
Abstract
Abstract
Purpose:
To compare the changes in subfoveal choroidal thickness (CT) in eyes with neovascular age-related macular degeneration (nAMD) treated with intravitreal ranibizumab or aflibercept.
Methods:
In this retrospective case series, the medical records of 28 patients with nAMD treated with at least 3 consecutive monthly injections of ranibizumab (0.5 mg/0.05 mL) or aflibercept (2 mg/0.05 mL) between December 2013 and June 2014 and who were followed up for at least 3 months were reviewed. Subfoveal choroidal thickness was measured using enhanced depth imaging optical coherence tomography.
Results:
Choroidal thickness decreased over time in the aflibercept group, but was unchanged throughout the study in the ranibizumab group. At each time point, the decrease was significantly greater in aflibercept-treated eyes compared with ranibizumab-treated eyes (P<0.05). No significant change in best-corrected visual acuity (BCVA) was seen in either group during follow-up. There was no correlation between change in choroidal thickness and age, sex, duration of previous antivascular endothelial growth factor treatment, number of previous injections, spherical equivalent, baseline choroidal thickness, and the BCVA outcome in either group.
Conclusions:
Subfoveal choroidal thickness appeared to decrease significantly in eyes with nAMD during 3 months of aflibercept treatment. No corresponding decrease in choroidal thickness occurred in ranibizumab-treated eyes.
Introduction
C
Indeed, VEGF-A appears to play a key role in the physiological processes of the choroid and choroid vasculature, including regulation of the survival and permeability of the choriocapillaris (CC), which is known to be important in the development of age-related macular degeneration (AMD). 7 Consequently, prolonged inhibition of VEGF using intravitreal anti-VEGF agents may affect the integrity of the CC. This has been demonstrated, at least in principle, in primate models where intravitreal administration of bevacizumab 1.25 mg caused a number of ultrastructural changes, including a significant reduction in CC fenestrations, the formation of immunocomplexes, RPE cell death, and thrombotic microangiopathy.8–10 However, in a recent study comparing the effects of intravitreal ranibizumab 0.5 mg and aflibercept 2 mg in primate eyes, although hemolysis, formation of protein complexes, thrombotic microangiopathy, and reduction of CC density were seen with both drugs, these ultrastructural changes were more prominent in aflibercept-treated animals. Furthermore, in contrast to ranibizumab, which peremeated the retina through the intercellular spaces, aflibercept was taken up by RPE cells leading to RPE cell death and hypertrophy. 11 The higher binding affinity of aflibercept for VEGF-A isoforms may, at least in part, explain the apparent differences in the effects on CC integrity between the 2 drugs. In addition, through the Fc domain, aflibercept can bind to the Fc receptor of both CC endothelial cells and red blood cells, leading to complement mediated cell death. 11
We recently showed significant reduction of choroidal thickness (CT) in a cohort of patients with treatment-resistant exudative AMD who were converted to aflibercept injections. 12 Similarly, a significant choroidal thickness reduction in 23 eyes with typical nAMD treated with 3 loading doses of ranibizumab followed by administration as required has been reported. 13 However, following an initial decrease in mean choroidal thickness in the first 3 months of ranibizumab treatment, there was no further significant change over a 12-month period. 13 In another study with a mean follow-up of 23.8 months, although there was a decrease of choroidal thickness over time, ranibizumab did not appear to modify the decline, as the change did not differ between patients who did or did not receive ranibizumab. 14 Furthermore, other studies have not shown any significant change in choroidal thickness with ranibizumab.15,16
Therefore, to further investigate the effect of anti-VEGF therapy on the choroid, the present retrospective case series aimed to compare changes in subfoveal choroidal thickness in eyes with nAMD treated with 3 monthly injections of ranibizumab or aflibercept.
Methods
Study population
We performed a retrospective observational study conducted in the Eye Clinic of the Umberto I University Hospital, Rome, Italy. The local ethics committee approved the retrospective protocol, and the research followed the principles of the Declaration of Helsinki.
The medical records of patients with refractory nAMD (ie, persistent intraretinal or subretinal fluid with or without pigment epithelial detachment (PED) after at least 6 consecutive monthly injections with ranibizumab) who were treated with 3 further consecutive injections of ranibizumab (0.5 mg/0.05 mL) or converted to 3 monthly injections of aflibercept (2 mg/0.05 mL) between December 2013 and June 2014 were reviewed. Of note, aflibercept was available in our hospital only after February 2014. Thus, during the study interval, patients who were being converted and were in the loading phase were receiving monthly instead of bimonthly injections. All subjects provided written informed consent to ranibizumab or aflibercept injection in accordance with Italian laws regarding privacy. The time frame between the last ranibizumab injection before the study analysis must not be less than 4 weeks and could not exceed 6 weeks. Eligible eyes had to be followed up for at least 3 months on a monthly basis.
Patients in the ranibizumab and aflibercept group were then matched for age and mean number of previous anti-VEGF injections. Exclusion criteria consisted of the following: prior treatment with PDT; clinical signs of geographic atrophy on fundus examination or near infrared images; pathologic myopia, defined as a spherical equivalent of more than −6.0 D and/or consistent retinal abnormalities on fundus examination (such as myopic crescent, thinning and loss of the choriocapillary, prominent large choroidal vessels, areas of focal atrophy, and lacquer cracks); a diagnosis of retinal angiomatous proliferation or idiopathic polypoidal choroidal vasculopathy, glaucoma, macular hole, macular pucker, retinal vascular occlusion, choroiditis, hereditary diseases in the study or the fellow eye, or other ocular disease different from nAMD; and prior intraocular surgery except for uncomplicated phacoemulsification performed within the preceding 6 months.
Fourteen eyes of 14 patients were included in each group. The medical charts of the 28 patients were retrospectively reviewed and the following data were collected: patient age, gender, diagnosis, past ocular history, including dates, types, and number of previous intravitreal injections, and coexisting ocular conditions. All patients had to have had complete ophthalmic examination, including best-corrected visual acuity (BCVA) measurement and optical coherence tomography (OCT). BCVA was measured using the standardized, 70-letter Early Treatment Diabetic Retinopathy Study (ETDRS) chart (Chart “R”; Precision Vision) at a 4 m distance. In both the aflibercept and ranibizumab groups, subfoveal choroidal thickness and BCVA were recorded before the initiation of the last 3 consecutive injections (baseline) and at 1, 2, and 3 months thereafter.
Subfoveal choroidal thickness measurement
Spectral-domain OCT images of the choroid were obtained using the Spectralis OCT (Spectralis Family Acquisition Module, V 5.1.6.0; Heidelberg Engineering) and the enhanced depth imaging modality, following a standardized protocol. Active eye tracking (TruTrack) and automatic follow-up scan (AutoRescan) were used to enable point-to-point correspondence between consecutive follow-up scans. Keratometry readings (average corneal curvature in mm) and refraction (spherical equivalent in diopters) were entered into the Eye Data window of the Heidelberg Explorer Software to estimate optical magnification. All scans were acquired in the high-resolution acquisition mode. Two high-quality (>20 units) 30° horizontal and vertical line scans through the fovea comprising 90–100 averaged frames for each scan were obtained for each eye. The image showing best visualization of the border between the choroid and sclera was selected, and choroidal thickness was measured using a digital caliper tool. The choroid was defined as the layer between the base of the RPE and the hyperreflective line or margin corresponding to the chorioscleral interface (Fig. 1). In eyes with PED, choroidal thickness was defined as the layer between Bruch's membrane and the chorioscleral interface. Subfoveal choroidal thickness from the horizontal and vertical line scans was measured by 2 of the coauthors who were masked to the subjects' treatment, and the 4 values were averaged for data analysis.
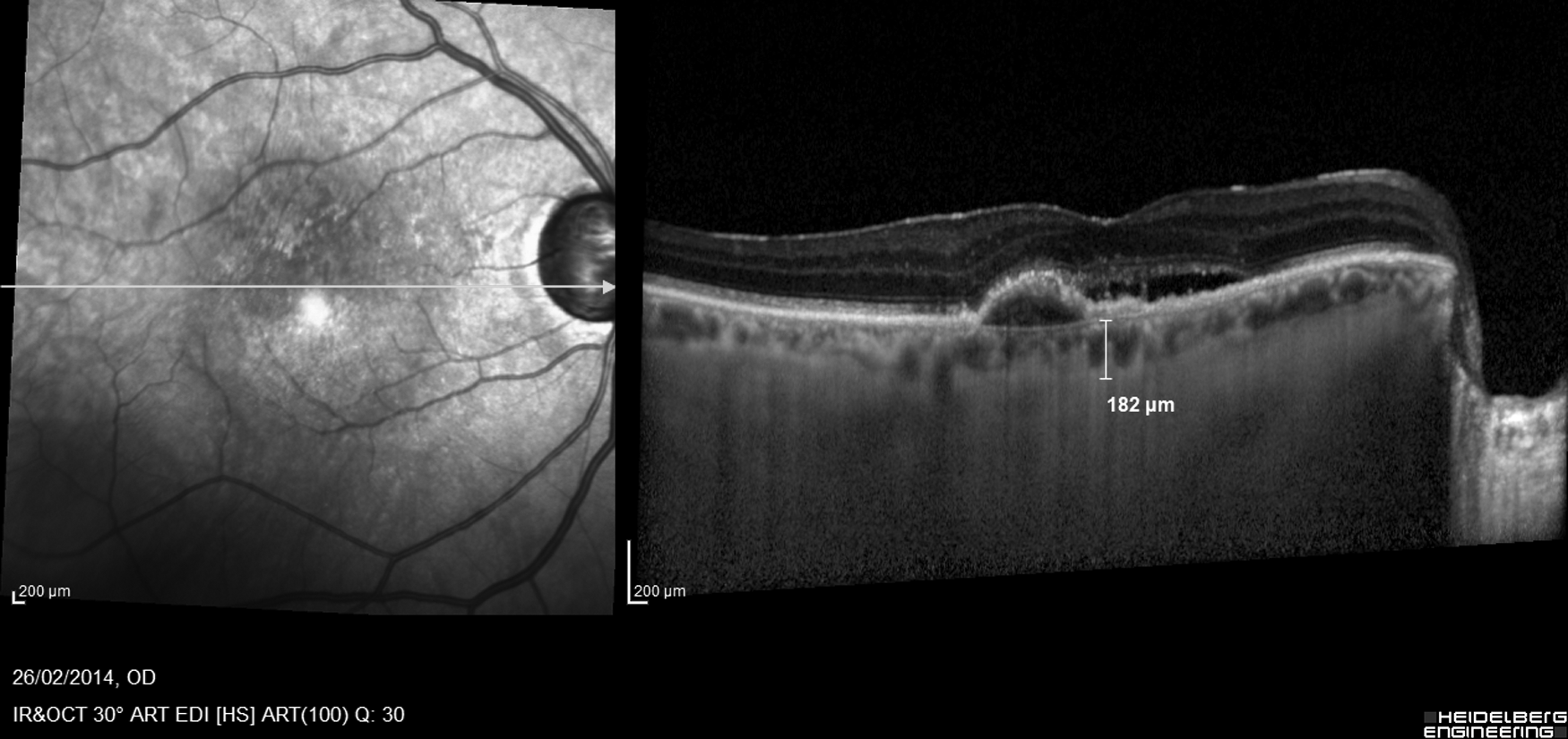
Representative optical coherence tomography image of subfoveal choroidal thickness measurement. The choroid was defined as the layer between the base of the retinal pigment epithelium and the hyperreflective line or margin corresponding to the chorioscleral interface. In eyes with pigment epithelial detachment, choroidal thickness was defined as the layer between Bruch's membrane and the chorioscleral interface.
Outcome measures
The primary outcome measure was change in the subfoveal choroidal thickness in eyes with nAMD in patients treated with ranibizumab or aflibercept. Correlations between choroidal thickness change and age, sex, baseline BCVA, number of previous injections, and BCVA outcome were also evaluated as secondary outcome measures.
Statistical analysis
All variables were tested for normal distribution using the Kolmogorov–Smirnov test. Longitudinal data were compared using the paired t-test or the Wilcoxon test, as appropriate. Intergroup differences were evaluated as choroidal thickness change compared with baseline using the unpaired t-test or the Mann–Whitney rank sum test, as appropriate. Categorical variables were compared using the Fisher's exact test. Bivariate correlations were examined using the Pearson analysis or the Spearman coefficient, as appropriate. Data are reported as mean value±standard deviation. P values <0.05 were considered significant.
Results
Twenty-eight eyes of 28 patients (14 in each group) who underwent 3 consecutive injections of aflibercept or ranibizumab for the treatment of nAMD were included in the study. All patients were previously treated with ranibizumab only. Fifteen patients were men and 13 women (4 men and 10 women in the aflibercept group and 11 men and 3 women in the ranibizumab group; P=0.02). The mean age was 75.6 years (range 63–86). Demographic and clinical characteristics of patients at the start of the study are shown in Table 1. There were no statistically significant differences in baseline values between groups. Furthermore, there was no significant difference in baseline choroidal thickness between men and women (223.0±96.0 and 181.7±62.7 for men and women, respectively; P>0.05, by both the unpaired t-test and Mann–Whitney rank sum test).
Values are mean±SD unless otherwise indicated.
Unpaired t-test with Levene's test for equality of variance.
Fisher's exact test.
BCVA, best-corrected visual acuity; ETDRS, Early Treatment Diabetic Retinopathy Study; VEGF, vascular endothelial growth factor; SD, standard deviation.
At baseline, mean choroidal thickness in the ranibizumab group was 212.6 μm compared with 195.1 μm in the aflibercept group (Table 1), with no significant difference between the groups. Choroidal thickness decreased over time in the aflibercept group, but remained virtually unchanged throughout the study in the ranibizumab group (Fig. 2). In the ranibizumab group, changes in choroidal thickness from baseline were −2.1±13.9, −3±19.1, and −2.9±19.0, at 1, 2, and 3 months, respectively. In the aflibercept group, changes in choroidal thickness from baseline were −14.0±12.2, −12.6±13.7, and −16.2±15.7, at 1, 2, and 3 months, respectively. At each time point, the decrease in choroidal thickness was significantly more prominent in aflibercept-treated eyes compared to ranibizumab-treated eyes (P=0.03, P=0.04, and P=0.03, at 1, 2, and 3 months, respectively). Changes in choroidal thickness over time are shown in Table 2. Changes in choroidal thickness in male patients were −6.1±14.1, −7.1±19.2, and −6.7±19.7, at 1, 2, and 3 months, respectively. The corresponding changes in female patients were −10.4±14.5, −8.5±14.7, and −12.8±17.0, at 1, 2, and 3 months, respectively. No significant differences in choroidal thickness were observed regarding sex (P>0.05, Mann–Whitney rank sum test).
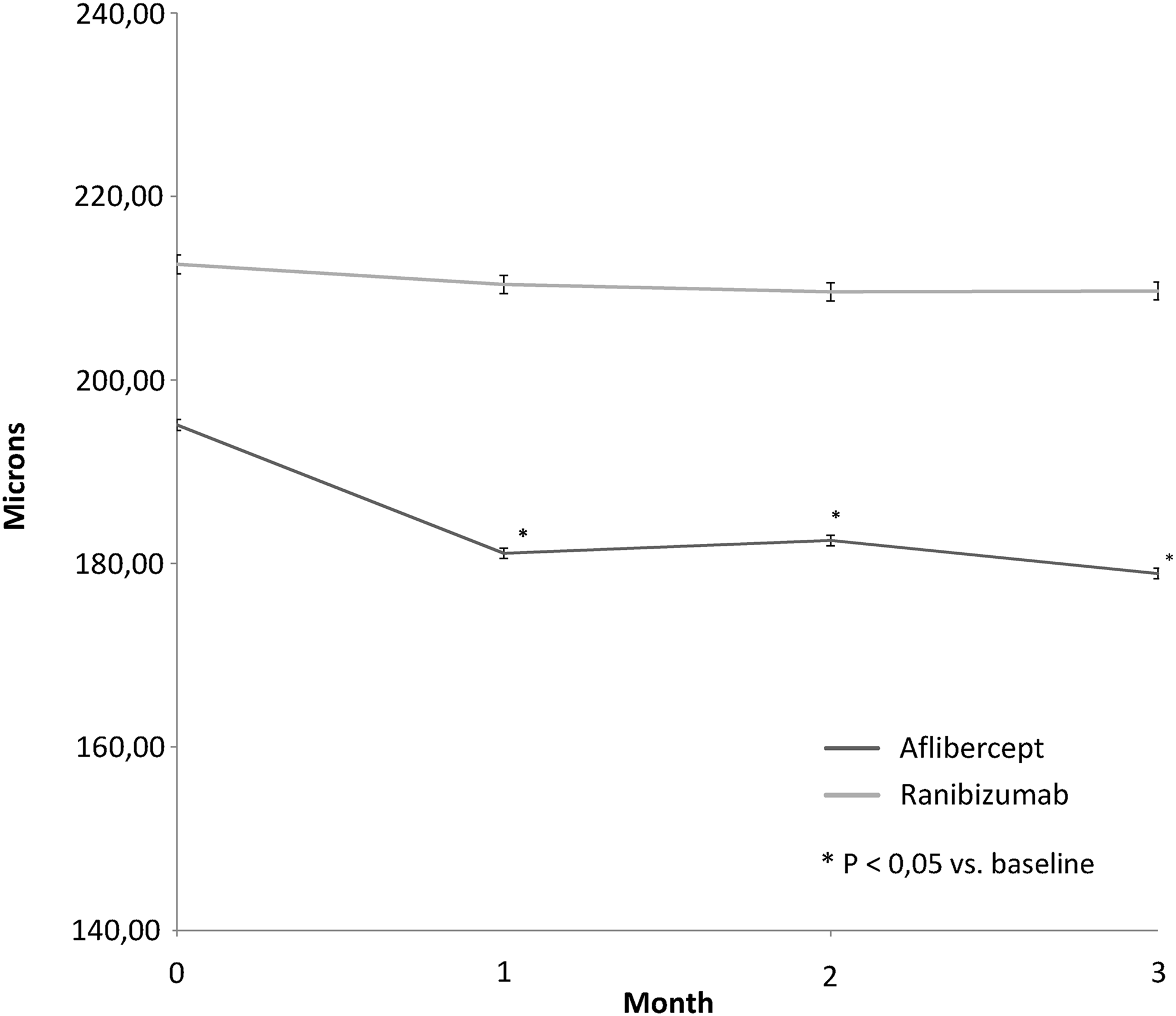
Mean subfoveal choroidal thickness during aflibercept and ranibizumab treatment for exudative age-related macular degeneration.
Values are mean±SD unless otherwise indicated.
Mann–Whitney rank sum test.
Paired t-test compared to baseline.
Mean baseline BCVA was 47.0±9.3 ETDRS letters (range, 27–57 letters) in the ranibizumab group and 43.7±11.0 letters (range, 22–59 letters) in the aflibercept group (P>0.05) (Table 1). At 3 months, mean BCVA in the ranibizumab group was 45.0±11.1 ETDRS letters and 43.6±9.4 letters in the aflibercept group. Compared with baseline, no significant change in BCVA was observed in either group (P>0.05, paired t-test). In addition, there was no difference in BCVA outcomes between groups (P>0.05, unpaired t-test).
Correlation analysis in either the ranibizumab or aflibercept groups did not find any relationship between changes in choroidal thickness and any of the following parameters: age, sex, duration of previous anti-VEGF treatment, number of previous injections, spherical equivalent, baseline choroidal thickness, and baseline BCVA (P>0.05, Spearman coefficient). Furthermore, no significant correlation was found between BCVA outcomes and changes in choroidal thickness during the study period (P>0.05, Pearson analysis). None of the eyes developed adverse events during the study.
Discussion
In the current, comparative retrospective case series, we evaluated the changes in choroidal thickness in patients with nAMD who were treated with 3 consecutive injections of ranibizumab or aflibercept. Compared with the ranibizumab group, aflibercept-treated eyes showed a significant decrease in choroidal thickness relative to baseline at each time point of follow-up.
The subfoveal choroid in the normal eye naturally thins with aging, with an estimated 1.56 μm decrease in thickness for each year of age. 17 Herein, at 3 months, aflibercept-treated eyes showed a mean decrease in choroidal thickness of 16.2 μm, which is greater than what could be expected during the natural course of aging.
VEGF inhibition has been shown to cause atrophic changes in the normal CC.8–10,18 Differences between aflibercept and ranibizumab in the biologic activity and binding affinities may account for the apparent thinning effect on the choroid shown by aflibercept in our study. Aflibercept is a soluble decoy receptor consisting of components of both VEGF receptor 1 (VEGFR1) and 2 (VEGFR2) fused to the Fc domain of human IgG-1, whereas ranibizumab does not have the Fc domain.11,19,20 Specifically, ranibizumab acts by blocking the receptor-binding domain of all VEGF-A isoforms, whereas aflibercept also binds to all VEGF-B isoforms and the placental growth factor. Compared with ranibizumab, aflibercept has a stronger binding affinity for VEGF-A and a longer presumed intravitreal half-life, which contributes to differences in the neutralizing ability against VEGF and duration of action.21,22 Furthermore, through the Fc domain, aflibercept can bind to the Fc receptor of CC endothelial cells and red blood cells, thus leading to complement mediated cell damage. 11
Indeed, experimental studies comparing the effects of intravitreal ranibizumab and aflibercept on the CC in primate eyes showed that reductions in CC density and CC endothelial wall thinning, as well as thrombotic microangiopathy, were more prominent in aflibercept-treated animals than in ranibizumab-treated animals. 11 Therefore, consistent with these experimental findings, the apparent thinning of the choroid that we observed in aflibercept-treated eyes may be interpreted as an undesired effect associated with choroidal vascular impairment and/or atrophic changes that may affect the integrity of RPE and the outer retina. Alternatively, the decrease in choroidal thickness may be reflective of a positive treatment response related to reduction in choroidal capillary permeability associated with the presence of an active choroidal neovascularization. However, our data do not allow us to draw any conclusions in this regard. Indeed, we only assessed the functional response, while we did not evaluate the relationship between choroidal thickness changes and the anatomical response to treatment (ie, intraretinal or subretinal fluid reduction and/or PED height reduction).
We did not find any correlation between baseline choroidal thickness and BCVA outcomes at 3 months. However, our follow-up is too short to draw definitive results. In addition, our cohort was characterized by non-naive patients with chronic nAMD. In a recent report, Kang et al. found that baseline subfoveal choroidal thickness was a significant prognostic factor for visual outcome in treatment-naive exudative AMD patients during a 6-month follow-up period. 23 Although the exact relationship between choroidal thickness and choroidal circulation is yet to be clarified, choroidal thickness is commonly used as a marker of choroidal circulation and CC status. Given its role in maintaining the RPE and outer retina, the choroid is considered to be important for visual acuity, and the findings by Kang et al. seem to support this concept.
To our knowledge, this is the first study comparing the effect of ranibizumab and aflibercept on choroidal thickness. However, its retrospective design, small sample size, and nontreatment-naive patients are potential limitations. With regard to the apparent, although nonsignificant, differences in baseline mean choroidal thickness, correlation analysis of baseline parameters demonstrated that changes in choroidal thickness over time were not related to the baseline choroidal thickness in either the ranibizumab or aflibercept groups.
In conclusion, our study showed that subfoveal choroidal thickness appeared to decrease during 3 months of aflibercept treatment in eyes with nAMD. However, given the limitations of this study, further investigations in appropriate prospective comparative studies of larger naive patient populations are needed to confirm whether clinically meaningful differences exist between ranibizumab and aflibercept with respect to thinning of the choroid and to investigate the relationship between choroidal thickness changes and treatment response.
Footnotes
Acknowledgment
Financial support for medical editorial assistance was provided by Novartis Farma, Italy.
Author Disclosure Statement
No competing financial interests exist.