
Abstract
Abstract
Purpose:
To evaluate the inhibitory effects of propranolol, a nonselective and lipophilic β-adrenergic receptor blocker, on alkali-induced corneal neovascularization (NV).
Methods:
Corneal NV was induced in 24 eyes of 24 Wistar rats using NaOH. Following alkali burn, animals were randomized into 4 groups according to topical treatment. Group I received 0.9% NaCl, Group II received preservative-free dexamethasone sodium phosphate 1 mg/mL, Group III received propranolol hydrochloride 1 mg/mL, and Group IV received 0.5 mg/mL propranolol hydrochloride drops twice a day for 7 days. The inhibitory effects of the drugs were compared as the percent areas of cornea covered by NV. Anti-vascular endothelial growth factor (VEGF) and anti-active caspase-3 immunostainings were also performed in corneal sections.
Results:
The median percent area of corneal NV was 59% (40.3–65.6) in Group I, 25.5% (20.9–43.4) in Group II, 68.9% (36.7–78.0) in Group III, and 50.4% (42.2–63.3) in Group IV. Group III and IV did not show any difference in comparison to Group I. Group II showed a statistically significant smaller area of corneal NV compared with Group I, III, and IV (P=0.004 for each comparison). Anti-VEGF immunostaining was significantly less in Group II compared with the other groups. Anti-active caspase-3 immunostaining was not different among the treatment groups.
Conclusions:
Topical propranolol 1 or 0.5 mg/mL does not have a significant inhibitory effect on alkali-induced corneal NV in rats.
Introduction
N
β-adrenergic agonists cause angiogenesis in different ways: they promote proangiogenic factors [vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF)] and matrix metalloproteinases (MMPs) (especially MMP2 and 9) and activate the extracellular signal-related kinase (ERK)/mitogen-activated protein kinase (MAPK) cascade.6,7 Apoptosis is inhibited through the src/MAPK cascade in β-adrenergic receptor activation. 7 β-adrenergic agonists induce vasodilatation and an increase in vascular permeability using nitric oxide.6,7 Propranolol, a nonselective lipophilic β-blocker that prevents the action of adrenaline and noradrenaline on both β1- and β2-adrenergic receptors, has been used in the treatment of infantile hemangioma (IH), which is characterized by proliferation of vascular endothelium, which results in abnormal vessels. The mechanism of action of propranolol in IH is not clearly identified, but it is apparent that the vessels regressed after propranolol therapy, which made propranolol a good choice in clinically important IHs since 2008. 8 It is thought that the β-adrenergic receptor blockade results in vasoconstriction, inhibition of angiogenesis, and induction of apoptosis. 7 The inhibition of endothelial cell proliferation, migration, and differentiation by propranolol is not limited with IH endothelial cells; it also inhibits normal primary endothelial cells too. 9 Propranolol was shown to induce apoptosis through caspase-3 and inhibits VEGF expression in hemangioma-derived endothelial cells. 10 Recently, the effect of propranolol on diabetic retinopathy, retinopathy of prematurity, and choroidal NV has been studied.11–13
The brilliant success in the treatment of IH with propranolol showed us the idea of using propranolol in corneal NV. To the best of our knowledge, the inhibitory effect of propranolol on corneal NV has not yet been studied. In this study, we evaluated the inhibitory effects of 2 different concentrations of topical propranolol on alkali-induced corneal NV in a rat model.
Methods
Experimental procedures
All of the procedures involving animals were conducted in accordance with the Association for Research in Vision and Ophthalmology resolution on the use of animals in research. Our local ethics committee approved the study. Twenty-four male albino Wistar rats weighing between 200 and 250 g were used in this study. The rats were housed under conditions of controlled temperature (23°C±20°C), illumination (12-h light–12-h dark cycle), and food and water provided ad libitum.
General anesthesia was achieved after intraperitoneal injection of ketamine hydrochloride 25 mg/kg of body weight (Ketalar®; Pfizer, Istanbul, Turkey) and xylazine hydrochloride 5 mg/kg of body weight (Rompun®; Bayer AG, Leverkusen, Germany). Only the right eyes of each rat were used in the study. Corneal anesthesia was induced by administration of topical proparacaine hydrochloride 0.5% drops (Alcaine®, Puurs, Belgium). Whatman #3 filter paper discs produced by a standard 3 mm biopsy punch were soaked for 10 s in 2 M NaOH. Afterward, discs were drained and overloaded moisture absorbed on tissue paper as described previously. 14 They were then placed in the center of each right cornea for 60 s. The molarity of NAOH and duration of filter papers on the rat corneas were determined after 2 preliminary experiments. Subsequently, 10 mL of saline was used to irrigate the cornea and conjunctival sac. To maintain high reproducibility rates of the burns, a single investigator (ME) did all the procedures. The burn stimulus response was scored by a blinded examiner (HS) as 0 (no blister, not raised above the corneal surface), +1 (small blister, raised slightly above the surface), +2 (medium blister, raised moderately above the surface), and +3 (large blister).
Rats were then randomly divided into 4 equal groups according to topical treatment; Group I received saline (0.9% NaCl) drops, Group II received preservative-free dexamethasone sodium phosphate 1 mg/mL (Dexasine® SE; Alcon Pharmaceuticals, Kayserberg, France), Group III received propranolol hydrochloride 1 mg/mL (Dociton® Injectionslösung; Mibe, Brehna, Germany), and Group IV received 0.5 mg/mL propranolol hydrochloride drops twice a day starting immediately after burn stimulus until the seventh day. Propranolol 1 mg/mL was diluted with isotonic saline at a 1:1 ratio to a concentration of 0.5 mg/mL.
On the seventh day, rats were anesthetized using the same method described above and photographs of the right eyes were taken with a Topcon SL-D7 slit lamp model with attached DC-3 camera. The apex of the cornea was placed in the same direction with a 0° beam angle of slit-lamp illumination to take standardized photos and make the whole cornea visible in the photograph.
Tissue preparation and immunostaining
Rats were sacrificed and their right globes were enucleated. To establish a good fixation, eyes were punctured with a 27-gauge needle at 2 points 1 mm away from limbus before they were placed in 10% formaldehyde for fixation for 24 h. The tissues were dehydrated in graded ethanol and embedded in paraffin wax. The paraffin-embedded tissues were cut into 5-μm-thick slices, mounted on polylysine-coated slides, deparaffinized with xylene, and rehydrated through graded concentrations of ethanol. Analysis was made of the photographs taken by a Nikon Eclipse 80i microscope attached to a Nikon DS-Fi1.
Immunohistochemically, as primary antibodies, the anti-VEGF antibody (Abcam, Cambridge, United Kingdom) and anti-active caspase-3 (Thermo scientific, Fremont, CA) were used. For antigen retrieval, sections were immersed in a 10 mM sodium citrate buffer for 5 min (pH 6.0) and heated for 20 min in a microwave oven. Endogenous peroxidases were quenched in 0.3% (v/v) hydrogen peroxide for 5 min. After washing in phosphate-buffered saline, slides were incubated with a blocking reagent for 10 min. Sections were incubated for 30 min at 37°C with primary antibodies. The sections were further incubated with the anti-polyvalent biotinylated antibody (ScyTek Laboratories, Logan, UT). The immune complexes were detected using an AminoEthyl Carbazole chromogen (ScyTek Laboratories) according to the manufacturer's instructions. 15
Anti-VEGF immunostaining intensity was evaluated in the whole cornea semiquantitatively with a previously described technique 16 as no (0), weak (1), moderate (2), or intense (3). Apoptosis was evaluated in the epithelium of corneas with the anti-active caspase-3 antibody-stained slices. The immunostaining intensity of anti-active caspase-3 was determined in the same fashion as anti-VEGF immunostaining. All evaluations were performed by an experienced examiner (EHT) who was blinded to experimental groups.
Photographic analysis
Initially, the photographs taken were cut in an ellipsoidal pattern through limbus by using Photoscape v3.4 (2005–2009 Mooii Tech Co. Ltd, Korea). Afterward, the tip points of vessels extending through the corneal center were merged end-to-end to form an imaginary irregular circular pattern, which represents the border of the vascularized/unvascularized cornea with the free accessible GIMP 2.6.11 GNU Image Manipulation Program (Fig. 1). Then, the area between the limbus and this imaginary circle was automatically painted with black and the center of the cornea with white. The photographs were then converted to binary code and pixel analysis was performed. The percentage of vascularized areas shown with black and the total corneal area was processed semiautomatically using the MATLAB R2008b (MathWorks, Natic, MA) program. The percentage was used to prevent the effect of different-sized corneas.

The representative picture of photographic analysis. Whole cornea is seen, the broken black–white irregular circuloid line was generated by the connection of the tip points of the new vessels, which extend to the center of the cornea.
Statistical analysis
Statistical analysis was done with SPSS 17.0 statistical software (SPSS, Inc. Chicago, IL). A P value<0.05 was considered statistically significant. All data are presented as median (minimum–maximum). The Kruskal–Wallis test was used to compare continuous variables. The Bonferroni adjusted Mann–Whitney U test was used for multiple comparisons. The P value was calculated according to the 0.05/(number of comparisons), so a P value<0.05/6≈0.008 was considered as statistically significant. The chi-square (Fisher's exact) test was used for categorical variables and data are presented as frequency and percent (%).
Results
There was no difference among the groups in terms of burn stimulus intensity (P=0.75). The difference among the groups was statistically significant in terms of percent areas of corneal NV (P=0.003). Figure 2 shows the representative pictures of corneas covered with NV in each group. According to the percentage of areas vascularized, propranolol treatment groups (Group III and IV) were not statistically significant in comparison to the control group. The details about the percentage of area vascularized are shown in detail in Table 1.

The representative pictures of corneas covered with neovascularization in each group. Control group (top left), topical dexamethasone 1 mg/mL group (top right), topical propranolol 1 mg/mL group (bottom left), and topical propranolol 0.5 mg/mL group (bottom right).
Values are expressed as median (minimum–maximum). The superscripts a, b, and c point to statistically significant differences between Group II versus Groups I, III, and IV (P=0.004 for each). The superscripts d, e, and f point to statistically significant differences between Group II versus Groups I, III, and IV (P=0.007, 0.009, and 0.007, respectively).
Not statistically significant P=0.323.
VEGF, vascular endothelial growth factor.
The anti-active caspase-3 immunostaining intensity for the determination of apoptosis did not show a statistically significant difference between groups (Table 1). Figure 3 shows representative images of anti-active caspase-3 immunostaining in each group. The anti-VEGF immunostaining intensity was significantly different among the groups (P=0.002). Group II showed the least anti-VEGF immunostaining intensity compared with the other groups. There was no difference among Groups I, III, and IV in terms of anti-VEGF immunostaining intensity. Table 1 shows the details of anti-VEGF immunostaining in each group in detail. Figure 4 shows representative images of anti-VEGF immunostaining properties in each group.
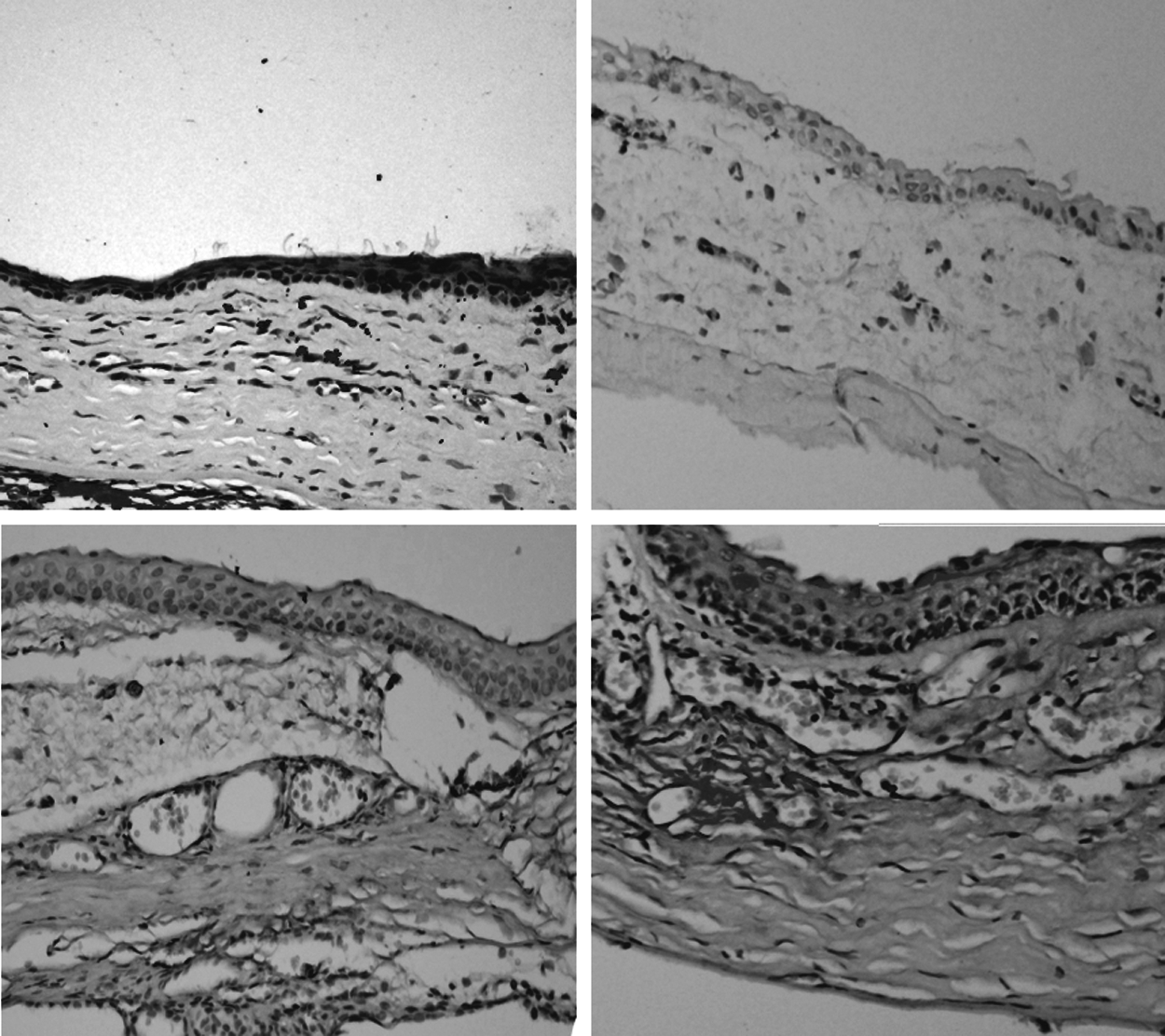
The representative sections of corneas stained for caspase-3 after being treated with isotonic saline (top left), topical dexamethasone 1 mg/mL group (top right), topical propranolol 1 mg/mL group (bottom left), and topical propranolol 0.5 mg/mL group (bottom right).

Anti-vascular endothelial growth factor immunostaining in isotonic saline group (top left), topical dexamethasone 1 mg/mL group (top right), topical propranolol 1 mg/mL group (bottom left), and topical propranolol 0.5 mg/mL group (bottom right). Higher densities of immunostaining were observed in the control, topical propranolol 1 and 0.5 mg/mL groups.
Discussion
In the present study, we demonstrated that topical administration of propranolol at 1 or 0.5 mg/mL doses does not seem to have a remarkable inhibitory effect on alkali-induced corneal NV in terms of the vascularized area, VEGF, and caspase-3.
VEGF has been documented as a major molecule not only in corneal NV 17 but also in diabetic retinopathy and choroidal NV. 18 VEGF was inhibited by dexamethasone in IH cells and cancer cells too.19,20 In our study, VEGF immunostaining of the cornea is significantly decreased by dexamethasone by means of percentage of areas neovascularized. This is in line with previous results of VEGF levels in alkali-induced corneal NV in a rat model. 21
Topical propranolol does not have an effect on VEGF immunostaining intensity of vascular endothelial cells in our study. Supporting this evidence, Chen et al. 22 showed that propranolol has no effect on NV in oxygen-induced retinopathy, and VEGF-A levels are not affected by propranolol administration in mice. Furthermore, using propranolol in normal and diabetic rats does not have an effect on retinal VEGF expression. 11 Additionally, Ristori et al. 12 stated that propranolol had no effect on VEGF levels in normoxic conditions both in the retina and other tissues. All these literatures are consistent with our results. On the contrary, Ristori et al., in the same study, established that propranolol had decreased VEGF expression in oxygen-induced retinopathy in retinal tissue. Propranolol had also decreased NV in the choroid and retina.12,13 A decrease in VEGF levels by using propranolol was also shown in hemangioma endothelial cells and squamous cancer cells.10,23 Interestingly, propranolol in normal rats caused an increase in VEGF levels in the retina. 24 These conflicting results in the literature about the relationship between propranolol and VEGF may be due to differences in administration routes, dosages, and the difference in physiopathological mechanisms of the different diseases. Nonetheless, NV is an intricate process that is not yet fully understood. Different pathways may cause the same clinical situation, which leads to conflicting results.
There have been many well-established methods for the investigation of corneal NV in animals, including physical and chemical methods, corneal microcapsule bag method, and immune-inducing method.25–27 The corneal NV induced by various etiological factors shows different features. The corneal inflammation induced by alkali-induced corneal burn was severe, which indicated that the infiltration of inflammatory cells can play a part in the development of corneal NV. In the present study, an alkali-induced corneal NV method was chosen for the determination of potential antiangiogenic effects of propranolol. In our experimental model, topical propranolol (0.5 or 1 mg/mL) did not show significant inhibitory effects on corneal NV. Different models of corneal NV using higher concentrations of propranolol through various administration routes (eg, subconjunctival or systemic) may provide better arguments for demonstrating antiangiogenic effects of propranolol.
Schwartz et al. 28 studied the effect of timolol, a nonselective beta-adrenergic antagonist, on corneal NV. Timolol was shown to have no inhibitory effect on NV. The method they used to induce NV is different from our study. The authors implanted micropellets containing the basic fibroblast growth factor in the cornea and tested the inhibitory effect of commercially available preparation of timolol (0.1%). Propranolol is a nonselective β1 and β2 receptor antagonist. Besides β1- and β2-adrenergic receptor blockage, there is some evidence that β3 receptors might play an important role in retinal NV through the nitric oxide pathway. 29 Although there is no study performed about the effect of β3 receptors on corneal NV, in theory, the β3 receptor might serve as an alternative way for NV in the course of β1- and β2-adrenergic receptor blockage.
Caspase-3 is one of the key mediators of apoptosis. 30 In our study, there was no difference in immunostaining with anti-active caspase-3 among the treatment groups, which agrees with Meijer-Jorna et al., 31 who found the capase-3 activity to be low to absent in 8 IH surgical specimens. Caspase-3, which is one of the key enzymes of apoptosis, was shown to play a role in the regression in the treatment of alkali-induced corneal NV in the animal model. 32 Additional to this data, corneal NV was shown to be regressed through caspase-3 activation. 33 In our study, propranolol did not have an effect on caspase-3. Apoptosis, which was induced by propranolol, might have a different pathway than caspase-3 in alkali-induced corneal NV.34,35
Systemic and subconjunctival administration of propranolol might reveal different results, but it was shown that topical use of propranolol is a safe and an effective method for treatment of IH. 36 In addition, topical administration of propranolol reached higher therapeutic concentrations compared with systemic administration in periocular capillary hemangiomas. 36 The efficacy of subconjunctival and systemic administration of propranolol against alkali-induced corneal NV, which is a limitation of the present work, should be tested in future studies.
In conclusion, topical administration of propranolol does not seem to have an inhibitory effect on corneal NV in this rat model. Further studies are necessary to confirm our results and to determine the effects of different dosages of propranolol on corneal NV.
Footnotes
Acknowledgments
The authors thank Fahrettin Küçükiba and Kemal Polat for their valuable contribution to photographic analysis.
Author Disclosure Statement
None of the authors has any competing financial interests in this study.