
Abstract
Abstract
Purpose:
To evaluate the efficacy and safety of gatifloxacin 0.5% ophthalmic solution administered twice daily for treatment of acute bacterial conjunctivitis.
Methods:
Two identically designed, double-masked, multicenter studies in the United States and India enrolled patients 1 year or older with acute bacterial conjunctivitis. Patients were randomized to gatifloxacin 0.5% or vehicle treatment for 5 days. Clinical success in clearing conjunctival hyperemia and discharge at day 6 (primary endpoint) and day 4 and microbiological cure were determined. Isolates from positive conjunctival samples were tested for sensitivity and susceptibility. Safety measures included adverse events (AEs). Data from these 2 studies were pooled for these analyses.
Results:
Of the 1437 randomized patients, 658 constituted the modified intent-to-treat population. Patient characteristics were similar between the pooled treatment groups. Clinical success occurred for 58.0% of gatifloxacin 0.5%-treated versus 45.5% vehicle-treated patients at day 6 (P=0.001) and for 23.7% versus 15.4% in the respective groups at day 4 (P=0.007). Microbiological cure was higher with gatifloxacin 0.5% than vehicle at days 4 and 6 (P<0.001 for both time points). The combined minimum inhibitory concentration required to inhibit 90% of isolates for gatifloxacin 0.5% was 2.0 μg/mL for gram-positive and gram-negative organisms. AEs were reported by 11.6% and 13.3% of patients in the gatifloxacin 0.5% and vehicle safety populations, respectively. One patient in each treatment group experienced a serious AE; neither was treatment related.
Conclusions:
The 0.5% concentration of gatifloxacin ophthalmic solution was safe and effective for treatment of acute bacterial conjunctivitis with twice-daily administration for 5 days.
Introduction
B
Although it is often a self-limiting disease, approximately 70% of patients with acute conjunctivitis seek treatment at primary and urgent care centers in the United States. 11 Empirical treatment with topical antibacterial agents that have a broad spectrum of activity against both gram-positive and gram-negative bacteria is the standard of care for acute bacterial conjunctivitis. 12 Meta-analyses have shown that topical antibiotic treatment can shorten the disease course, reduce likelihood of relapse, and decrease the risk of vision-threatening complications such as keratitis.12,13 Topical fluoroquinolones are active against bacteria that commonly cause conjunctivitis. However, older fluoroquinolones have been associated with ocular pathogen resistance.14–16
Antibacterial resistance is an inevitable consequence of the selective pressure of antibiotic exposure that is becoming prevalent among common bacterial causes of infections, including ocular infections. 17 Cavuoto et al. reported a 2-fold increase in the resistance of gram-positive organisms to ciprofloxacin from patients with bacterial conjunctivitis from 1994 to 2003. 18 More recently, Adebayo et al. reported a 6-fold increase in resistance to ciprofloxacin for both gram-positive and gram-negative isolates based on records of patients with bacterial conjunctivitis from 1997 to 2008. 4 An increasing frequency of methicillin-resistant Staphylococcus aureus (MRSA) among ocular isolates is of particular concern. Population-based surveillance studies indicate that MRSA infections are no longer confined to hospitals or hospital workers and can be acquired from the community.19,20 In the United States, the incidence of MRSA infections steadily increased from 29.5% in 2000 to 41.6% in 2005. 21 Among patients with bacterial conjunctivitis, the frequency of MRSA isolates significantly increased from 0.05% in 1994 to 30.5% in 2003. 18 Most MRSA are multidrug resistant (≥3 antibiotic agents), 21 and antibacterial-resistant infections may be more difficult to treat resulting in more serious complications. With continued increase in bacterial resistance, there is a need for effective antibacterial agents, such as a newer generation or formulations of fluoroquinolones, to treat ocular bacterial infections potentially caused by more resistant organisms.
Gatifloxacin ophthalmic solution 0.3% (Zymar®; Allergan, Inc., Irvine, CA), a fourth-generation fluoroquinolone, has been used successfully as a 4-times-a-day treatment of bacterial conjunctivitis. 22 Fluoroquinolones are concentration-dependent antibacterial agents 23 ; therefore, increasing the concentration of gatifloxacin may improve efficacy. In addition, enhancing the antibacterial activity of gatifloxacin 0.3% also may help prevent selection of resistant mutants. The gatifloxacin ophthalmic solution 0.5% (Zymaxid®; Allergan, Inc.) is a new formulation of gatifloxacin that was developed to maintain the safety of the prior formulation, while enhancing efficacy and allowing flexibility for a less frequent dosing regimen. Two large multicenter clinical trials that evaluate the efficacy and safety of gatifloxacin 0.5% ophthalmic solution in patients 1 year of age or older with acute bacterial conjunctivitis were designed and conducted to support regulatory approval. In this study, we report the pooled results of those trials.
Methods
Study design
Two identically designed, randomized, multicenter, double-masked, vehicle-controlled, phase 3 trials were conducted to evaluate the efficacy and safety of gatifloxacin ophthalmic solution 0.5% for the treatment of acute bacterial conjunctivitis. The first trial was conducted between August 2007 and June 2008 at 51 sites in the United States (ClinicalTrials.gov identifier: NCT00509873), and the second was conducted between February 2008 and January 2009 at 10 sites in the United States and 29 sites in India (ClinicalTrials.gov identifier: NCT00518089). Each study adhered to the tenets of the Declaration of Helsinki and Good Clinical Practice guidelines and was compliant with the Health Insurance Portability and Accountability Act of 1996 for all the US sites. The study protocol was approved by an institutional review board or independent ethics committee at each site and all patients provided written informed consent.
Study population
Patients at least 1 year of age were eligible for participation if they were clinically diagnosed in one or both eyes with acute bacterial conjunctivitis (or blepharoconjunctivitis), defined as moderate to severe (grade 2–3) conjunctival hyperemia and mild to severe (grade 1–3) discharge, graded on a 4-point scale (0=none, 1=mild, 2=moderate, 3=severe). Eligible patients must have had a best-corrected visual acuity equivalent to Snellen acuity of 20/80 or better. For children younger than 3 years old, visual acuity measurement was at the discretion of the investigator.
Patients were excluded if they had used antibiotics or corticosteroids for treatment of other infections during the past 1 or 2 weeks, respectively, before study enrollment; had signs and/or symptoms of conjunctivitis for more than 96 h or suggestive of fungal, viral, chlamydial, or allergic etiology; or were positive for adenovirus antigen using the RPS Adeno Detector™ [Rapid Pathogen Screening, Inc. (Williamsport, PA); K052092, November 2005] at baseline. Patients also were excluded from the trials if they had a clinical diagnosis of orbital cellulitis, preseptal cellulitis or ulcerative keratitis, infectious blepharitis as the primary cause of ocular hyperemia and discharge in the opinion of the investigator, uncontrolled systemic disease, serious systemic infection, immunosuppression, or known contraindications to any study medication component.
Patients may have had one eye or both eyes clinically diagnosed with acute bacterial conjunctivitis at day 1 (baseline) and qualified to be treated. If both eyes were diagnosed with acute bacterial conjunctivitis, the eye with positive bacterial conjunctival culture at baseline was designated as the study eye, while if both eyes were culture positive or negative at baseline, the right eye was designated as the study eye.
Study randomization, intervention, and masking
On the day 1 visit, after completion of the baseline eye examination, patients were assigned a randomization number sequentially, according to the order of enrollment within each site. Blocks of computer-generated numbers allocated to each site and a central, automated interactive voice response system/interactive web response system (IVRS/IWRS) were used for patient assignment. Patients were randomized 1:1 to receive either gatifloxacin 0.5% or vehicle (the formulation without gatifloxacin) in the qualified eye(s) for 5 days. On day 1, patients instilled 1 drop of study medication every 2 h for up to 8 doses. On days 2 to 5, patients instilled 1 drop of study medication twice a day in the qualified eye(s).
All study medication was supplied in identical sterile plastic 10-mL dropper bottles. The bottles had unit labels coded at Allergan using a computer-generated randomization list, which included the study number and kit number matching the patient randomization assignments. Patients, all personnel responsible for clinical management, laboratory staff, and study administrators were masked to the randomized treatment assignment throughout the study.
Visits were scheduled on day 1 (baseline), day 4, and day 6; the day 6 visit must have occurred between 12 h (minimum) and 48 h (maximum) after the last dose of study medication. At each visit, ocular signs (conjunctival hyperemia and mucopurulent discharge) and symptoms (itching and tearing) of conjunctivitis in both eyes were rated using a 4-point scale (0=none, 1=mild, 2=moderate, 3=severe). Using conjunctival swabs, samples for determining bacterial culture and sensitivity were taken from the clinically diagnosed eyes without the aid of topical anesthetic. The swabs were aseptically added to transport tubes and prepared for shipment to a central laboratory. Adverse events (AEs) were recorded, and visual acuity and biomicroscopy assessments were conducted in both eyes. At each study visit, the clinical staff inspected the medication bottle to confirm usage. Any major deviations from the administration schedule (eg, medication was administered for less than 5 days) were reported.
Microbiological sensitivity and susceptibility
Conjunctival samples with organisms above the in vitro pathological threshold were tested for microbiological sensitivity and susceptibility to gatifloxacin, moxifloxacin, azithromycin, ciprofloxacin, erythromycin, gentamicin, tetracycline, and tobramycin. In addition, the Kirby-Bauer measurement was used to test susceptibility to gatifloxacin and moxifloxacin. Sampling kits, including transport media, were provided to each site in the United States and India by Covance Central Laboratories Services (Indianapolis, IN), a laboratory certified by the College of American Pathology (CAP) and with Clinical Laboratory Improvement Amendments (CLIA) certification, to maintain uniform analytical processes. Instructions for collection, storage, and transport were provided to each site.
Conjunctival samples obtained at sites in the United States were sent directly to Covance for all analysis, including identification, quantification, and Kirby-Bauer testing. Conjunctival samples obtained from sites in India were frozen and shipped within 24 to 48 h, to Super Religare Laboratories Limited (formerly SRL Ranbaxy Limited, Mumbai, India), also CAP certified, which had received instructions on processing organisms from Covance. SRL performed identification, quantification, and Kirby-Bauer testing. Culture-positive organisms, determined to be above the specific quantitative threshold, were refrozen and sent in batches to Covance in the United States for susceptibility and minimum inhibitory concentration (MIC) testing. The organism identification completed in India by SRL was used for the outcome analysis, although the organisms were reidentified by Covance before susceptibility testing.
MICs (μg/mL) were determined for organisms above the pathological threshold at a given visit, and when multiple numbers of any one species were observed, MIC90s (minimum concentration required to inhibit 90% of isolates) were calculated. Sensitivity and susceptibility criteria were determined using the active agent by standard methods, defined by Clinical Laboratory Standards Institute (CLSI) Performance Standards for Antimicrobial Susceptibility Testing M100-S17 (2007) and CLSI M45-A (methods for antimicrobial dilution and disk susceptibility testing of infrequently isolated or fastidious bacteria). MIC results from a single laboratory, Covance, were used in data analysis for all sites.
Outcome measures and data analysis
All patients satisfying the inclusion criteria and clinically diagnosed with bacterial conjunctivitis at baseline, who were randomized and began treatment, comprised the intent-to-treat (ITT) population. Efficacy endpoints that were evaluated in the pooled modified intent-to-treat (mITT) population, comprised patients whose conjunctival samples collected from at least one of the qualified eye(s) at baseline tested positive for bacterial cultures postrandomization. All patients enrolled in the study who received at least 1 dose of study medication were included in the safety analysis; all qualified eyes were evaluated for safety assessments.
The prespecified primary efficacy endpoint for the pooled analyses was clinical success at day 6 in the pooled mITT population, defined as the proportion of patients with clearing of both conjunctival hyperemia and discharge (score of 0 for both) in the study eye using the up to day 6 analysis method. Since the self-limiting course of bacterial conjunctivitis may reduce observable differences between treatment groups at later time points, data collected after day 6 were excluded to identify treatment benefits that occurred before the resolution of bacterial conjunctivitis. All secondary efficacy endpoints were analyzed in the study eye and included clinical success at day 4, the patients achieving microbiological cure (defined as eradication of all bacteria present at baseline) at day 4 and at any time up to and including day 6, and clinical improvements in ocular signs and symptoms. AEs recorded by the investigator were coded to preferred terms using the Medical Dictionary of Regulatory Activities, version 10.0.
The last observation carried forward method was used to impute missing values for efficacy analyses of the mITT and ITT populations. Categorical variables were analyzed by the Pearson chi-square test, Fisher's exact test, or Cochran–Mantel–Haenszel method. Continuous variables were analyzed using analysis of variance for between-group comparisons and the paired t test for within-group analysis of changes from baseline. A P value of≤0.05 was considered a statistically significant difference between treatment groups.
Power calculations for each of the individual studies in this pooled analysis were based on a 2-sided Pearson chi-square test for the primary efficacy measure using the mITT population. Assuming clinical success in 57% of patients in the vehicle group and a type-I error rate of 0.05, a sample size of 140 patients per treatment group in the mITT population was estimated to achieve 80% power to detect a difference of 16 percentage points in clinical success, between gatifloxacin 0.5% and vehicle. With an expected 60% culture-positive rate, 467 patients were projected to be randomized in each study to attain 280 patients (140 per treatment group assuming an equal distribution of positive cultures in each treatment group) for the mITT population.
Results
Patient disposition and baseline characteristics
In total, 1437 patients were randomized in the two phase 3 studies; 1433 patients received at least 1 dose of study drug and constituted the safety population (Fig. 1). Seventy-two patients from 1 site were excluded from all efficacy analyses due to data integrity issues. The United States Food and Drug Administration was informed of the data integrity concerns and allowed the exclusion of these patients from the primary analysis. Consequently, the pooled ITT population consisted of 1365 patients; 681 randomized to receive gatifloxacin 0.5% (642 [94.3%] completed treatment) and 684 randomized to vehicle (639 [93.4%] completed treatment). The mITT population, the primary population for efficacy analyses, comprised 333 patients in the gatifloxacin 0.5% group and 325 patients in the vehicle group. Overall, patient disposition was similar between the 2 treatment groups and the majority of patients completed the study as planned.
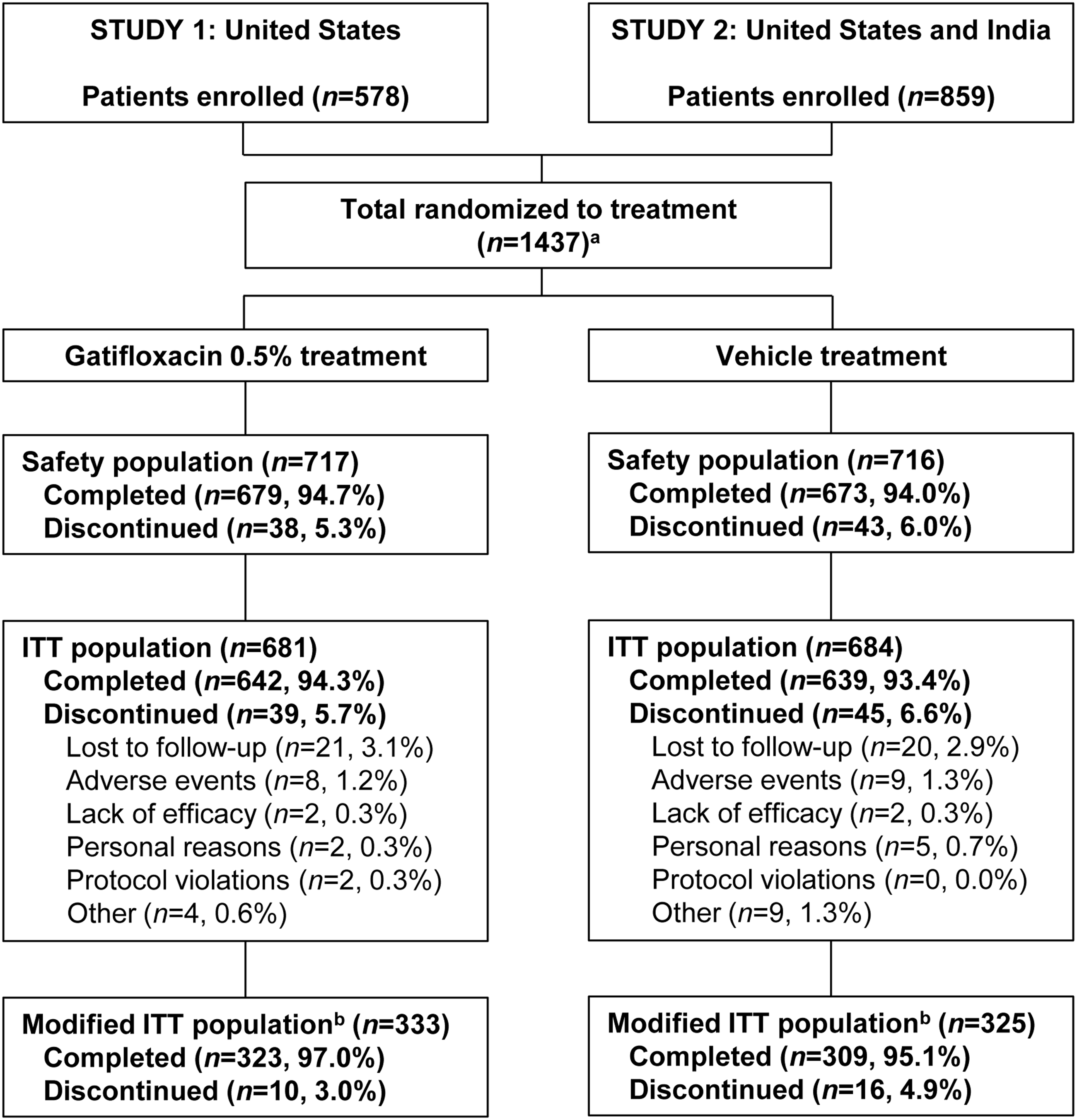
Patient disposition. aSeventy-two randomized patients from 1 site were excluded from the intent-to-treat (ITT) population and efficacy analyses due to data integrity issues. bModified ITT population consisted of patients with a positive conjunctival culture at baseline.
Baseline demographic and patient characteristics for the mITT population are presented in Table 1. There were no significant differences between treatment groups in age, sex, or race. Only a small difference in the severity of conjunctival hyperemia at baseline was present between the gatifloxacin 0.5% (2.3) and the vehicle group (2.2), although the difference was statistically significant (P=0.021). The severity of mucopurulent discharge and ocular symptoms of discomfort was comparable between the treatment groups at baseline.
P=0.021, one-way analysis of variance.
mITT, modified intent-to-treat; SD, standard deviation.
Clinical outcome results
Clinical success at day 6 (primary endpoint) occurred in 58.0% (193/333) of patients treated with gatifloxacin 0.5% compared with 45.5% (148/325) of the vehicle-treated group (P=0.001). At the day 4 time point, 23.7% (79/333) of patients receiving gatifloxacin 0.5% had clinical success compared with 15.4% (50/325) in the vehicle group (P=0.007) (Fig. 2A). At days 4 and 6, microbiological cure was greater in the gatifloxacin 0.5% treatment group, with the difference between treatment groups being statistically significant. At day 4, microbiological cure occurred in 87.4% (291/333) of patients in the gatifloxacin 0.5% group and 62.8% (204/325) in the vehicle group, and 90.4% (301/333) and 70.2% (228/325) had microbiological cure at day 6, respectively (P<0.001 for both day 4 and day 6) (Fig. 2B).
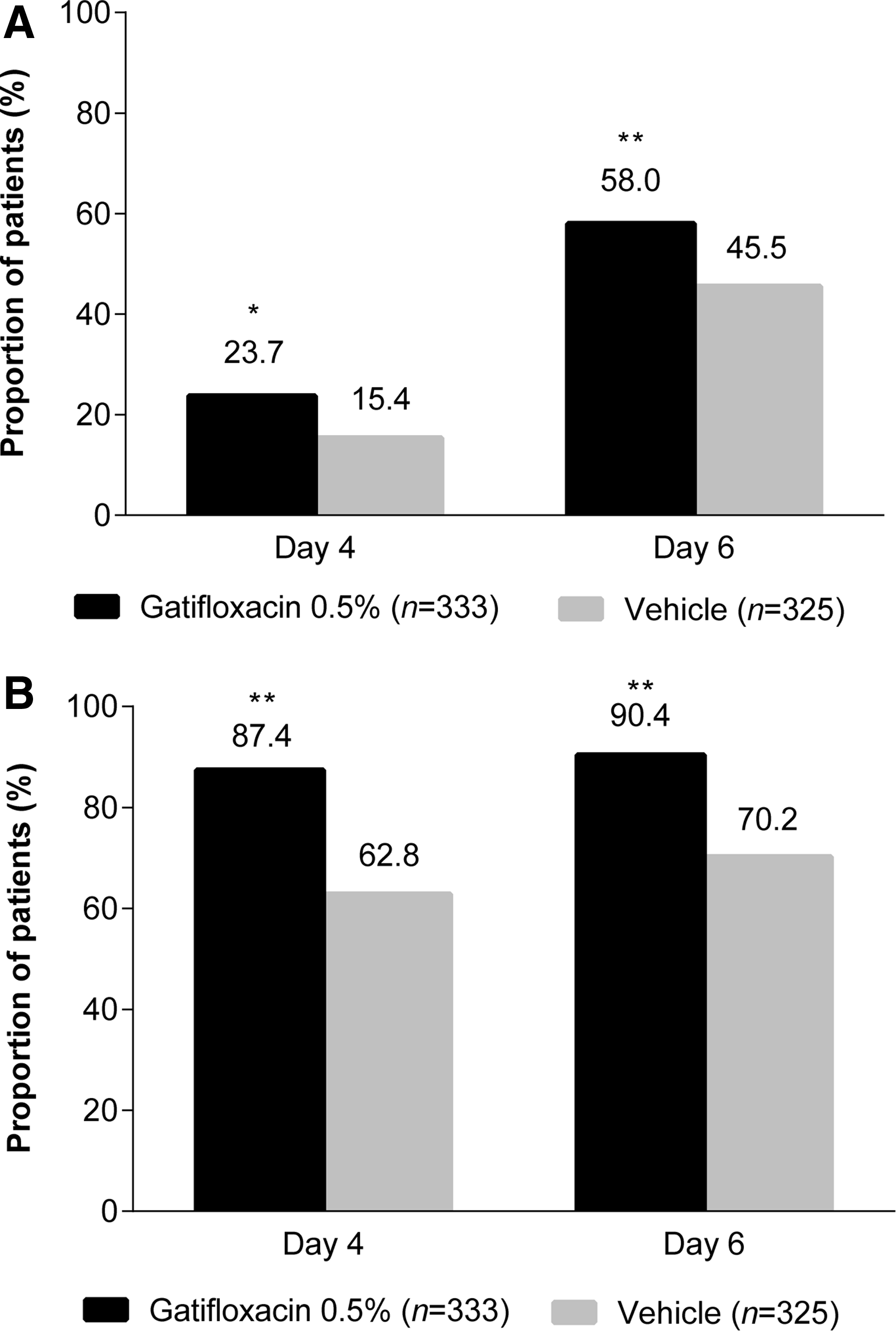
Proportion of patients with clinical success
Clinical improvement in ocular signs occurred in a higher proportion of patients in the gatifloxacin 0.5% group compared with the vehicle group at both day 4 (92.8% [309/333] vs. 87.1% [283/325]; P=0.015) and day 6 (96.1% [320/333] vs. 92.3% [300/325]; P=0.037) time points. Improvements in ocular symptoms in the study eye were recorded in the gatifloxacin 0.5% treatment group compared with the vehicle group at the day 4 (80.4% [267/332] vs. 74.1% [240/324]) and day 6 (87.7% [291/332] vs. 84.3% [273/324]) time points, but did not reach statistical significance.
Microbiological results
Bacterial isolates commonly identified at baseline in the mITT population are shown in Table 2; the most frequently identified organisms in a qualified eye in the gatifloxacin 0.5% and vehicle groups overall were H. influenza (20.1% and 17.5%), S. aureus (19.5% and 15.7%), Staphylococcus epidermidis (16.5% and 15.7%), and S. pneumonia (13.8% in both groups). The 5 most common organisms isolated in at least 5 patients in the qualified eye at baseline in the United States were H. influenza, S. pneumonia, S. aureus, S. epidermidis, and the Streptococcus mitis group, with MIC90s to gatifloxacin 0.5% ranging from 0.03 μg/mL to 2.0 μg/mL. In India, the 5 most common organisms were S. aureus, S. epidermidis, Staphylococcus hominis, Klebsiella pneumonia, and Pseudomonas aeruginosa, with MIC90s to gatifloxacin 0.5% ranging from 1.0 μg/mL to >8.0 μg/mL.
The combined MIC90 of gatifloxacin 0.5% for all organisms in any qualified eye was 2.0 μg/mL (Table 3). This was the same as the MIC90 of moxifloxacin and lower than the MIC90s for azithromycin, ciprofloxacin, erythromycin, gentamicin, tetracycline, and tobramycin, which ranged from 8.0 μg/mL to >32 μg/mL. The MIC90 of gatifloxacin 0.5% for all gram-positive bacteria combined was 2.0 μg/mL, which was the same as the MIC90 of moxifloxacin and lower than the MIC90s for azithromycin, ciprofloxacin, erythromycin, gentamicin, tetracycline, and tobramycin, which ranged from >8.0 μg/mL to >32 μg/mL. For gram-negative organisms, the combined MIC90 of gatifloxacin 0.5% was 2.0 μg/mL, which was the same as the MIC90 for tobramycin, higher than the MIC90 of ciprofloxacin (0.50 μg/mL), and lower than the MIC90s for moxifloxacin, azithromycin, erythromycin, gentamicin, and tetracycline, which ranged from 4.0 μg/mL to >32 μg/mL.
Sensitivity testing conducted for organisms above pathological threshold only and treatment groups were combined.
MIC90, minimum concentration required to inhibit 90% of isolates.
Safety results
Overall, treatment with gatifloxacin 0.5% was well tolerated, and the majority of AEs in both treatment groups were of mild or moderate severity. Across the pooled studies, there were 2 patients with serious AEs: one patient in the gatifloxacin group with a history of depression and anxiety who was hospitalized (for worsening depression and anxiety) a day after starting medication and another patient in the vehicle group who suffered congestive heart failure.
The incidence of all AEs regardless of causality for the pooled safety population was low and numerically lower in the gatifloxacin 0.5% (11.6% [83/717]) than in the vehicle group (13.3% [95/716]), although the difference was not statistically significant (P=0.332). The incidence of treatment-related AEs was 4.3% (31/717) in the gatifloxacin 0.5% group compared with 3.4% (24/716) in the vehicle group (P=0.338); only 2 treatment-related AEs, eye irritation and dysgeusia, were reported by 1% or more of patients but occurred in less than 3% of patients in any treatment group. AEs reported by 1% or more of patients in any treatment group are shown in Table 4.
P<0.04, Fisher's exact test.
P<0.05, Pearson's chi-square test.
There were no changes in visual acuity or biomicroscopy finding increases of 1 severity grade or greater from baseline to any follow-up visit, which occurred at a significantly greater frequency in the gatifloxacin 0.5% group than the vehicle group.
Discussion
Acute bacterial conjunctivitis is one of the most common eye disorders encountered by primary care physicians and urgent care centers.5,24 Results from this study suggest that gatifloxacin 0.5% ophthalmic solution administered twice daily for up to 5 days is effective for the treatment of acute bacterial conjunctivitis in patients 1 year of age or older. Gatifloxacin 0.5% was superior to vehicle treatment in the primary analysis; clinical success was achieved in the study eye at the day 6 time point using the up to day 6 analysis method in the pooled mITT population. Gatifloxacin 0.5% was also superior to vehicle treatment on the secondary efficacy variables of clinical success at the day 4 time point and for both microbiological cure and clinical improvement in ocular signs at the day 4 and day 6 time points.
Gatifloxacin 0.5% was administered twice daily to patients with acute bacterial conjunctivitis in this study. For products of this type, it is a typical practice to start treatment with a loading dose to kill a majority of the bacteria in the diagnosed eye(s). On the first day of treatment, a drop was to be administered every 2 h up to 8 times. Thereafter, dosing every 12 h was expected to be sufficient to kill the remaining bacteria, even those with a low level of resistance to the anti-infective. With reported increases in antibacterial resistance with ocular pathogens, including those that cause bacterial conjunctivitis,4,18 it is important that antibacterial ophthalmic solutions eliminate all bacterial isolates to help prevent the development of resistant variants.
The fourth-generation fluoroquinolones, gatifloxacin and moxifloxacin, were introduced to provide greater coverage against gram-positive organisms than earlier generations of fluoroquinolones, based on significant activity against both DNA gyrase and topoisomerase IV.25,26 Susceptibility testing from the current studies revealed that gatifloxacin 0.5% had an overall MIC90 of 2.0 μg/mL among all bacterial isolates from conjunctival samples collected at baseline (day 1). For all gram-positive organisms tested, the MIC90 of gatifloxacin was similar to that for moxifloxacin and lower than all other antimicrobial agents. For all gram-negative organisms, the MIC90 for gatifloxacin was similar to tobramycin and lower than all other antimicrobials tested except ciprofloxacin, which had the lowest MIC90. Overall, ciprofloxacin, a second-generation fluoroquinolone, had significantly lower potency relative to both gatifloxacin and moxifloxacin for gram-positive organisms. This is consistent with a previous in vitro study that found gatifloxacin and moxifloxacin to be superior to ciprofloxacin against gram-positive organisms, and ciprofloxacin to be most effective against gram-negative organisms from ocular infections. 27 In another study of bacterial isolates from ocular infections, a higher percentage of both gram-negative and gram-positive organisms were susceptible to gatifloxacin compared to other topical antibiotics, including ofloxacin, ciprofloxacin, norfloxacin, gentamicin, tobramycin, neomycin, chloramphenicol, erythromycin, tetracycline, and amikacinin. 28 As has been reported in other studies,3,4 the most common organisms identified at baseline were H. influenza, S. aureus, S. epidermidis, and S. pneumonia. Despite the different causative organisms, microbiological cure was observed with gatifloxacin 0.5% ophthalmic solution in nearly all patients enrolled in the study.
Overall, treatment with gatifloxacin 0.5% ophthalmic solution was safe and well tolerated. There were no differences in the incidence of general or ocular AEs between the gatifloxacin 0.5% and vehicle groups. The most frequently reported treatment-related AEs in either group were eye irritation and dysgeusia.
The study has some limitations, including comparing gatifloxacin 0.5% to vehicle treatment and not an active comparator, and both gatifloxacin 0.5% and vehicle products contained the preservative benzalkonium chloride that has antibacterial activity and may have affected outcomes.29–31 In addition, all conjunctival samples collected from patients across the study sites were shipped to an independent central laboratory in Indiana for susceptibility testing. Other studies have employed a similar design, including the Ocular Tracking Resistance in US Today (TRUST) study, a nationwide study involving 35 sites evaluating the antimicrobial susceptibility patterns in the United States. 32
Conclusions
Based on clinical success (defined as the proportion of patients with a score of zero for both conjunctival hyperemia and discharge at day 6), gatifloxacin 0.5% ophthalmic solution administered twice daily for 5 days was effective in treating acute bacterial conjunctivitis in patients enrolled at sites in both the United States and India. Microbiological cure was achieved with gatifloxacin 0.5% regardless of the wide variety of bacterial isolates and susceptibilities identified in vitro at baseline. No significant safety issues related to the study drug were observed with gatifloxacin 0.5% either in adults or in pediatric patients.
Footnotes
Acknowledgments
This study was sponsored by Allergan, Inc. (Irvine, CA). Writing and editorial assistance were provided to the authors by Kakuri Omari, PhD, and Gayle Scott, PharmD, of Evidence Scientific Solutions (Philadelphia, PA), and funded by Allergan, Inc. (Irvine, CA). All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Author Disclosure Statement
W.H., M.C., Y.R.B., and J.M.D. have no competing conflicts of interest; C.F., L.V., D.A.H., and H.J. are employees of Allergan, Inc. (Irvine, CA).