
Abstract
Abstract
Purpose:
To assess the safety of intracameral injection of moxifloxacin (MFLX) using the total replacement technique [bag and chamber (BC) flushing].
Methods:
The anterior chamber including the area behind the intraocular lens was irrigated and replaced using BC flushing. In Group A, 36 patients received balanced salt solution irrigation in the right eye and intracameral MFLX (150 μg/mL: 33-fold dilution of 0.5% eye drops) in the left eye. In Group B, 33 patients received intracameral MFLX in the right (500 μg/mL: 10-fold dilution) and left eyes (150 μg/mL: 33-fold dilution). Visual acuity, intraocular pressure, corneal endothelial cell density, corneal thickness, and foveal thickness were recorded before and up to 3 months after surgery.
Results:
In either group, there were no statistically significant differences between the right and left eyes with respect to visual acuity, intraocular pressure, corneal endothelial cell count, and foveal thickness before and at 3 months after surgery. There was no difference in corneal thickness before and at 3 months after surgery. In patients who received 500 μg/mL MFLX during surgery, central corneal thickness at 1 week after surgery was significantly reduced.
Conclusions:
In the present study, there was no adverse effect associated with intracameral injection of 150–500 μg/mL MFLX. Moreover, our results supported the safety of BC flushing. Thus, BC flushing, which can irrigate the inside of the capsular bag and attain stable antibiotic concentrations, appears to be a favorable technique for intracameral injection of MFLX.
Introduction
P
When performing intracameral injections, it is common to use a relatively small volume (0.05–0.2 mL) of a highly concentrated antibiotic solution that is either undiluted or diluted.1–8 However, small-volume injection is likely to result in an unstable intracameral antibiotic concentration. Moreover, it is difficult to ensure the delivery of small amounts of antibiotics into the area behind the intraocular lens (IOL) where bacteria can be easily trapped. 9 Experiments with pig eyes indicated that in some cases, drugs administered to the anterior chamber do not effectively reach the area behind the IOL. 10 Suzuki et al. reported that bacteria trapped behind the IOL disrupted the posterior capsule and caused endophthalmitis after uneventful cataract surgery. 11 We previously reported that bag and chamber (BC) flushing (Fig. 1) using intracameral MFLX irrigated the anterior chamber and the area behind the IOL. 10 The total replacement method for this administration (BC flushing) resulted in a stable concentration because there was little individual difference in the actual intracameral injection. Thus, we prefer to use BC flushing for the final surgical intracameral injection of MFLX, rather than simple injection. In our previous retrospective survey, we observed no adverse effect in 18,794 cases following intracameral injection of MFLX using the total replacement technique. 8

A cannula is inserted and the anterior chamber is flushed for several seconds
In the present study, we aimed to estimate the safety of intracameral injection of MFLX using the total replacement technique (BC flushing) in a prospective manner.
Methods
Our study comprised 138 eyes of 69 patients who underwent cataract surgery from January 2012 to September 2013 at Saiseikai Kurihashi Hospital. The exclusion criteria were history of trauma, previous ophthalmic surgery, uveitis, corneal opacity, macular degeneration, or cystoid macular edema due to retinal diseases such as diabetic retinopathy and vein occlusion.
We administered 0.5% levofloxacin eye drops 4 times daily for 3 days before surgery. In all patients, 10% povidone–iodine was applied to the periocular area, followed by irrigation with 5 mL of 1.25% iodine solution. Following topical anesthesia with 1% xylocaine, all surgeries were uneventfully performed by a single surgeon using a 2.4-mm scleral corneal incision. The phaco settings were same for all surgeries; the divide-and-conquer technique was applied during the phacoemulsification of the lens. IOLs (iSert Micro 251; HOYA, Tokyo or W-60, Santen, Osaka) were inserted using injectors and the ophthalmic viscosurgical device (OVD) was eliminated using the standard irrigation and aspiration (IA) technique. The IA tip was not intentionally inserted behind the IOL. Instead, the IOL was tapped to facilitate OVD elimination. Furthermore, the anterior chamber, including the area behind the IOL, was irrigated and replaced with diluted MFLX or balanced salt solution (BSS) using the BC flushing technique (Fig. 1). The MFLX solution was prepared using commercially available self-preserved Vigamox 0.5% ophthalmic solution (Alcon, Fort Worth, TX).
In Group A, 36 patients received BSS irrigation in the right eye and intracameral MFLX (150 μg/mL: 33-fold dilution) in the left eye. In Group B, 33 patients received intracameral MFLX in the right (500 μg/mL: 10-fold dilution) and left eyes (150 μg/mL: 33-fold dilution).
After surgery, all patients received the following medications for 28 days: topical MFLX and 0.1% betamethasone sodium phosphate 4 times daily and topical bromfenac ophthalmic solution 2 times daily.
Corrected and uncorrected visual acuity (logMAR), intraocular pressure, and corneal endothelial cell density were recorded in each group before and at 3 months after surgery. Central corneal thickness was recorded before and at 1 week and 3 months after surgery in each group. Corneal endothelial cell density and central corneal thickness were recorded using a specular microscope (Noncon Robo FAII, Konan, Hyogo). In addition, foveal thickness was recorded before and at 1 and 3 months after surgery using optical coherence tomography (Cirrus™ HD-OCT; Carl Zeiss Meditec, Jena, Germany) in each group.
This study was approved by the Saiseikai Kurihashi Hospital Review Board and conducted under the guidelines of the Declaration of Helsinki. Written informed consent was obtained from each patient. Right and left eye measurements were compared in the 2 groups using Student's t-test by SPSS for Windows statistical program. Age and sex were analyzed using Student's t-test and Fisher's exact test, respectively. A P-value of<0.05 was considered significant.
Results
The mean age of the patients included in this study was 71.9±7.5 years (range: 54–83; 17 men and 19 women) for Group A and 73.9±8.5 years (range: 52–91; 10 men and 23 women) for Group B. There were no statistically significant differences between the patients in the 2 study groups with respect to age (P=0.84) or sex (P=0.22). All patients involved were Japanese.
A comparison between the right and left eyes in the 2 study groups did not show statistically significant differences in the ocular parameters of visual acuity, intraocular pressure, or corneal endothelial cell count before and at 3 months after surgery (Tables 1 and 2).
Figures 2a and b show the results of OCT for Groups A and B, respectively. A comparison between the right and left eyes in the 2 study groups showed no statistically significant differences in foveal thickness (Fig. 2a, b).
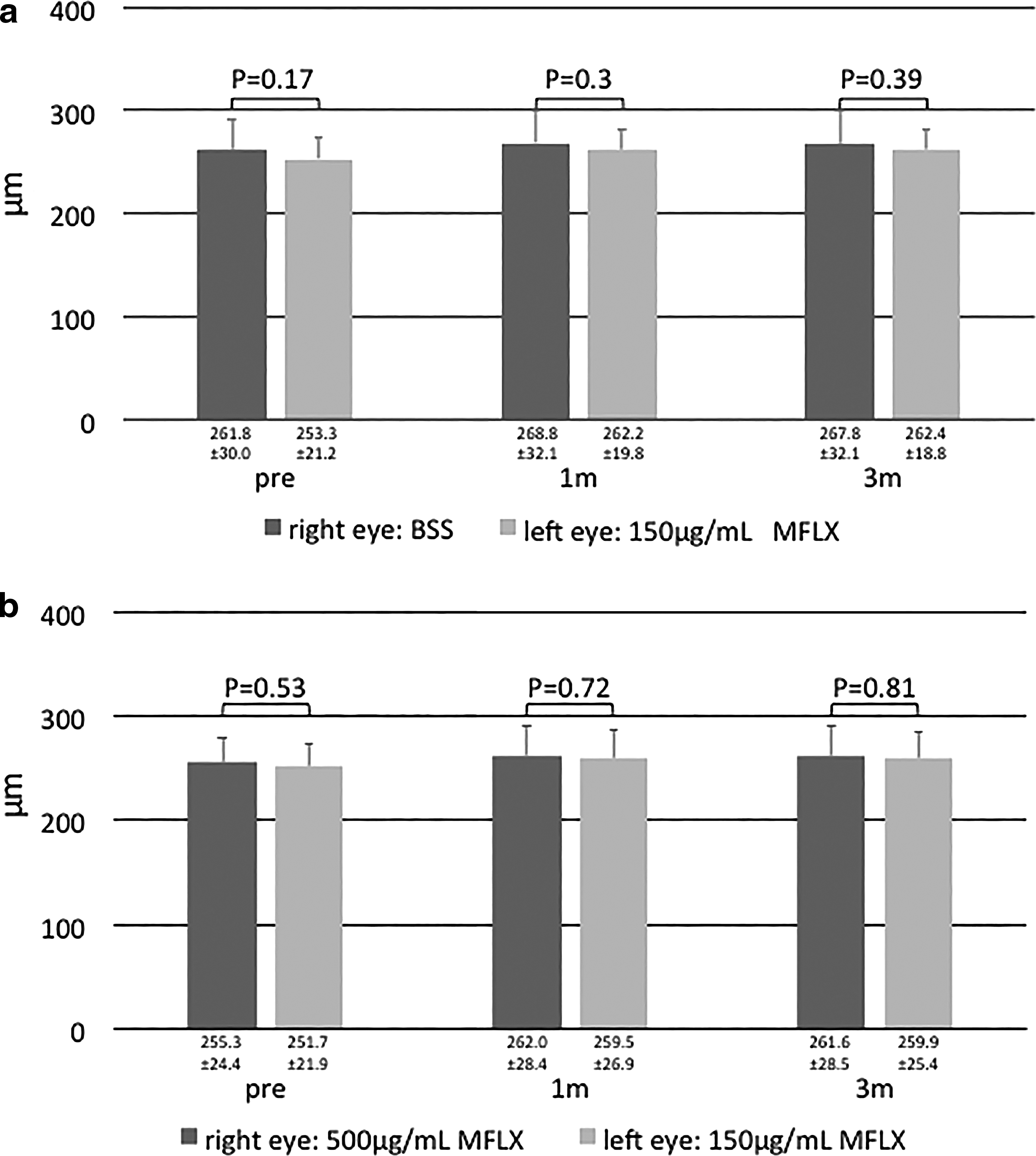
Comparison of foveal retinal thickness (mean±SD) in Group A
In patients who received 500 μg/mL MFLX during the procedure in Group B, central corneal thickness was significantly reduced at 1 week after surgery. Corneal thickness before and at 3 months after surgery demonstrated no differences in both groups (Fig. 3a, b).

Comparison of central corneal thickness (mean±SD) in Group A
No adverse events, such as severe corneal damage, toxic anterior segment syndrome, or posterior capsular rupture, were observed in any group. Endophthalmitis did not occur in any case.
Discussion
Arshinoff and Bastianelli observed that the infection rate following intracameral MFLX administration was only 1 in 35,194 cases. 12 Their data showed extremely low infection rates; however, this study included experienced surgeons as Arshinoff and Bastianelli menioned. Arbisser 7 used 0.1 mL of 1,000 μg/mL MFLX (5-fold dilution), Lane et al. 5 used 0.05 mL of MFLX stock solution, Espiritu et al. 3 used 0.1 mL of MFLX stock solution, and Ekinci Koktekir and Aslan 13 used 0.05 mL of 1,000 μg/mL MFLX (5-fold dilution). All these researchers demonstrated the safety of these concentrations in humans. After administering the doses recommended by these reports, anterior chamber concentrations were calculated to be ∼300–1,500 μg/mL.
To the best of our knowledge, there have been no reports regarding complications, such as toxic anterior segment syndrome or corneal endothelial cell damage, caused by intracameral MFLX administration. Meanwhile, Kernt et al. 14 observed impaired cultured corneal epithelial cells and retinal pigment epithelial cells at doses >250 μg/mL. Although Kernt et al. conducted an in vitro study under strict conditions that included incubation with the drug for 24 h, it is possible that high concentrations of MFLX are associated with latent dangers. Assuming that the half-life of intracameral MFLX is 1 h, 15 it is highly likely that any ensuing tissue damage may be within the permissible range even at higher concentrations in vivo. A final concentration of >1,000 μg/mL may not be necessary, although the safety of that concentration should be closely examined. In addition, an administration method other than small-volume injection has never been even examined. In other words, the most suitable administration method and optimal dose (concentration) has not been well established.
We previously conducted a retrospective survey at 19 institutions in west-central Japan where intracameral MFLX injections were administered. At all institutions, MFLX was diluted to a predefined concentration and administered using a 5-mL syringe to completely replace the fluid in the anterior chamber during the final stage of surgery. 8 The number of endophthalmitis cases at less than 1 month after surgery was 8/15,958 (ie, 1/1,955) before the introduction of intracameral MFLX administration, whereas there were 3/18,794 (ie, 1/6,265) cases after introduction. 8 The concentration range in the study was primarily 100–500 μg/mL.
In some cases, small-volume injection may result in unexpectedly lower or higher antibiotic concentrations. In addition, the distribution of MFLX in the eye is uneven. With small-volume injection, the antibiotic cannot be properly delivered to some areas. On the contrary, BC flushing will enable surgeons to deliver antibiotics to the anterior chamber and the area behind the IOL, to entirely replace the fluid in this area, resulting in effective irrigation and required antibiotic concentrations, and to create an instant self-sealing wound, avoiding hypotony and recontamination at the end of surgery. Consequently, BC flushing will perform well even with a “relatively low concentration.” The “relatively low concentration” ranged from 150 to 500 μg/mL in the present study. Considering that the concentration obtained after topical MFLX is 1.8 μg/mL, 16 the concentration of 150–500 μg/mL is ∼100 times higher. Unlike cefuroxime, whose effect is time-dependent, the effect of MFLX is concentration-dependent and a sufficient concentration maintained for ∼2 h is considered effective. 6 Metzler 17 revealed that the minimum inhibitory concentration required to inhibit 90% growth (MIC90) of methicillin-resistant Staphylococcus aureus was ∼16 μg/mL. Duggirala 18 indicated that the MIC90 for susceptible Pseudomonas aeruginosa was ∼2 μg/mL. Miller 19 reported on coagulase-negative staphylococci wherein the MIC90 reached 32 μg/mL. Using the 1-h half-life obtained from our study on rabbits, 15 the concentration of 150–500 μg/mL immediately after injection would be reduced to ∼38–125 μg/mL 2 h later, which was assumed to exceed the MIC90 of most pathogens.
Generally, corneal thickness increases as a result of postoperative inflammation or corneal endothelial cell damage. In the present study, no case of corneal edema was observed after surgery. Corneal thickness measured at 3 months after surgery showed no significant differences. In the group that received 500 μg/mL of MFLX, corneal thickness was significantly reduced at 1 week after surgery. This may be due to the anti-inflammatory effects of MFLX. Arbisser et al. reported that the aqueous cell count 1 day after surgery was significantly less in the MFLX-treated group compared with that in the control group. 7 Some reports have indicated that MFLX has anti-inflammatory effects and antibiotic effects.20,21 Fluoroquinolones have been shown to inhibit the secretion of other proinflammatory cytokines such as IL-1alpha, IL-3, IL-6, and IL-8 from macrophages. 22
In the present study, foveal thickness was not different between both groups.
A previous study examined the retinal safety of MFLX at intravitreal concentrations of 5–500 μg/mL using electroretinography (ERG) and histopathology in animal models. Intravitreal MFLX caused no ERG or retinal histologic abnormalities up to 100 μg/mL in mice and 150 μg/mL in rabbits. 23 Furthermore, intravitreal MFLX that exceeded the final estimated concentration of 300 μg/mL in rabbits was reported to be nontoxic as per the results of slit-lamp observation, indirect ophthalmoscopy, corneal ultrasound, and pachymetry. 24 Our previous experiments using pig eyes revealed that approximately >1% of intracameral MFLX (150 μg/mL) was transferred to the anterior vitreous (1.80–2.20 μg/mL) regardless of the administration method (small-volume injection or BC flushing) 25 ; toxicity to the retina did not appear to be a concern at these concentrations.
Endophthalmitis is a rare complication; hence, extremely large sample sizes are required to assess the effects and safety of any prophylaxis. Our previous survey with intracameral MFLX demonstrated a tendency toward a decrease in the number of cases of endophthalmitis but showed no significance compared with the control group. At the very least, we have never encountered any adverse effect following intracameral injection of MFLX.
Conclusion
In the present study, there were no adverse effects associated with intracameral injection of 150–500 μg/mL MFLX. Moreover, our results supported the safety of BC flushing. Our study indicates that BC flushing, which can irrigate the inside of the capsular bag and attain stable antibiotic concentrations, appears to be a favorable technique for intracameral injection of MFLX. However, as 150–500 μg/mL MFLX may not be sufficient enough to cover highly resistant strain, further studies are needed to confirm safety with higher doses, and efficacy in prevention of endophthalmitis.
Footnotes
Acknowledgments
The authors would like to thank Mr. Mitsuharu Ikeda for his assistance with this article.
Author Disclosure Statement
Dr. Yoshitsugu Inoue was a medical advisor at Alcon Japan from February to March 2013 and August to October 2013. No other authors received financial support from any public or private sources. The authors have no financial or proprietary interest in the products, methods, or materials described herein.