate was 64% based on ICGA. Authors in the previous study concluded that the disturbances of choroidal circulation in patients with CSC give rise to increase in the hydrostatic pressure in the choroid, and subsequently, to increase in the thickness of choroid. 20 Maruko et al. 21 showed that the choroid thickened in both eyes, even if the SRF was present in one eye. They also showed that SFCT was greater in the fellow eyes with choroidal vascular abnormality than in the fellow eyes without choroidal vascular abnormality. In our study, SFCT was significantly greater in the symptomatic eyes than that in the fellow eyes, which is consistent with the results of Maruko et al. We observed that SFCT in the fellow eyes with choroidal vascular abnormality significantly differed from that in the fellow eyes without choroidal vascular abnormality. Moreover, we also found that SFCT in the symptomatic eyes was not significantly greater than that in the fellow eyes with choroidal vascular abnormality.
Despite the efficacy of PDT in chronic CSC, previous studies demonstrated complications, such as RPE-atrophy, choroidal ischemia, and secondary choroidal neovascularization, when applying standard fluence (50 J/cm2) PDT.9,10 Shin et al. 22 compared the efficacy and safety of half-fluence and conventional PDT. They found no significant difference in treatment success between the 2 groups (94.1% treated with half-fluence vs. 100% treated with conventional PDT); yet, the choriocapillaris perfusion decrease was significantly more severe in conventional PDT group. After half-fluence PDT, BCVA significantly improved at months 1, 3, and last follow-up (mean follow-up was 12.6 months) compared with baseline. In our study, we used an ICGA-guided PDT protocol with half-fluence (25 J/cm2) and normal dose of verteporfin (6 mg/m2) to enhance the efficacy and minimize the side effects of the treatment. Consistent with the findings of the aforementioned study, treatment resulted in 93.7% of eyes with complete resorption of SRF in the present study. Our results also showed that improvement of BCVA started at day 1, and then continued to significantly improve at days 3, 7, 30, and 60 compared with BCVA at baseline. PDT exerts a superoxide reaction on the choroidal vessels, resulting in vascular thrombosis. 23 A study by Maruko et al. 13 that compared the SFCT after photocoagulation or PDT in chronic CSC showed that choroidal thickness decreased after PDT but not after argon photocoagulation. Maruko et al. 13 also reported that baseline choroidal thickness significantly increased at day 2 after PDT and then decreased at day 7 and week 4 compared with baseline. The authors hypothesized that the choroidal thickness increases in early phase because of the upregulated production of VEGF and the reduction in late phase is because of the choroidal vascular thrombosis. Consistent with those findings, we found a transient choroidal thickening at day 1 after PDT. The baseline SFCT significantly increased at day 1 and then decreased at day 3 that was still greater than the baseline SFCT. SFCT reduced to below-baseline values at day 7 and showed a tendency to decrease at day 30 and at day 60. The results of the present study also revealed that SFCT in the symptomatic eyes remained greater than that in the fellow eyes throughout the follow-up.
In terms of change in CFT, a study by Smretschnig et al. 24 showed that CFT significantly decreased at 1 month and remained stable until 1 year after half-fluence PDT. In the present study, CFT showed a reduction starting from the first day of the treatment; yet, a significant reduction was observed at days 7, 30, and 60 compared with CFT at baseline. Moreover, we also found that CFT showed a tendency to be more decreased in the symptomatic eyes than that in the fellow eyes at days 30 and 60 after treatment. The smaller CFT in the course of SRF resorption may be because of 2 reasons; retinal atrophy because of extensive change by the disease itself, or retinal atrophy induced by PDT. However, our study was not designed to investigate the prognostic factors that affect the success of the treatment; thus, we did not evaluate neuroretinal thickness before and after the treatment.
Although this study has the strength of being a prospective, there are some weaknesses, including the small sample size and short-term follow-up considering the disease course of chronic CSC. Therefore, further study is needed in order to determine whether there would be any changes in outcomes in longer-term period after PDT. Additionally, there is currently no automated software to measure the choroidal thickness. Therefore, the choroidal thickness was measured manually in the present study. However, it has been shown previously that there is good interobserver repeatability with this technique by Spaide et al. 25
In conclusion, our results indicate that visual recovery started as early as the first day of the treatment and continued to improve until the complete resorption of SRF in the symptomatic eyes after PDT. We also found that SFCT in the symptomatic eyes was greater than that in the fellow eyes. Increased values of SFCT in the symptomatic eyes of chronic CSC reduced after half-fluence PDT. While it did not decrease to that of the fellow eyes throughout the follow-up. Another important finding in the present study was that resorption of SRF started as early as the first day of treatment despite choroidal thickness increased at that time. It remains unclear why the onset of resorption of SRF did not correlate with the normalization of SFCT in very early period of PDT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.