
Abstract
Abstract
Purpose:
To evaluate some clinically important features of benzalkonium chloride (BAK) toxicity by comparing tafluprost with 0.001% BAK and travoprost preserved with SofZia applied to the ocular surface of the eyes with glaucoma.
Methods:
This was a prospective, randomized, observer unmasked, multicenter crossover trial. A total of 195 patients were randomized and 174 patients completed the study at 19 clinics between November 2011 and August 2012. Topical BAK-preserved tafluprost or SofZia-preserved travoprost was newly administered or continued. Superficial punctate keratopathy (SPK), tear break-up time (BUT), the conjunctival hyperemia score, and intraocular pressure (IOP) were compared at the baseline visit, 4, and 12 weeks after the start of therapy. The eye drops were switched to another eye drop after 12 weeks of observation.
Results:
The total SPK and conjunctival hyperemia scores were significantly lower in the tafluprost compared with those in the travoprost phase (both P=0.038). There were no significant differences in the SPK scores of the superior area (P=0.679), central area (P=0.089), inferior area (P=0.090), and tear BUT (P=0.271). The IOP-lowering effects were similar (P=0.155).
Conclusions:
SPK, hyperemia score, and tear BUT while using tafluprost with 0.001% BAK were not inferior compared with those caused by travoprost with SofZia.
Introduction
G
Recently, ocular surface diseases caused by the preservatives in eye drops have been a focus of attention. 7 The addition of preservatives to eye drops for glaucoma therapy may induce ocular surface disease, with signs such as pain or discomfort during instillation, a foreign body sensation, stinging or burning or eyelid itching, superficial punctate keratopathy (SPK), or worsening of ocular surface disease.8–11 Furthermore, glaucoma patients are presumably at a higher risk for developing ocular surface disease, in part, due to the fact that both diseases are more common in older patients. 12 Therefore, attempts are being made to avoid the use of BAK as a preservative to reduce the incidence of ocular surface disease. Travoprost is a prostaglandin F2α analog preserved by SofZia, ionized Zinc in a solution buffered with borate, and sorbitol instead of BAK. Some researchers have reported that travoprost preserved with SofZia is less toxic to the ocular surface than latanoprost preserved with 0.02% BAK.10,13–16 Tafluprost is also a prostaglandin F2α analog containing 0.001% BAK. BAK is not a chemical with a single structure, but rather a mixture of dodecyl, tetradecyl, and hexadecyl dimethylbenzylammonium chloride. It is necessary to select the optimal concentration and combination of BAK to reduce the frequency of ocular surface diseases and maintain the power of BAK preservatives.17,18
The composition of BAK in topical tafluprost optimizes the preservative effects and minimizes ocular surface damage in cultured human corneal epithelial cells. 7 However, the effects of optimized BAK on the ocular surface in glaucoma patients have not been fully investigated. In this study, we prospectively evaluated the ocular surface changes and IOP-lowering effects of tafluprost with optimized 0.001% BAK and topical travoprost preserved with SofZia in patients with glaucoma. To accomplish this, we investigated the SPK score, tear break-up time (BUT), conjunctival hyperemia score, and IOP in Japanese patients who received tafluprost preserved with 0.001% BAK or travoprost preserved with SofZia in a crossover, randomized, multicenter prospective study.
Methods
The study was conducted in accordance with the tenets of the Declaration of Helsinki, and the protocol was approved by all the Review Boards of participating institutes. This study was registered in the University Hospital Medical Information Network (UMIN): UMIN000006621, and written informed consent was obtained from all participants before enrollment.
Design
This study was a prospective, randomized, multicenter, observer unmasked, 12-week, crossover-controlled clinical trial comparing the efficacy and safety of tafluprost (0.0015%) with BAK (0.001%) and travoprost with SofZia (0.004%) in patients with glaucoma or ocular hypertension. The trial was conducted from November 2011 to August 2012 at 19 sites in Japan.
Patients
Males and females, 20 years of age or older, with a diagnosis of primary open-angle glaucoma (POAG) or ocular hypertension were eligible. Treatment-naïve patients and those who were receiving prostaglandin analog treatment regimen that began at least 12 weeks before the screening visit were eligible. The subjects receiving combined therapy with the individual component of prostaglandin analog and beta-blocker eye drops (11 eyes) were also included.
The exclusion criteria for ophthalmic conditions were the presence of conditions where Goldmann applanation tonometry readings are unreliable, including corneal injury and marked corneal distortion, the use of contact lenses, inflammatory ocular surface disease, anterior/posterior uveitis (either eye within 6 months of screening), ocular infection, laser treatment or ocular surgery within the previous year, and pregnancy. Eyes with an increased IOP under the study protocol and those requiring additional IOP-lowering therapy (additional IOP-lowering eye drops, laser treatment, and ocular surgery) were excluded from this study. We did not include the subjects with dry eyes. We also excluded the subjects taking a fixed combination of prostaglandin analogs and timolol.
Procedures and assessments
After signing the Institutional Review Board-approved informed consent document, each subject underwent a comprehensive initial ocular examination, including slit-lamp biomicroscopy, gonioscopy, and fundus examination. The IOP was measured using Goldmann applanation tonometry and slit-lamp examinations were performed to evaluate the ocular surface, including the tear BUT and the presence of SPK and hyperemia. We used the data from only 1 eye for each patient, and when both eyes met the inclusion criteria, we analyzed the data for the right eye.
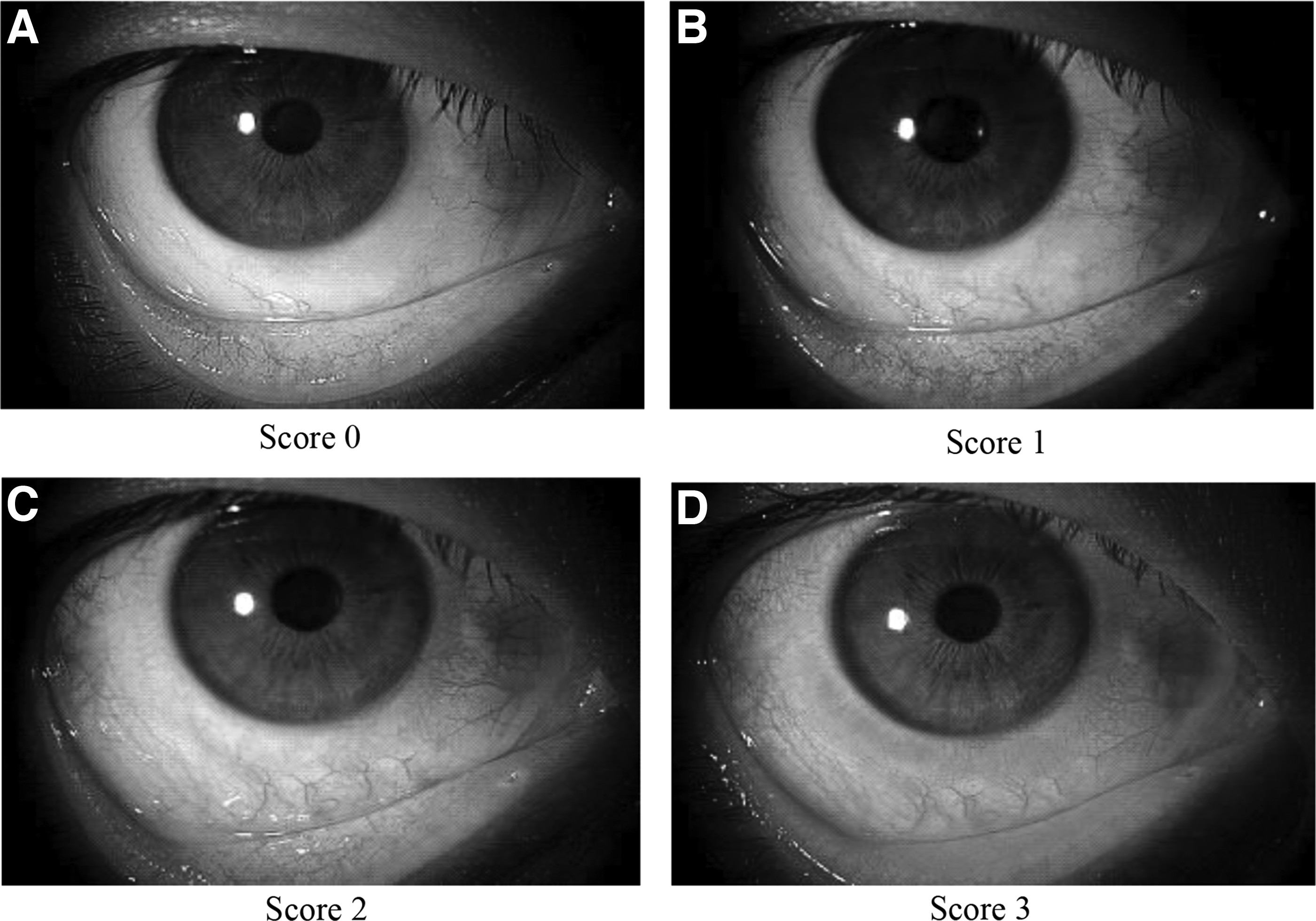
The presence of SPK in one-third of the superior area, the central area, and one-third of the inferior area was evaluated separately based on a grade of 0 to 3. The SPK scores of 3 sectors were totaled to determine the degree of SPK in the total area. The maximum value for the total SPK was 9 (Fig. 1). 19 The presence of conjunctival hyperemia was evaluated using standard grading photographs (Fig. 2). The degree of conjunctival hyperemia was graded from a score of 0 to 3. The BUT was examined thrice, and the average value was determined. Changes in various ocular surface indicators (Δhyperemia score, Δsuperficial punctate keratitis score, and Δtear BUT) and the IOP (ΔIOP) at each time point from baseline were assessed.

Cornea segment sectioning for staining scores. The presence of superficial punctate keratopathy (SPK) in one-third of the superior area, the central area, and one-third of the inferior area was evaluated separately based on a grade of 0 to 3. Score-0 indicates no staining. Score-1 indicates partial staining of less than half of the area. Staining of more than half of the area was evaluated as score-2, while staining of the entire area was evaluated as score-3. The SPK scores of 3 sectors were totaled to determine the degree of SPK in the total area. The maximum value for the total SPK was 9.
Photographs used to score hyperemia.
All subjects who agreed to join this study, including those newly diagnosed with POAG and ocular hypertension, were placed on tafluprost treatment (tafluprost 0.0015% with 0.001% BAK as the preservative; Tapros®; Santen Pharmaceutical Co., Ltd., Osaka, Japan) or travoprost treatment (travoprost 0.004% with SofZia® as the preservative; TravatanZ®; Alcon Japan, Inc., Tokyo, Japan). The subjects were randomly assigned to the tafluprost first and travoprost first treatment groups using the envelope method. The subjects using PG eye drops switched their medication to tafluprost or travoprost without a washout period. Both tafluprost and travoprost were prescribed at a dose of 1 drop every 24 h (administered at night). The subjects were withdrawn from this study when the doctors either found severe side effects, thus judged it to be impossible to continue the study, or when the subjects did not want to continue participating in this study for any reason.
Four and 12 weeks after the start of the topical treatment, the subjects underwent a comprehensive ocular examination between 9 and 12 AM, including an assessment of the ocular surface condition (SPK) and tear BUT, and slit-lamp biomicroscopy to assess the degree of conjunctival hyperemia and tonometry using a Goldmann applanation tonometer. After 12 weeks, the second treatment period began. During the second treatment period, the drugs were administered in the 2 groups using a crossover method. Measurements and assessments identical to those conducted during the first treatment period were performed. The ocular surface condition and IOP were evaluated at weeks 4 and 12 in the second treatment period.
Sample size
The primary hypothesis was that tafluprost with BAK would be noninferior to travoprost with SofZia with respect to changes in the ocular surface condition (SPK) from baseline to 12 weeks after the initiation of therapy. The minimum sample number to detect up to 80% of a 0.2 difference in the SPK score between the 2 treatment phases and a P-value of 0.05, assuming a standard deviation of 0.4, 20 was 63 subjects per phase.
Statistical analyses
The baseline characteristics of the subjects randomized to the tafluprost and travoprost treatment phases were statistically analyzed using the Mann–Whitney U test for data without normal distribution (gender, diagnosis distribution, conjunctival hyperemia scores) and the t-test for other data with normal distribution. The main outcome was the comparison of the SPK scores between the 2 phases. The differences in the rates of conjunctival hyperemia, tear BUT, and IOP were the secondary outcomes.
The IOP values, SPK score, hyperemia score, and changes in tear BUT after 12 weeks of therapy (at baseline and 4 and 12 weeks) were evaluated using a mixed-effects model repeated measures ANOVA, and the paired t-test was used to compare each time point within the ANOVA. Using that test, the group effect (difference between the tafluprost phase and travoprost phase), the time effect (differences at 4 and 12 weeks), and the interactions between the time and group effects (whether the effect of some phase increased with time) were examined.
Intragroup comparisons of SPK, conjunctival hyperemia score, BUT, and IOP measurements raw data were carried out using the 1-way ANOVA. Carryover tests were performed for all parameters based on the methods of Littell et al. 21 All analyses, except for the carryover tests, were performed using the software SAS Version 9.2 for Windows (SAS Institute, Tokyo, Japan). The carryover tests were performed using the JMP 9.0 version software program (SAS Institute, Inc., Cary, NC). The significance level was set at P<0.05. We performed the per-protocol analysis first and added the intent-to-treat analysis for the obtained data.
Results
One hundred seventy-four eyes of 174 patients from the 195 enrolled participants completed the study. Eighty-one patients received tafluprost treatment first, while 93 patients received travoprost first.
The demographics and frequencies of a prostaglandin analog history among the tafluprost to travoprost and travoprost to tafluprost groups are presented in Table 1. The differences in the demographics between these 2 groups were not significant. In both groups, ∼70% of the patients had previously used prostaglandin analogs. Forty-six subjects (26.4%) were newly diagnosed with POAG or ocular hypertension and naive to eye drops. One hundred sixty-three subjects (93.7%) were under prostaglandin monotherapy, and 11 subjects (6.3%) were using prostaglandin and beta-blockers.
The values are presented as the mean±standard deviation.
BUT, break-up time; IOP, intraocular pressure; M/F, male/female; POAG, primary open-angle glaucoma; SPK, superficial punctate keratopathy.
Both tafluprost-BAK and travoprost-SofZia were well tolerated over the 24-week treatment period. Discontinuation rates were reported with a similar incidence in both treatment phases (13 eyes and 8 eyes, which comprised 6.8% and 4.4% of the patients in the tafluprost-BAK and travoprost-SofZia phases, respectively). The adverse event was found in 1 eye (0.52%) in the tafluprost-BAK phase and 4 eyes (2.2%) in travoprost-SofZia phase. The drug-related adverse event was an increase in eye discharge in the tafluprost-BAK phase. Allergic conjunctivitis and pain were found in the travoprost-SofZia phase. The number of patients who discontinued visits to the hospital was 7 subjects (3.7%) in the tafluprost-BAK phase and 1 subject (0.54%) in the travoprost-SofZia phase. Six subjects preferred to use their prior eye drops after entering the study. One subject died of bile duct cancer. One subject broke his back during the study period and was unable to continue visits.
After 12 weeks of the treatment period, a comparison of the total SPK score demonstrated a significant difference between tafluprost and travoprost (P=0.038, Fig. 3A). There were no significant differences of treatment–time interactions or time with respect to the SPK of the total area of the cornea (P=0.654 and P=0.541, respectively). Regarding the comparison of the SPK in superior, center, and inferior scores, there were no significant differences of treatment (P=0.679, P=0.089, and P=0.090, respectively; Fig. 3B–D). The interaction between treatment and time with respect to the tear BUT was not significant (P=0.876), and the tear BUT values at different time points were similar (P=0.978). There were no differences in the tear BUT values between the tafluprost and travoprost phases (P=0.271), as shown in Fig. 4A. In addition, the conjunctival hyperemia scores were significantly different between the tafluprost and travoprost phases (P=0.038, Fig. 4B). However, time did not significantly affect the hyperemia scores (P=0.945). The hyperemia scores of all subjects at week 4 were significantly higher than those observed at baseline (P=0.041; paired t-test), whereas the differences between the week 12 values and baseline values (P=0.113) and between the week 4 and 12 values (P=1.000) were not significant. The interaction between treatment and time was not significant (P=0.660).
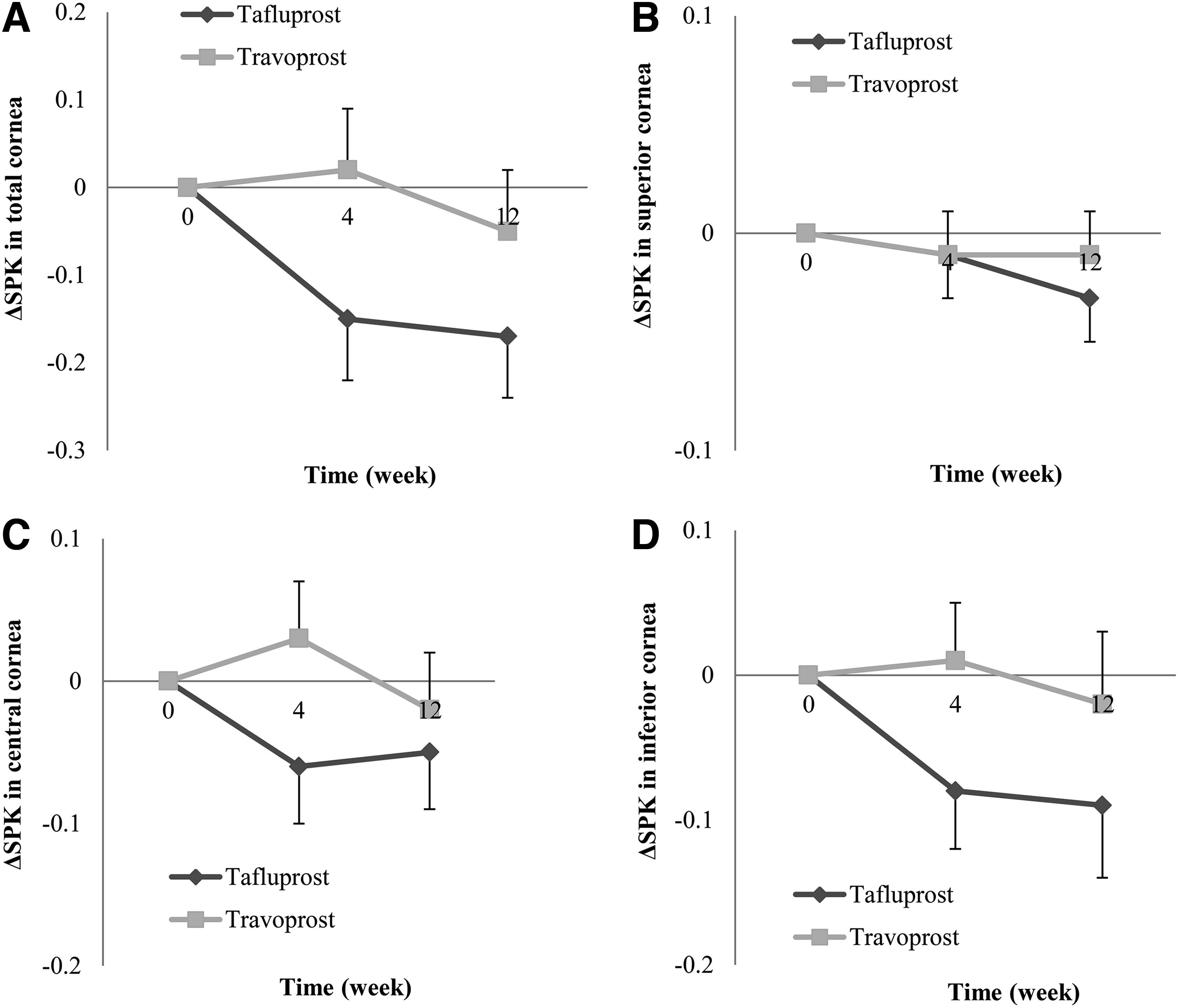
Changes in the superficial punctate keratopathy score (ΔSPK) in the tafluprost–benzalkonium chloride (BAK) and travoprost-SofZia groups (mean±standard error), treatment differences were evaluated using a mixed-effects model repeated measures ANOVA for

Changes in the tafluprost-BAK and travoprost-SofZia groups (mean±standard error), treatment differences were evaluated using a mixed-effects model repeated measures ANOVA in the
For those who had previously received prostaglandin analog treatment, the conjunctival hyperemia scores during the travoprost phase were significantly higher than those in the tafluprost phase (P=0.042). For those naive to glaucoma treatment, there was no significant difference between the scores during the travoprost and tafluprost phases (P=0.471).
The mean IOP of all subjects significantly decreased from baseline (P<0.0001 at week 4, P=0.0012 at week 12; paired t-test) with no significant differences between weeks 4 and 12 (P=0.612). The differences in the level of reduction of the IOP between the tafluprost and travoprost phases were not significant (P=0.155, Fig. 4C). Furthermore, the interaction between time and treatment was also not significant (P=0.882).
The carryover tests showed insignificant values for the SPK total scores (P=0.127), SPK superior scores (P=0.765), SPK central scores (P=0.786), tear BUT values (P=0.67), and IOP values (P=0.068). The carryover tests were significant for the SPK inferior values (P<0.0001) and the presence of conjunctival hyperemia (P=0.006).
The changes in the raw SPK score, BUT, hyperemia scores, and IOP are shown in Tables 2 and 3. There were no significant differences between the tafluprost and travoprost phases and the intragroup at any parameter.
The values are presented as the mean±standard deviation. The intragroup difference was analyzed using ANOVA.
ANOVA, analysis of variance.
The values are presented as the mean±standard deviation. The intragroup difference was analyzed using ANOVA.
After deleting subjects being treated concomitantly with a beta-blocker and prostaglandin analogs and prior bimatoprost users, a comparison of the difference in the level of the total SPK score, tear BUT, hyperemia score, and IOP demonstrated no significant difference between tafluprost and travoprost (P=0.058, P=1.000, P=0.053, and P=0.844, respectively).
Intent-to-treat analysis using mixed-effects model repeated measures ANOVA showed that the total SPK score of the travoprost phase was higher than that of the tafluprost phase (P=0.027). However, other parameters did not show any significant difference.
Discussion
Ocular surface disease is characterized by inadequate tear quantity and quality coupled with disruption of the integrity of the ocular surface involving the lid, conjunctiva, and cornea. 22 SPK is one of the most severe conditions caused by ocular surface disease, and chronic SPK can cause the loss or depletion of corneal stem cells. 23 For these reasons, we set the SPK score as the main outcome measurement. Our results showed the SPK scores in all corneal areas in eyes treated with BAK-preserved tafluprost to be smaller than those observed in the eyes treated with SofZia-preserved travoprost by both the per-protocol analysis and intent-to-treat analysis. The differences were not significant, except for the SPK scores of the total corneal area. Aihara et al., 15 in a prospective open-label study, and Yamazaki et al., 14 in a prospective uncontrolled study, found significant differences in the SPK scores for the entire cornea after switching from 0.02% BAK-preserved latanoprost to SofZia-preserved travoprost. These results indicate that SofZia-preserved travoprost has beneficial effects on the ocular surface while exhibiting a comparable IOP-lowering efficacy to that of BAK-preserved latanoprost. SofZia-preserved travoprost is recognized to be a safer prostaglandin eye drop than BAK-preserved eye drops. Our results also showed that tafluprost with 0.001% BAK is associated with a low incidence of ocular surface damage, especially in the cornea, similar to that observed with SofZia-preserved travoprost.
The hyperemia scores at week 4 were significantly higher than those observed at baseline likely because we included subjects naive to prostaglandin treatment. We found significant differences between the subjects treated with BAK-preserved tafluprost and SofZia-preserved travoprost by per-protocol analysis, but not by the intent-to-treat analysis. Previous studies reported no significant difference of those prostaglandin drops with and without BAK.16,24,25 A meta-analysis recently reported that latanoprost is associated with a lower incidence of conjunctival hyperemia than bimatoprost and travoprost in the treatment of ocular hypertension and/or glaucoma. 26 The reason for the reduction in hyperemia caused by latanoprost is likely due to the structure of the latanoprost molecule and its pharmacological receptor profile. 27 These findings suggest that the incidence of hyperemia may also be influenced by the prostaglandin molecule itself.
Although our results showed the significant differences in total SPK and hyperemia score, the differences were small. We are not sure whether these significant differences are clinically significant or not. Conjunctival hyperemia score was evaluated in all patients regardless of baseline treatment status and this significant change versus baseline is likely the contribution of treatment-naïve patients. The results may be different if the subgroups were analyzed (treatment-naïve, prostaglandin analog treatment). We analyzed hyperemia score changes in the treatment-naïve group and the prior latanoprost treatment group during the first treatment period. We could not see any significant hyperemia score difference between the BAK-preserved tafluprost group and SofZia-preserved travoprost group in treatment-naïve subjects maybe because of the small number of subjects.
When the tear BUT is decreased, the ocular surface easily becomes desiccated. One study found no significant differences between bimatoprost (preserved with 0.005% BAK), latanoprost (preserved with 0.02% BAK), and travoprost (preserved with SofZia) with respect to the BUT after 3 months of treatment. 25 In contrast, 2 studies reported an improvement in the tear BUT values among patients switched from BAK-preserved latanoprost to SofZia-preserved prostaglandin analogs.16,28 In the present study, we found no significant differences in the tear BUT values between the patients treated with BAK-preserved and SofZia-preserved prostaglandin analogs. Our results showed that tafluprost with 0.001% BAK is associated with a low incidence of ocular surface damage similar to that observed with SofZia-preserved travoprost.
In this study, we found no significant differences in the IOP-lowering effects of tafluprost 0.0015% and travoprost 0.004%. This finding is similar to that of previous studies of patients with normal-tension glaucoma. 29 Kawaguchi et al. compared the treatment efficacy of latanoprost, SofZia-preserved travoprost, tafluprost, and bimatoprost using bilateral therapy in normal subjects and showed that the mean diurnal IOP reduction achieved with latanoprost on days 7 and 14 was similar to that observed following treatment with travoprost and tafluprost. 30 One study using an animal model showed that BAK does not affect the corneal penetration of a prostaglandin analog, tafluprost, into rabbit aqueous humor. 31 Our results support the previous findings that the IOP-lowering efficacy is not influenced by reducing 32 or eliminating24,33 BAK from the formulation in patients with glaucoma or ocular hypertension.
Although this was a prospective study, we switched the eye drops without setting a washout period. This is one limitation of this study. However, we selected this protocol for ethical reasons to prevent the progression of glaucoma. Randomization and carryover tests were performed to overcome this limitation. The carryover test results showed significant values for the SPK inferior and conjunctival hyperemia scores. Nevertheless, we observed underestimation of the SofZia-preserved travoprost mean values and overestimation of the BAK-preserved tafluprost mean values for the SPK inferior and conjunctival hyperemia scores at week 12. These findings indicate that the actual differences in these 2 parameters were higher than that obtained in this study, resulting in smaller P-values. Therefore, the carryover test results do not change the conclusion that BAK-preserved tafluprost is a safe eye drop with respect to ocular surface disease, as is SofZia-preserved travoprost.
Another limitation of this study is that the observation period was not long and the observers were not blinded. However, a 12-week evaluation period is considered adequate to washout the previous eye drops and assess the therapeutic effects on the IOP and the condition of the ocular surface. 34 Aihara et al. 15 and Yamazaki et al. 14 found a beneficial effect of SofZia-preserved travoprost on the ocular surface conditions compared with 0.02% BAK-preserved latanoprost. Their study period was 3 months long (12 weeks). This is the reason why we set 3 months as our observation period. We based the present duration of observation on these previous studies. However, we cannot conclusively confirm whether a 3-month study period is sufficient to evaluate the ocular surface changes after applying eye drops. A longer observation period might provide clearer results.
We also included some subjects under the concomitant use of beta-blocker and prostaglandin analogs and prior bimatoprost users. Bimatoprost may thus have influenced the observed higher hyperemia score and lower IOP value. The characteristics of beta-blocker eye drops are not the same. Some beta-blockers are instilled once daily, while others are given twice daily. Some beta-blockers are considered to be much safer than others. This is the reason why we also analyzed the data after deleting the subjects receiving combined therapy with a prostaglandin analog and beta-blocker eye drops and prior bimatoprost users. Although the difference in the total SPK score and conjunctival hyperemia score showed marginal P-values (P=0.058 and P=0.053), the difference in the level of the total SPK score, tear BUT, hyperemia score, and IOP demonstrated no significant difference between the tafluprost and travoprost treatment phases. This may indicate that the difference in the ocular surface conditions between optimized BAK-preserved tafluprost and SofZia-preserved travoprost is not large.
We used the standard grading photographs to evaluate the conjunctival hyperemia. These are somewhat subjective methods. Yoneda et al. developed the software and system to evaluate the conjunctival hyperemia objectively. 35 Using objective methods to evaluate ocular surface condition may be necessary in the future.
In conclusion, we found no significant differences in the IOP-lowering effects of either tafluprost with 0.001% BAK or travoprost with SofZia. The ocular surface parameters (SPK, tear BUT, and conjunctival hyperemia) while using tafluprost preserved with 0.001% BAK were not inferior to those by SofZia-preserved travoprost.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Appendix: Members of the Ocular Surface Disease and Glaucoma Study Group
Yoshiaki Kiuchi, Takashi Kanamoto, Hideki Mochizuki, Shunsuke Nakakura, Ishida Yasuhito, Teranishi Shinichiro, Ken Sagara, Kuniisa Shinkawa, Miho Enoki, Masako Nakayama, Makiko Yuta, Miho Fukumura, Takashi Murashige, Masaki Tanito, Shiro Mizoue, Shinichi Okuma, Koji Namiguchi, Naoki Komatsu, Makiko Takahashi, Tomoko Naito, Rieko Ishihara, Tetsuya Baba, Kazuyuki Hirooka, Masanobu Mizote, and Ulfah Rimayanti