
Abstract
Abstract
Purpose:
To assess the efficacy of combined intravitreal bevacizumab (IVB) and macular grid and scatter laser photocoagulation in the treatment of macular edema secondary to branch retinal vein occlusion (BRVO) over a 12-month period.
Methods:
A prospective, interventional case series study was conducted in 20 patients. Patients were treated with 3 monthly IVB injections, followed by macular grid laser and scatter laser photocoagulation to nonperfused ischemic retina. Repeated IVB injections were performed on an as-needed basis when patients had recurrent macular edema.
Results:
The best-corrected visual acuity of 20/40 or better was achieved in 17 eyes (85%) and a vision gain of 3 lines or more was noted in 12/20 eyes (60%). Mean visual acuity improved from 0.68 logMAR at baseline to 0.28 logMAR at 3 months, 0.26 logMAR at 6 months, and 0.26 logMAR at 12 months (P<0.01). The mean central macular thickness (CMT) was 442 μm at baseline and decreased to 266, 264, 300, and 294 μm at 1, 3, 6, and 12 months' follow-up, respectively (P<0.01). A mild rebound CMT increase was noted at 6 months, which was reduced after bevacizumab reinjection. Ten patients (50%) required repeated IVB injections. Fifteen eyes (75%) have complete edema resolution on optical coherence tomography scan at the 12-month return visit. Overall, patients received an average of 4 injections during the 12-month period. No adverse ocular or systemic events were observed following injections.
Conclusions:
Early IVB injections in combination with subsequent macular grid and scatter laser photocoagulation treatment significantly improved vision and reduced macular edema secondary to BRVO. Further studies are warranted to evaluate the long-term outcomes and safety.
Introduction
R
The Branch Vein Occlusion Study (BVOS) group demonstrated the effects of grid laser photocoagulation treatment in 139 eyes of patients with macular edema following BRVO. 2 Since then, the grid laser has become the standard of care for BRVO. However, only 40% of eyes recover a visual acuity (VA) of 20/40 or better, and VA remains 20/200 or worse in 12%. The mean improvement of 1.33 lines of vision after 3 years in the BVOS still leaves many patients with substantial visual disability. In addition, visual improvement after laser therapy occurs very slowly. Furthermore, the macular edema and retinal hemorrhage in the acute phase of BRVO may preclude laser treatment, and it can take several months before laser can be used. Therefore, more effective therapeutic options are needed to improve vision more rapidly and effectively than with grid lasers alone.
Elevated intraocular levels of vascular endothelial growth factor (VEGF) have been demonstrated in the vitreous of BRVO.3,4 Increased VEGF, triggered by hypoxia, is a key mediator of intraocular neovascularization and macular edema.5–7 It can increase vascular permeability by increasing phosphorylation of tight junction proteins, such as occludin and zona occludens-1, subsequently resulting in macular edema. 8 Therefore, the inhibition of VEGF could theoretically provide a therapeutic advantage in macular edema and neovascularization. 9 Bevacizumab (Avastin; Genetech, San Francisco, CA) is a recombinant monoclonal antibody that binds all isoforms of VEGF-A. The systemic administration of bevacizumab is approved for metastatic colon cancer. Intravitreal injections of bevacizumab have been used to treat macular edema secondary to BRVO.10–14 Concerning other anti-VEGF agents, the BRAVO study showed that after 6 monthly ranibizumab (Lucentis; Genentech) injections, the mean gain from baseline in best-corrected visual acuity (BCVA) was 16.6 and 18.3 letters in the 0.3- and 0.5-mg ranibizumab groups, respectively, compared with 7.3 letters in the sham group. 15 After the initial 6 months, evaluations and as-needed treatments were carried out every month, and these significant improvements were maintained at month 12. 16
Our previous report demonstrated that intravitreal bevacizumab (IVB) monotherapy showed promising short-term functional and anatomical effects in the treatment of macular edema secondary to BRVO. 17 In that study, the effects of IVB occurred within 1 month, but did not last for more than 3 months. Therefore, multiple repeated injections were needed to maintain visual improvement. The retinal nonperfusion (RNP) ischemic area, which triggers the intraocular VEGF increase, is an important underlying cause of recurrent macular edema in BRVO. It may be possible to combine several therapeutic modalities to achieve a synergistic effect and decrease the frequency of injection. Herein, we present our experience with a prospective, consecutive case series of 20 patients treated with combined IVB and macular grid and scatter laser photocoagulation for the retinal nonperfused area in patients with macular edema secondary to BRVO over a 12-month study period. The aim of the current study was to evaluate the efficacy of this combined therapeutic option in the treatment of macular edema secondary to BRVO.
Methods
In this prospective, interventional case series study, patients diagnosed as having BRVO associated with macular edema were recruited and enrolled at Taipei Veterans General Hospital, Taipei, Taiwan, Republic of China. The study protocol, which followed the Declaration of Helsinki, was approved by the Institutional Review Board of Taipei Veterans General Hospital.
Study criteria and outcome measures
The inclusion criteria of this study were patients with a chief complaint of blurred central vision or metamorphopsia due to persistent macular edema secondary to the diagnosis of acute BRVO for at least 1 month. BRVO was defined as retinal hemorrhage, exudates, edema or other biomicroscopic evidence of RVO (eg, telangiectatic capillary bed), and a dilated, tortuous venous system in the quadrant of the retina drained by the affected vein. All enrolled patients had a VA of 20/50 or worse and a central macular thickness (CMT) of more than 250 μm, as measured by optical coherence tomography (OCT). The exclusion criteria were signs of concurrent ocular inflammation or infection, intraocular surgery (including postvitrectomized eyes) within the previous 3 months, uncontrolled blood pressure, recent history of stroke or myocardial infarction, and severe unstable systemic diseases. The patients who received intravitreal injections of any anti-VEGF drugs (ranibizumab or bevacizumab) or triamcinolone acetonide (TA) within the previous 3 months were also excluded.
The patients were initially treated with 3 monthly IVB injections (2.5 mg/injection in a volume of 0.1 mL), then followed by macular grid laser and scatter laser photocoagulation treatment to any nonperfused area observed by fluorescein angiography (FA).
The primary study outcome measure was defined as the proportion of patients gaining 3 lines or more of vision at 12 months. The secondary outcome measures were the mean change from baseline BCVA and the mean change in the central 1-mm macular thickness measured by spectral domain OCT (RTVue-100 SD-OCT; Optovue, Inc., Fremont, CA; Cirrus HD-OCT; Carl Zeiss Meditec, Dublin, CA). Prior systemic or ocular diseases associated with the occurrence of RVO and any ocular and systemic adverse events after the IVB injections were also evaluated and analyzed.
All of the patients signed a written informed consent form. The nature of off-label use of this drug and the potential side effects of endophthalmitis, retinal detachment, and the possibility of thromboembolic events were discussed with the patients before obtaining informed consent.
Ocular examinations
All patients received complete ophthalmic examinations before the injection, including Snellen BCVA measurement converted to a logarithm of the minimum angle of resolution (logMAR), intraocular pressure (IOP), indirect ophthalmoscopy, slit lamp biomicroscopy, fundus photography, and macular mapping using OCT at the first visit (baseline). After treatment, serial changes in VA and CMT were measured at 1-, 3-, 6-, 9-, and 12-month follow-up examinations after the injection. FA was performed at the initial examination and repeated as necessary during return visits.
Injection procedure and safety monitoring
Before injection, topical anesthetic eye drops were applied at least thrice. The injections were performed through pars plana under aseptic conditions in the operating room. The conjunctival sac and eyelid margin were rinsed with povidone-iodine solution. After application of a sterile drape, a lid speculum was inserted. Bevacizumab (Avastin; Genetech) was stored in a refrigerator at 4°C. The dosage of IVB in the injections was 2.5 mg (0.1 mL), which was injected using a syringe with a 30-g needle at a distance of 4.0 mm from the limbus in phakic eyes and 3.5 mm in pseudophakic eyes. Before injection, anterior chamber paracentesis was performed to maintain an adequate postoperative IOP. The injected site was compressed carefully using a sterile cotton-tipped applicator to prevent fluid reflux. After injection, the IOP and central retinal artery perfusion were checked, and antibiotic eye drops were applied 4 times a day for 1 week. The patients were then examined at an out-patient clinic on day 1 and every 4 weeks thereafter for 1 year. Systemic conditions were also monitored. Blood pressure was measured before the bevacizumab injection and at 1 week after injection. Other systemic conditions associated with RVO were assessed by a thorough review, including myocardial infarction, stroke, or other thromboembolic diseases.
Laser photocoagulation
After the third IVB injection, laser application was performed on a return visit with a pan-funduscopic TransEquator® lens (Volk Optical, Inc., Mentor, OH) based on the FA findings. Macular grid laser photocoagulation (spot diameter, 50–100 μm; exposure time, 100 ms; power, 80–125 mW) was applied over the previous leakage area at the macula outside the foveal avascular zone if the hemorrhage had cleared sufficiently to allow for safe application of the laser. Scatter laser photocoagulation (spot diameter, 200 μm; exposure time, 100–150 ms; power, 150–250 mW) was also applied to the sector of nonperfused ischemic retina outside the macula and up to the far periphery based on the FA findings. Additional grid and scatter laser photocoagulation treatment was allowed for any nonperfused areas by doctor's clinical judgment at the 6- and 9-month follow-up visit.
Reinjection criteria
Bevacizumab injections were repeated according to the clinical judgment of the doctors based on VA, biomicroscopic evaluation of the macula, and CMT on OCT. Repeated injections were performed on an as-needed basis when the patients had persistent or recurrent macular edema. Any of the following changes appearing during follow-up were criteria (indications) for repeated injections: (i) VA loss of at least 1 line of the Snellen chart with OCT evidence of fluid in the macula; (ii) an increase in CRT of at least 100 μm; and (iii) evidence of persistent fluid on OCT 1 month after the previous injection. All criteria were based on a comparison with the findings of the previous month.
Statistical analysis
Statistical analysis of the data was performed using SPSS software (version 15.0; SPSS, Inc., Chicago, IL). Serial changes in mean BCVA and CMT were recorded. BCVA was reported as logMAR VA for statistical analysis. The Wilcoxon t-test was used to assess differences between baseline and post-treatment data in mean logMAR BCVA and CMT. A P-value of<0.05 was considered to be statistically significant.
Results
A total of 20 consecutive patients (20 eyes) with persistent macular edema secondary to BRVO were enrolled and investigated in this study. The detailed baseline characteristics and outcomes of the patients are summarized in Table 1. Of the 20 patients, 12 were male and 8 were female with a mean age of 64.8±10.5 years (range: 47–83 years). The mean follow-up period was 14 months (range: 12–18 months). Fifteen patients had a history of hypertension (75%). Other medical conditions included diabetes mellitus (10%), hyperlipidemia (35%), coronary arterial disease (15%), and stroke (10%). In addition, 3 patients had glaucoma (15%).
BRVO, branch retinal vein occlusion; CAD, coronary arterial disease; CMT, central macular thickness; DM, diabetes mellitus; MAR, minimum angle of resolution.
After the initial 3 monthly IVB injections and subsequent laser photocoagulation, repeated IVB injections were performed on an as-needed basis. Ten patients (50%) required repeated IVB injections according to reinjection criteria, and the mean number of reinjections was 1. Overall, patients received an average of 4 injections during the whole 12-month follow-up period. The mean number of laser photocoagulation treatments following the bevacizumab injections was 2±1.
Visual acuity
The baseline mean BCVA with logMAR scale was 0.68±0.38 (n=20) (Table 2). There was a statistically significant improvement in VA after combined treatment, and the logMAR BCVA improved to 0.28±0.25, 0.26±0.25, 0.26±0.23, and 0.26±0.22 at 3, 6, 9, and 12 months, respectively, following treatment (P<0.01 compared with the baseline data at each time point) (Fig. 1). The final BCVA of 20/40 or better was achieved in 17 eyes (85%) at 12 months. Twelve of the 20 eyes (60%) showed a VA improvement of 3 lines or more on the Snellen chart. No patient had a loss of vision greater than 1 line at the 12-month visit.
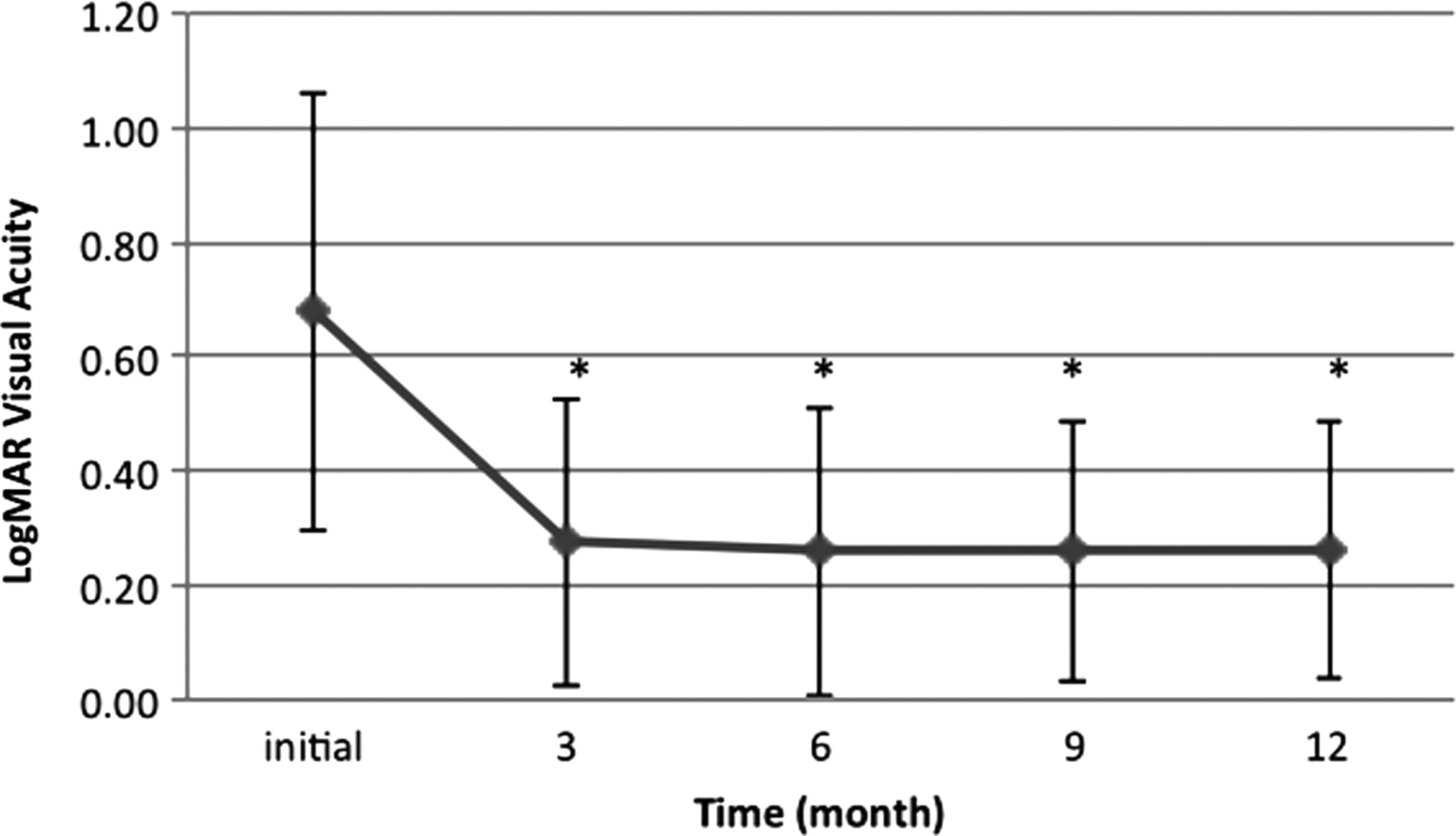
Mean best-corrected visual acuity (logMAR) at baseline, 3, 6, 9, and 12 months after combined intravitreal bevacizumab injections and laser photocoagulation in the patients with branch retinal vein occlusion (n=20). *P<0.01 compared with the baseline data at each time point. MAR, minimum angle of resolution.
OCT, optical coherence tomography.
Central macular thickness
The mean CMT measured by OCT at baseline was 442±140 μm (n=20) (Table 2). There was a statistically significant decrease in CMT after treatment, with measurements at 1, 3, 6, and 12 months of 266±63, 264±81, 300±96, and 294±69 μm, respectively (P<0.01 compared with the baseline data at each time point) (Fig. 2). However, there was a mild rebound in mean CMT increase to 300 μm at 6 months, which was then reduced after bevacizumab reinjection (Fig. 2). The fluctuation of CMT did not seem to impact significantly on vision. Fifteen eyes (75%) had complete edema resolution on OCT scan at the 12-month return visit.

Central macular thickness (CMT) measured by optical coherence tomography at baseline, 1, 2, 3, 6, and 12 months after intravitreal bevacizumab injections and laser photocoagulation in the patients with branch retinal vein occlusion (n=20). A mild rebound in CMT increase was noted at 6 months after injection. *P<0.01 compared with the baseline data at each time point.
The original nonperfused avascular area on FA imaging was decreased in all patients with no evidence of progression after combined IVB and laser treatment in our study. During the follow-up period, none of the patients showed any ocular adverse events such as glaucoma, endophthalmitis, uveitis, vitreous hemorrhage, or retinal detachment. No systemic adverse events such as cardiovascular or thromboembolic events were noted.
One patient who presented with acute BRVO and was treated with 3 IVB injections at baseline, 1, and 2 months and subsequent macular grid and scatter laser photocoagulation treatment is shown in Fig. 3.
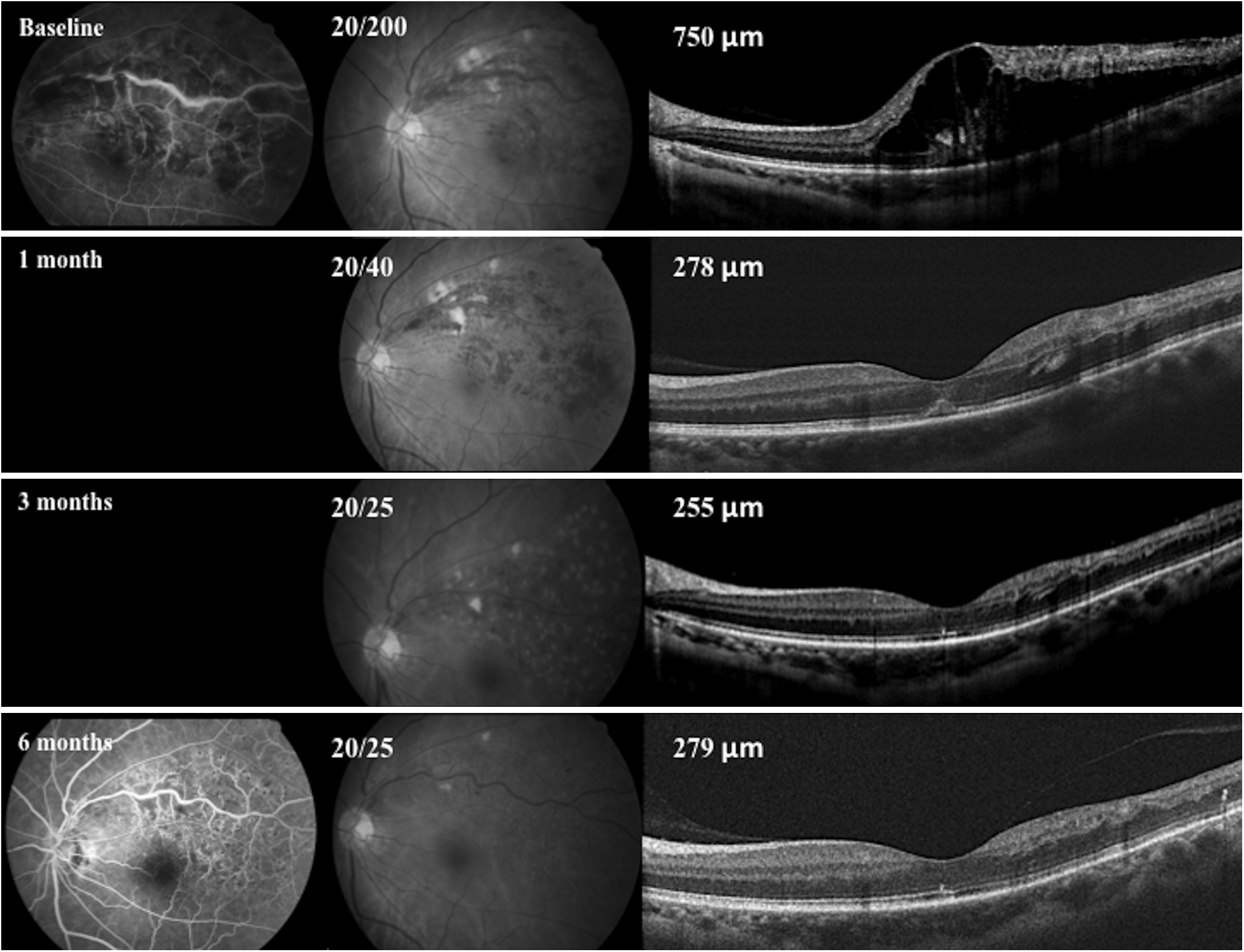
A 54-year-old male presented with marked subretinal fluid and severe cystoid macular edema secondary to branch retinal vein occlusion in the left eye. This patient received 3 intravitreal bevacizumab injections at baseline, 1, and 2 months and subsequent grid and scatter laser photocoagulation treatment. After 3 months, his visual acuity significantly improved from 20/200 at baseline to 20/25 associated with an obvious reduction in retinal thickness. After 6 months, his visual acuity remained stable, and follow-up fluorescein angiography showed no further fluorescein dye leakage and an obvious decrease in the nonperfused area.
Discussion
The present study demonstrated that IVB given in a 3-month loading regimen, followed by adjunctive macular grid and scatter laser photocoagulation, provided an additional benefit by reducing the number of repeated injections and maintained a substantial visual improvement in patients with macular edema secondary to BRVO after a period of 12 months.
In the acute phase of BRVO, there is profuse macular edema and retinal hemorrhage, which preclude laser treatment. Hemorrhage on the inner retina may absorb the laser energy and cause ganglion cell damage, which may lead to permanent visual field defects. It usually takes a few months for spontaneous hemorrhage absorption. In the BVOS, patients were observed for 3 months before laser treatment was considered. However, during that time permanent visual loss may occur due to severe macular edema and irreversible photoreceptor damage. Therefore, there is a need for earlier and more effective treatment for acute BRVO. Intravitreal pharmacological inhibition of VEGF could theoretically provide a therapeutic advantage for macular edema secondary to BRVO.
Intravitreal corticosteroids, TA, have been widely used to treat macular edema with diverse etiologies, including BRVO. The Standard Care versus Corticosteroid for Retinal Vein Occlusion (SCORE) study, which included 441 patients and a 12-month follow-up period, reported that intravitreal injection of TA did not obtain better results than those in the control group treated with grid laser photocoagulation. 18 Moreover, this treatment modality is limited by its potential complications of glaucoma, cataract, and endophthalmitis.19,20
Our previous study demonstrated that IVB showed promising short-term functional and anatomical effects in the treatment of macular edema secondary to BRVO, and that the effects of IVB occurred within 1 month, but did not last for more than 3 months. 17 Similar observations have been reported in the literature.10,11,13 Therefore, multiple repeated injections are needed to maintain visual improvements. The BRAVO study, a prospective randomized clinical trial, evaluated the efficacy of intraocular injections of ranibizumab for patients with macular edema following BRVO. 15 In the BRAVO study, patients were treated with 6 monthly injections of ranibizumab during the first 6 months, and then as needed for the next 6 months. The mean number of injections was 2.8, which were given from 7 to 12 months. 16 In addition, in the HORIZON study, which was an extension follow-up study of the BRAVO study, the mean number of reinjections was 2.1 for the second year of follow-up. 21 In an additional long-term study of RVO patients treated with ranibizumab, 50% patients of BRVO still required an average 3 injections during their fourth year of follow-up. 22 The main shortcoming of anti-VEGF agents (ranibizumab or bevacizumab) is the short duration of the effect, whereas laser photocoagulation has the advantage of better durability. We suggest that combining IVB with laser treatment may further decrease the intraocular VEGF loading and sustain the effect of bevacizumab. In the current study, after 3 bevacizumab loading injections, macular grid laser and scatter PRP were applied to the nonperfused ischemic retina. There were only 10 patients (50%) requiring repeated IVB injections. Overall, patients received an average of 4 injections during the 12-month follow-up period. Compared with previous reports in literature,15,16,21,22 the current study demonstrated that our patients maintained good visual outcome by fewer reinjections during the 12-month period.
In a pilot trial of anti-VEGF agents for patients with RVO, Campochiaro et al. reported that there is considerable variability in the treatment response. 23 The optimal dosing of IVB in treating BRVO has also yet to be determined. The doses of bevacizumab reported in the literature have ranged from 1.25 to 2.5 mg.8,9,24,25 In the current study, to maximize efficacy, we chose a higher dosing regimen of 2.5 mg to prolong the therapeutic effect and reduce the frequency of reinjections. The HORIZON trial also suggested that more aggressive treatment early on (higher dose or more frequent injections) is beneficial and may reduce the need for long-term reinjections. 21 In the current study, IVB was given in a 3 monthly loading 2.5-mg regimen, followed by adjunctive laser photocoagulation treatment.
The efficacy of grid laser photocoagulation for the treatment of macular edema in BRVO was confirmed in the BVOS trial. 2 In the ranibizumab–treated group in the BRAVO study, 36% to 43% patients underwent grid laser treatment.15,16 In the present study, by combining IVB with laser treatment we are able to use a relatively lower laser power setting (80–125 mW), which is a safer treatment protocol. There were no adverse events after grid laser treatment in our patients. Additionally, we suggest that the combined use of grid laser treatment may provide a long-term effect of better macular stability over the transient effect of decreased vascular permeability following anti-VEGF therapy. Donati et al. also reported that grid laser may reduce the number of IVB injections to control BRVO-induced macular edema. 26 In the current study, in addition to macular grid laser, scatter laser photocoagulation was also applied to the sector of nonperfused ischemic areas outside the macula and up to far peripheral regions where lesions were observed with FA. We suggest that scatter laser for peripheral ischemic retina may further decrease the VEGF loading and reduce the need for repeated bevacizumab injections over the long term.
The RNP area is an important driver of recurrent macular edema. Measurements of the area of RNP have shown that increases in the area of RNP are common in BRVO. 18 There is a clinical concern that anti-VEGF therapy may worsen the RNP in the natural course of RVO. However, the report by Campochiaro et al. demonstrated that treatment with ranibizumab did not worsen the RNP in patients with RVO, but rather reduced its occurrence compared with the sham-treated patients. 27 The authors provided an important insight regarding the pathogenesis and treatment of RVO, in that the initial vein occlusion causes baseline ischemia, subsequent release of VEGF, and leukostasis, which then contribute to the progression of RNP and thus worsening of ischemia. Infrequent anti-VEGF PRN injections may not be sufficient to prevent the progression of RNP, which may contribute to recurrent ME and loss of visual gain. 28 In the current study, after the initial 3 monthly bevacizumab loading regimen, we observed that the original nonperfused avascular area on FA imaging decreased without progression in all of the patients. The retinal nonperfused areas were also treated with adjunctive laser photocoagulation ablation, which may lead to the pharmacological therapy being more effective and durable. Our results suggest that decreasing the areas of RNP by dual therapy could eliminate the need for prolonged bevacizumab injections thereafter and shorten the disease course.
The limitations of this study included the relatively small number of patients and short-term follow-up period. There was no control comparison group of IVB alone without laser treatment. A long-term prospective study is essential to confirm the maintenance of the therapeutic benefits demonstrated in this study. Evaluation of any long-term ocular and systemic adverse effects is also mandatory.
In conclusion, the present study showed that early IVB injections in combination with subsequent macular grid and scatter laser photocoagulation treatment significantly improved vision and reduced macular edema in the patients with BRVO over a 12-month study period. Further studies are warranted to evaluate the long-term outcomes of combined IVB injections and laser treatment for BRVO and whether the need for reinjections can be reduced over time.
Footnotes
Acknowledgments
This study was supported by grants from the National Science Council (NSC98-2314-B075-003-MY2) and Taipei Veterans General Hospital (V100C-043, V99C1-009), Taiwan.
Author Disclosure Statement
No competing financial interests exist.