
Abstract
Abstract
Purpose:
To compare the efficacy and safety of the brand-name and generic 2% dorzolamide/0.5% timolol fixed-combination (DTFC) drugs in glaucoma patients.
Methods:
This was a prospective single-center study, in which patients using only the brand-name DTFC (Cosopt®; Merck and Co, Inc.) drug and those using Cosopt with prostaglandin analogs (PGs) were enrolled. In the patients using Cosopt (Group A) and Cosopt with PGs (Group B), Cosopt was switched to its generic counterpart (Batidor®; Bausch & Lomb, Inc.). The intraocular pressure (IOP) was measured before the switch and 4, 8, and 12 weeks after the switch in both groups. The questionnaire on the discomfort symptoms and on the discomfort score for the use of eye drops was answered by the patients in both groups before the switch and 12 weeks after the switch.
Results:
A total of 112 patients were enrolled in the study, 62 in Group A and 50 in Group B. The IOPs before the switch and 4, 8, and 12 weeks after the switch showed no statistical difference in both groups (P>0.05). There were higher incidences of bitter taste and blurring with Cosopt, and there was a higher incidence of headache with Batidor in both groups, but no significant differences (P>0.05) were noted. There was, likewise, no significant difference in the discomfort score between 2 drugs in both groups (P>0.05).
Conclusions:
After the switch, the IOP-lowering effect of the generic drug Batidor was similar to that of the brand-name drug Cosopt in the monotherapy and combination therapy with PGs. No significant differences were found in terms of the discomfort symptoms and discomfort score between the 2 drugs.
Introduction
T
Generic drugs have been used in a variety of ways, such as cardiovascular medicines, anticonvulsant medicines, nonsteroidal anti-inflammatory drugs, levothyroxine, oral contraceptives, and proton pump inhibitors.4–8 This trend is also true for the antiglaucoma ophthalmic solutions.9–11 The 2% dorzolamide/0.5% timolol fixed-combination (DTFC) drug has been widely used for the treatment of glaucoma because of its highly intraocular pressure (IOP)-lowering effect and the increased compliance with it due to its ease of use.12,13 Lately, generic versions of DTFC have also become available in South Korea. Unfortunately, however, there has been no clinical study comparing generic and brand-name DTFC drugs. In this study, the efficacy and safety of the generic and brand-name DTFC drugs in glaucoma patients were compared.
Methods
This study was performed as a prospective single-center trial approved by the institutional review board at Cheil Eye Hospital. The study was conducted in accordance with the ethical principles described in the Declaration of Helsinki. Before their enrollment in the study, the subjects received information regarding the study and written informed consent was obtained from each subject.
The subjects were South Korean glaucoma patients who had been receiving treatment with a DTFC brand-name drug (Cosopt®; Merck and Co, Inc.) with or without prostaglandin analogs (PGs) for at least 3 months. Patients with a history of a laser treatment or ocular surgery within 6 months, previous glaucoma surgery, conditions preventing IOP measurement by applanation tonometry, and discomfort increased by another ocular disease, except an ocular surface disease, were excluded from the study. The subjects were divided into 2 groups. Group A consisted of patients who had used only Cosopt, and Group B consisted of those who had used Cosopt and PGs.
The study consisted of 4 scheduled visits over 12 weeks (day 0 and weeks 4, 8, and 12). At day 0 (preswitch), Cosopt was switched to a generic drug (Batidor®; Bausch & Lomb, Inc., Tampa, FL) in both groups. The administration time of Batidor was set to around the same time before the administration of Cosopt. The IOP value used for analysis was the mean of 2 Goldmann applanation tonometry readings, while the measurement time for each patient was decided based on the time of the baseline measurement. As such, the measurements were performed within 2 h, either before or after such time. For the evaluation of the adverse events, a questionnaire survey (Fig. 1) about the discomfort symptoms and the overall discomfort score was conducted at day 0 and week 12 after the switch in both groups.
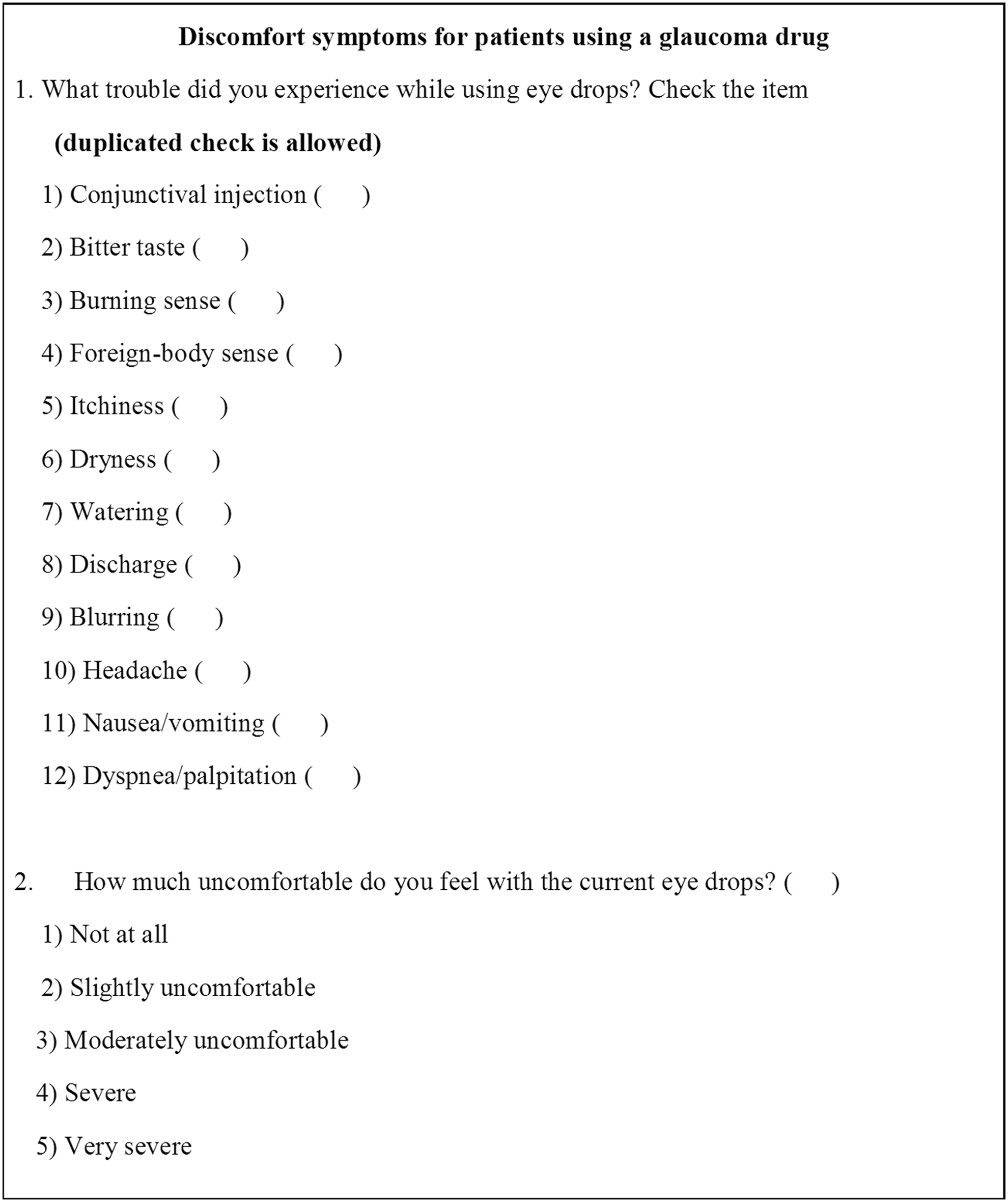
Questionnaire on discomfort.
Statistical analyses were performed using PASW Statistics 18.0 version (SPSS, Inc., Chicago, IL). The IOPs and the IOP reduction rates of each group were determined using repeated measures analysis of variance compared to the mean and standard deviation. Each discomfort symptom was evaluated using a nonparametric McNemar test. The discomfort scores of the 2 drugs in each group were compared using the paired t-test. P<0.05 was considered statistically significant.
Results
A total of 112 patients were enrolled in this study. Sixty-two patients were recruited in Group A and 50 in Group B. Group A composed of 27 men (43.5%) with a mean age of 63.2±13.3 years, and Group B composed of 28 men (56%) with a mean age of 63.1±12.5 years. In Group A, 71.9% (n=77) had primary open-angle glaucoma and 10.3% (n=11) had angle-closure glaucoma. In Group B, on the other hand, 80.5% (n=74) had open-angle glaucoma and 9.8% (n=9) had angle-closure glaucoma (Table 1). Forty-two percent of patients (n=21) were given tafluprost 0.005% (Taflotan®; Santen Pharmaceutical Co., Ltd., Osaka, Japan), 36% (n=18) were given latanoprost 0.005% (Xalatan®; Pfizer, Inc., Puurs, Belgium), 18% (n=9) were given travoprost 0.004% (Travatan®; Alcon Laboratories, Inc., Fort Worth, TX), and 4% (n=2) were given bimatoprost 0.01% (Lumigan®; Allergan, Inc., Irvine, CA) in Group B, and these were continued during the study period.
Chi-square test.
Linear by linear association.
POAG, primary open-angle glaucoma; ACG, angle-closure glaucoma.
The IOPs in Group A were as follows: 13.9±4.0 mmHg at preswitch and 13.1±3.9, 14.1±4.2, and 13.4±3.5 mmHg at weeks 4, 8, and 12 postswitch, respectively. There was no statistically significant difference in IOPs in Group A (P=0.44). The IOPs in Group B were as follows: 12.4±2.0 mmHg at preswitch and 12.0±3.0, 12.0±2.8, and 12.0±3.1 mmHg at weeks 4, 8, and 12 postswitch, respectively. There was also no statistically significant difference in IOPs in Group B (P=0.50, Fig. 2). The rates of IOP reduction are shown in Fig. 3. In Group A, the IOP reduction rates were −38.2%±21.4% at preswitch and −41.9%±18.6%, −37.2%±26.1%, and −38.2%±26.0% at weeks 4, 8, and 12 postswitch, respectively, with no significant difference (P=0.26). In Group B, the IOP reduction rates were −38.6%±20.3% at preswitch and −41.7±17.9, −39.2±29.6, and −40.7%±24.0% at weeks 4, 8, and 12 postswitch, respectively. There was also no statistically significant difference (P=0.52).
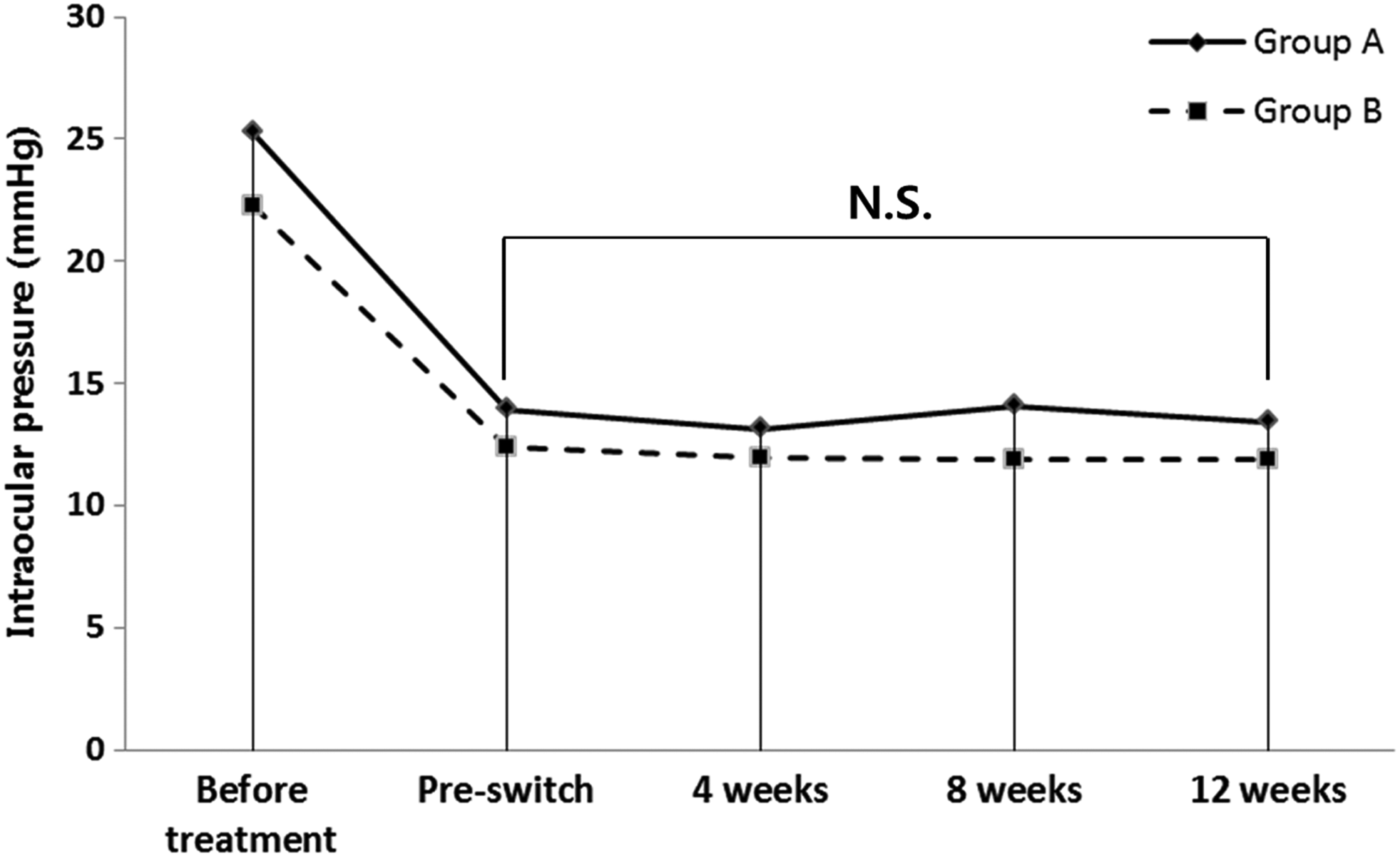
Mean intraocular pressure (IOP) after the switch to Batidor® in the 2 groups. There was no significant difference between preswitch and at weeks 4, 8, and 12 postswitch in each group (P>0.05, repeated measures analysis of variance [ANOVA]).

IOP reduction rate from before treatment to preswitch (Cosopt®) and at weeks 4, 8, and 12 postswitch (Batidor). There was no statistically significant difference in IOP reduction rate between Cosopt and Batidor in each group (P>0.05, repeated measures ANOVA). Data are expressed in mean±SD.
The adverse events were also evaluated through the questionnaire survey, which were conjunctival injection, bitter taste, burning sense, foreign body sense, itching, dryness, watering, discharge, blurring, headache, nausea/vomiting, and dyspnea/palpitation. Adverse events were reported for both drugs by 58.1% (n=36) of the patients in Group A, by 58.0% (n=29) of the patients in Group B for Cosopt with PGs, and by 54.0% (n=27) of the patients in Group B for Batidor with PGs. In Group A, bitter taste (7.7% vs. 3.2%, P=0.38) and blurring (3.2% vs. 0.0%, P=0.50) were numerically common in Cosopt, and dryness (0.0% vs. 3.2%, P=0.50), headache (0.0% vs. 8.0%, P=0.06), and nausea/vomiting (0.0% vs. 3.2%, P=0.50) were numerically common in Batidor. In Group B, bitter taste (12.0% vs. 6.0%, P=0.38), foreign body sense (12.0% vs. 4.0%, P=0.29), blurring (16.0% vs. 10.0%, P=0.45), and nausea/vomiting (6.0% vs. 0.0%, P=0.25) were numerically common in Cosopt, and conjunctival injection (16.0% vs. 26.0%, P=0.23) and headache (0.0% vs. 4.0%, P=0.50) were numerically common in Batidor. Nausea/vomiting (n=5) were transient symptoms after drug instillation and there were no vomiting symptoms. Headache (n=7) was also transient and was a mild symptom caused by a burning sensation after drug instillation. No cardiovascular and pulmonary adverse events were reported during the study (Table 2). The discomfort scores representing the overall uncomfortable sensation at preswitch and at week 12 postswitch were 1.8±0.8 and 1.6±1.0 in Group A, respectively, and 1.8±0.8 and 1.5±0.7 in Group B, showing no statistically significant difference between the 2 drugs in each group (P>0.05, Table 3).
One patient may have experienced more than 1 adverse event.
McNemar test.
The values are presented as mean±standard deviation.
Paired t-test.
Discussion
In this study, the IOP-lowering effects and safety of the brand-name drug Cosopt and of the generic drug Batidor were compared. The study results showed that Cosopt and Batidor had similar IOP-lowering effects, regardless of whether PGs were used or not used. The IOP reduction rate of both Cosopt and Batidor at week 12 postswitch was −38.2%. These findings are consistent with those of recent studies. Henderer et al. 14 showed a mean percentage change of −40% in the patients after 2 months of initial treatment with Cosopt. Crichton et al. 15 reported a −36.4% change in IOP after 6 weeks, and a −40.4% change in the patients treated with Cosopt after 12 weeks. Kim et al., 16 however, reported an IOP change of −23.7% at week 12 postswitch in the normal-tension glaucoma patients treated with DTFC, which was inferior to the results of the present study. This may be attributable to the lower baseline IOP compared to that of the subjects in the present study. In the results of the present study, the IOP-lowering effects of Cosopt and of Batidor with PGs were −38.6% and −40.7%, respectively, which were consistent with the results of the previous studies.17,18 The IOP-lowering effect of DTFC with PG, however, was similar to that of DTFC only in the present study. It is supposed that this result might have been due to the difference in the baseline IOP between the 2 groups.
The previous studies have shown that the efficacy of brand-name systemic drugs and of the generic systemic drugs is equal. In tacrolimus, the equivalent efficacy of the brand-name drug Prograf® (Astellas Ireland Co., Ltd.; Killorglin, County Kerry, Ireland) and of the corresponding generic drugs was reported. 7 Furthermore, the generic cyclosporine drug had a similar efficacy as the brand-name drug Sandimmune® (Norvatis Pharmaceuticals, Basel, Switzerland).19,20 Conversely, in antiglaucoma drugs, the study on Xalatan (Pfizer, New York, NY) showed that the IOP-lowering effect of Xalatan was higher compared with the corresponding generic drug in primary open-angle glaucoma and ocular hypertension patients. The difference in IOP lowering could be caused by the difference in adjuvants. 21
The safety of the 2 drugs was evaluated based on their discomfort symptoms and discomfort scores. There were no significant differences in terms of the discomfort symptoms and discomfort score in both groups. These results were similar to previous studies, which showed no differences in terms of adverse events between the generic drug and brand-name drugs of simvastatin, warfarin, and clozapine.22–26 Nevertheless, in the present study, there was a trend of higher incidences of bitter taste and blurring with Cosopt, and a higher incidence of headache with Batidor in both groups, but without significant differences. In fact, there are no differences in terms of active ingredient, preservative (0.0075% benzalkonium chloride), pH (∼5.65), and osmolarity (242–323 mOsM) between Cosopt and Batidor, based on data from the US Food and Drug Administration. Although generic drugs have the same qualitative and quantitative compositions in terms of active substances, adjuvants are not obvious.3,27 A difference in adjuvants could lead to differences in viscosity, surface tension, and pH, which could cause a different trend in the incidence of discomfort symptoms between generic and brand-name drugs.27,28 In addition, it is presumed that the different trend of incidences in discomfort symptoms could also be influenced by the drop volume, which was attributed to the different bottle designs. 29
This study had limitations. First, regression to the mean could affect the result of IOP measurements, since the IOP measurement was not blinded. Second, there was a limitation in comparing the safety of the 2 drugs because of the insufficient washout period. As the follow-up period, however, was 3 months, which is longer than the commonly considered washout period of brand-name drugs, it seemed difficult for the remaining effects of the previous medication to affect the aforementioned study results. Finally, the present study was likely to have a bias that brand-name drugs might be better than generic drugs. There were few patients, however, who had been familiar with brand-name and generic drugs (data were not shown). In addition, efforts were made to eliminate prejudice by explaining to the patients that the active ingredients of the brand-name and generic drugs were the same. Nevertheless, despite these limitations, the design of this study reflected the common clinical situation of switching from a brand-name drug to a generic drug.
This study is the first one to compare the brand-name DTFC drug Cosopt with the generic DTFC drug Batidor. After the switch, the IOP-lowering effect of Batidor was found to be similar to that of Cosopt at the monotherapy and combination therapy with PGs. In addition, there was no difference in the discomfort symptoms and discomfort score for the monotherapy and combination therapy with PGs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.