
Abstract
Abstract
Purpose:
The ideal notion of monthly intravitreal injections is difficult to achieve when it comes to real-life scenarios. In reality, patients often are treated with larger intervals due to circumstances. The purpose of this study was to compare the results of intravitreal bevacizumab injections with shorter intervals versus longer intervals for the treatment of choroidal neovascularization (CNV) in age-related macular degeneration (AMD) in a real-life clinic.
Methods:
A retrospective, consecutive cohort study of naive eyes of patients with CNV secondary to AMD treated with intravitreal bevacizumab. Patients included underwent at least 3 consecutive injections with intervals <45 days in between them (Group A) or >45 days (Group B). Best corrected visual acuity (BCVA) and optical coherence tomography were performed before the initial intravitreal injections and after the last injection.
Results:
Group A consisted of 24 eyes of 18 patients and Group B 30 eyes of 25 patients. There was a significantly larger mean of consecutive (5.0 vs. 3.78, P=0.013) and total (9.44 vs. 7.2, P=0.021) injections in Group B. There was a significant improvement in average BCVA in Group A only (0.65–0.52, P=0.006). However, a significant and similar improvement in retinal volume was found in both groups (P<0.05).
Conclusion:
This study emphasizes the importance of achieving consecutive injections with short intervals. Practitioners and decision makers should be mindful that providing additional resources to accomplish proper frequency may be more effective (visual outcome), cost effective (less injections), and safer (less exposure) for the patient.
Introduction
N
In recent years, new indications for intravitreal anti-VEGF have risen15–19 making monthly injections ergonomically difficult to achieve.5,20–22 In addition, patients themselves may miss an appointments due to anxiety from treatment-related pain and discomfort, 23 travel distance, 24 a need for a chaperon, 25 and other personal reasons. Thus, increased demand and low patient compliance may lead to delayed treatment in the form of larger intervals between injections in real-life scenarios.20–22
The purpose of this study was to compare the results of intravitreal bevacizumab injections with shorter intervals versus longer intervals for the treatment of CNV in AMD in a real-life clinic.
Methods
All data for this retrospective cohort study were collected and analyzed in accordance with the policies and procedures of the Institutional Review Board of the Meir Medical Center and the tenets set forth in the Declaration of Helsinki.
Study participants
The manually categorized registry of the Retina Clinic, Department of Ophthalmology of the Meir Medical Center was searched for all consecutive patients with CNV secondary to AMD, who were treated with intravitreal bevacizumab between January 1, 2011, and July 31, 2012. The standard of care in our department consists of 3 initial consecutive monthly intravitreal injections followed by administration pro re nata. 26 Inclusion criteria were patients with naive AMD who underwent 3 initial consecutive injections with intervals <45 days (Group A) or intervals >45 days (Group B) for the treatment of subfoveal CNV due to predominantly classic AMD. Patients who received the initial 3 injections at inconsistent intervals were excluded from this study. For example, patients were excluded if 1 or more of their injections qualified them for Group A and 1 or more of the initial 3 injections qualified them for Group B. Additional exclusion criteria were patients previously treated with laser photocoagulation, intravitreal triamcinolone, macular surgery, or photodynamic therapy, and patients with a history of glaucoma, diabetic retinopathy, uveitis, and macular disorders other than AMD, or a follow-up time of <12 months. Patients with retinal angiomatous proliferation (RAP) or significant pigment epithelial detachments (PEDs) were excluded.
Data collection
Each patient underwent BCVA measurement and ophthalmic examination, including slit-lamp biomicroscopy. Baseline fluorescein angiography was performed to verify the diagnosis. Optical coherence tomography (OCT, Stratus OCT; Carl Zeiss) testing was performed through a dilated pupil. The retinal volume of the 3.45 mm central retina was obtained using the macular thickness map. The scans were reviewed by a retina specialist and only high-quality scans were included. These were defined as scans with a signal strength >6 that exhibit correct delineation of the retina layers as detected automatically by the intrinsic software segmentation algorithm and are without image artifacts caused by eye movement and pupillary shadowing. Each patient underwent BCVA and OCT examinations before the initial injections and 1 month after the last one. The dose of bevacizumab injected was 1.25 mg/0.05 cc.
Statistical analyses
All data collected in the study were inserted into an electronic database using Microsoft Excel 2007 (Microsoft Corporation). Statistical analyses were performed using SPSS 21.0 (SPSS, Inc.). We compared both the baseline and outcome measurements of the treatment groups by using, whenever appropriate, Student's t-test or Kruskal–Wallis test. We used the chi-square or Fishers' exact test, as indicated, for analysis of categorical variables. Snellen BCVA values were converted to LogMAR units. A P value of <0.05 was considered significant.
Results
Out of a total of 250 patients receiving intravitreal injections during the study period, 54 eyes of 43 patients fulfilled the inclusion criteria. Reasons for being excluded were the initial 3 injections at inconsistent intervals (n=114), additional macular or retinal disorders (n=34), glaucoma (n=21), previous laser treatment (n=14), insufficient follow-up time due to being lost to follow-up (n=11), previous intravitreal triamcinolone injections (n=4), RAP (n=4), previous vitrectomy (n=3), and uveitis (n=2). The patient follow-up time ranged between 385 and 1,148 days. Group A included 24 eyes of 18 patients with a range of 25–44 days between injections. Group B included 30 eyes of 25 patients with a range of 45–60 days between injections. Table 1 depicts the demographic details and baseline characteristics of the groups. Both groups were similar in terms of age (74.2 vs. 75.1 years, P=0.67), gender (61% vs. 48%, P=0.40), mean baseline BCVA (0.65 vs. 0.61, P=0.74), and mean baseline central retinal volume (2.65 vs. 2.68 mL, P=0.84).
Group A received 3 initial bevacizumab injections with intervals <45 days, while Group B received the 3 initial injections with intervals >45 days.
BCVA, best corrected visual acuity; CI, confidence interval.
Table 2 depicts the outcomes of both the injection groups. Briefly, there was a significantly larger mean of consecutive (5.0 vs. 3.78, P=0.013) and total (9.44 vs. 7.2, P=0.021) injections in Group B. There was a significant improvement in the average BCVA Group A (0.65–0.52, P=0.006) with a nonsignificant trend toward deterioration Group B (0.61–0.66, P=0.404). A statistically significant difference was found in the change (delta) of BCVA between both groups (P=0.011) (Figure 1). A significant improvement in OCT volume was found in both Group A (2.65–2.29 mL, P=0.001) and Group B (2.68–2.35 mL, P=0.002). No statistically significant difference was found in the change (delta) of volume between both groups (P=0.406) (Figure 2).
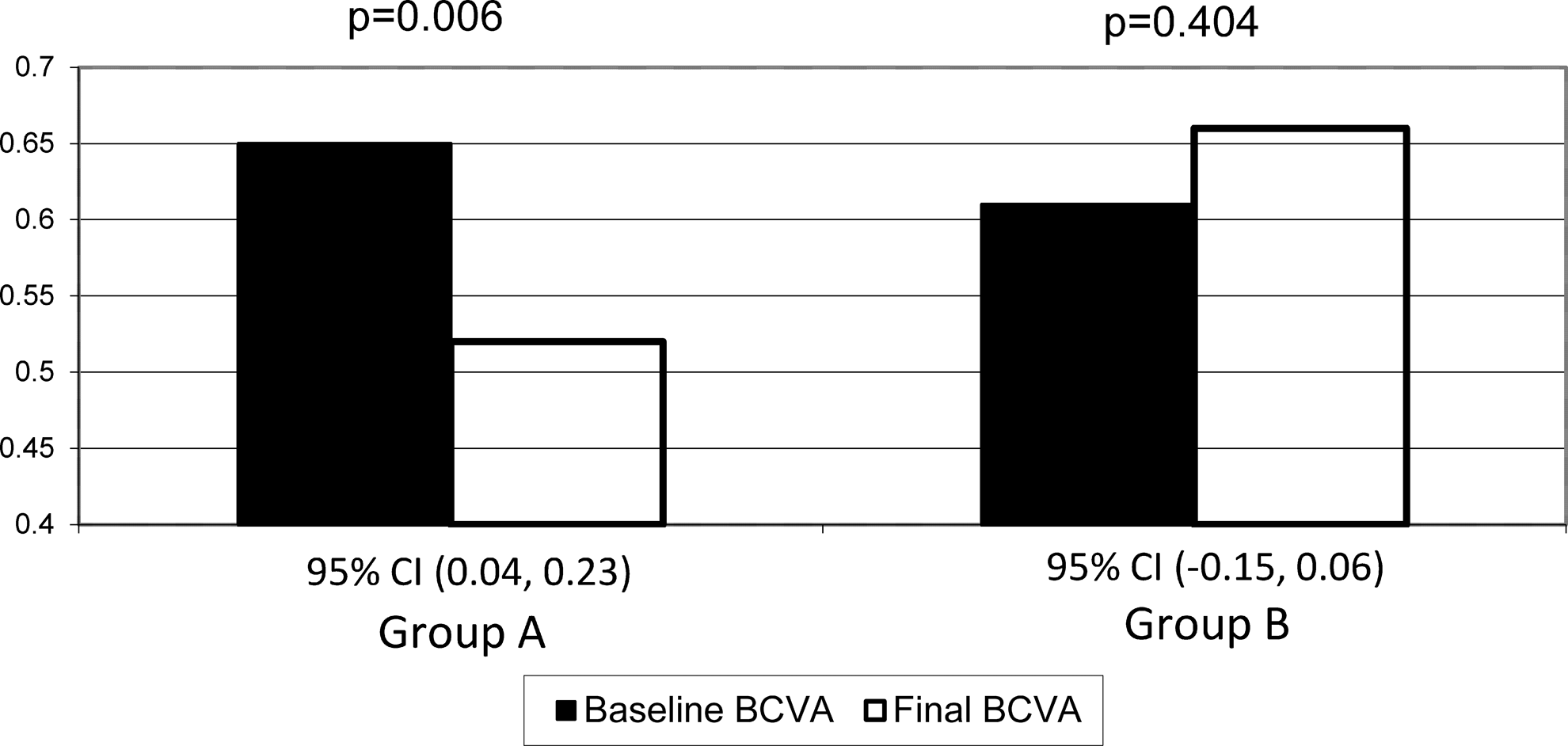
A comparison of the improvement in best corrected visual acuity (BCVA) between both injection groups. Only Group A experienced a significant improvement in BCVA.
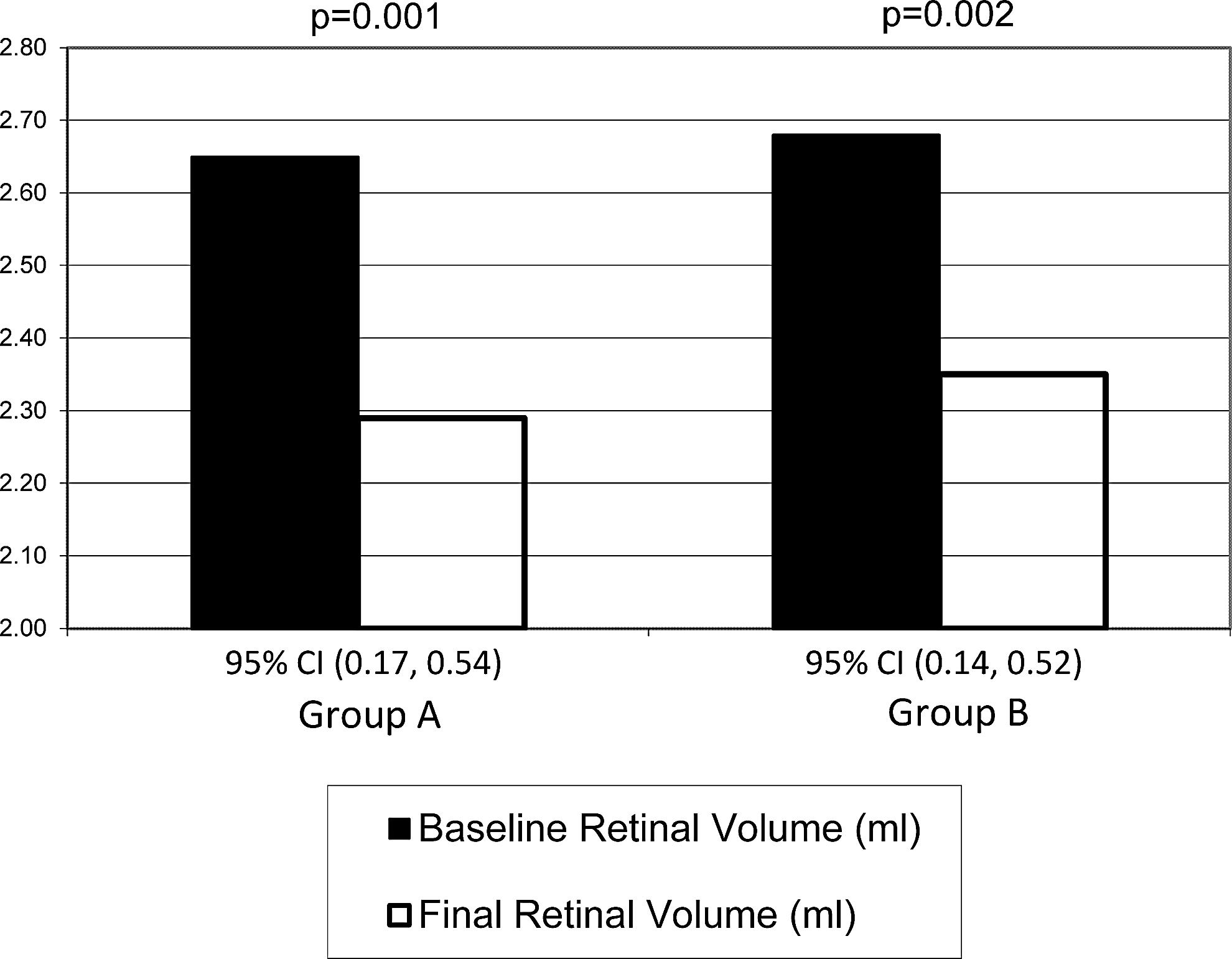
A comparison of the improvement in central retinal volume (mL) between both injection groups. Both groups experienced a significant improvement in terms of central retinal volume.
Group A received 3 initial bevacizumab injections with intervals <45 days, while Group B received the 3 initial injections with intervals >45 days.
Delta BCVA, final best corrected visual acuity – baseline best corrected visual acuity; Delta central retinal volume, final central retinal volume – baseline central retinal volume.
The post hoc statistical power values were above 0.70 for the primary outcomes.
No systemic or local complications such as vitreous hemorrhage, retinal detachment, or endophthalmitis occurred in either of the groups.
Discussion
In this study, we compared the results of intravitreal bevacizumab injections with shorter intervals versus longer intervals for the treatment of subfoveal CNV secondary to AMD in a real-life clinic.
This study demonstrated improvements in BCVA and central retinal volume in the group with shorter intervals (Group A). These findings are supported by those of previous studies that also reported improvement in these outcomes with similar intervals.3,10–14 The group treated with longer intervals (Group B) demonstrated a nonsignificant trend of BCVA deterioration. This finding is supported by that of Sonmez et al. who performed 3 initial injections of bevacizumab at 6-week intervals followed by 12-week intervals with the latter unable to maintain BCVA. 27 Similar findings were found with ranibizumab, in the EXCITE study, when comparing monthly and quarterly injections. 28 However, it is worth mentioning that in our study, Group B did demonstrate a significant improvement in OCT retinal volume (2.68–2.35 mL, P=0.002). This somewhat surprising finding, considering the nonimprovement in BCVA, is in fact supported by the findings of the EXCITE study. 28 In the EXCITE study, the monthly injection group achieved a better improvement in BCVA at 12 months when compared to the quarterly injection groups, whereas both groups demonstrated a significant and similar improvement in terms of central retinal thickness (CRT). This was explained by intermittent retinal thickening and a temporal association between functional and morphological changes. A recent subanalysis of the EXCITE study by Simader et al. 29 found that specific alterations in morphological parameters such as intraretinal cysts, subretinal fluid, and PEDs, significantly influence the potential for visual gain. They found that the association between CRT and BCVA became less evident during the follow-up and explained this as irreversible damage to the retinal architecture.
Group B underwent a larger number of consecutive and total number of injections (5.0 vs. 3.78, P=0.013 and 9.44 vs. 7.2, P=0.021, respectively). A study by Krebs et al. 30 comparing treatment of early AMD lesions versus advanced lesions found that the fluid in all compartments of early lesions was absorbed earlier than advanced lesions with longer lasting fluid deposits. Suboptimal treatment in the form of large intervals may also delay the absorption of fluid deposits and explain the need for more injections. Previous studies, investigating the effect of decreased intervals between injections (maintenance phase) following a 3-month period of monthly injections (initial phase), indicate that lower frequencies lead to a higher overall amount of injections and worst visual outcomes.27,28 Sonmez et al. reported worst visual outcomes and OCT findings when applying a 6-week injection interval for 3 months followed by a 12-week interval when compared to more frequent dosing. 27 In the EXCITE study, a comparison of monthly and quarterly ranibizumab injections following 3 initial monthly injections demonstrated that at 12 months, BCVA gain in the monthly regimen was higher compared with the quarterly regimens. 28 Unlike this study, the aforementioned did not investigate the effect of increased intervals during the initial phase itself, as sometimes encountered in real-life situations.
An important limitation of this study is its retrospective nature. However, based on previous studies and their findings, it would be unethical to intentionally treat patients with intervals of more than 6 weeks. An additional limitation of this study is its small sample size. However, when performing a post hoc analysis of the power, we found it to be relatively sufficient with a value above 0.70 for the primary outcomes of BCVA and retinal volume changes. Although BCVA and OCT measurements performed before and after sequential injections may misrepresent the fluctuative nature of large intervals, 28 it may provide a better insight regarding the differences between groups, which may no longer be apparent after many injections and a long treatment duration.
A potential limitation of this study is that the best treatment interval is not necessarily associated with the best schedule for observation. In our study, we did not report and analyze the observation intervals and therefore the possibility to differentiate between response and activity and to identify additional influential factors is limited.
Another limitation is that one cannot exclude that the response (BCVA) may have affected subsequent adherence. This may have led patients with a gain of BCVA to have shorter observation intervals and therefore questioning the causality between observation intervals and the outcomes of the study. Potentially, future prospective studies could address this issue with strict methodology; however, when considering the outcomes of this study, this may no longer be considered an ethical study to consider prospectively as one group will most probably be intentionally receiving subpar treatment.
In summary, this study supports the current literature regarding the need to inject bevacizumab with intervals shorter than 6 weeks. This emphasizes that a compromise in the form of intervals larger than 45 days is insufficient. Performing injections every 6 weeks or less leads to a better BCVA and fewer injections. Therefore, improving the awareness of practitioners to the importance of achieving monthly intervals between injections, especially throughout the initial phase, is warranted. 21 In addition, decision makers should be mindful that providing additional resources may be more effective (visual outcome), cost effective (less injections), and safer (less exposure) for the patient.
Footnotes
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
Author Disclosure Statement
No competing financial interests exist.