
Abstract
Abstract
Purpose:
To assess the efficacy and safety of switching from timolol 0.5% to brimonidine 0.1% in patients with glaucoma treated with a prostaglandin analog (PGA) and timolol combination.
Methods:
This prospective, open-label multicenter study enrolled patients with open-angle glaucoma or ocular hypertension who were being treated with a PGA and timolol. After baseline measurements, timolol was switched to brimonidine 0.1%, and patients were followed for 12 weeks. Patients visited at 4 and 12 weeks after switching. The main outcome measure was the change in intraocular pressure (IOP). For safety evaluations, hyperemia, formation of conjunctival follicles, superficial punctate keratopathy as a local side effect, blood pressure (BP), and heart rate (HR) were evaluated.
Results:
One hundred seven patients participated in this study. Among them, 103 patients completed the study. The IOP values at baseline, 4 weeks, and 12 weeks after the transition were 15.7±2.7, 14.3±2.8, and 14.0±2.8 mmHg, respectively. IOP was significantly reduced at 4 and 12 weeks compared with baseline (p<0.001). There were no significant changes in hyperemia or follicle formation. The superficial punctate keratopathy score was significantly reduced at 12 weeks compared with baseline (p<0.05). Systolic and diastolic BP values were significantly reduced and HR significantly increased after switching (p<0.05).
Conclusion:
Switching from timolol 0.5% to brimonidine 0.1% may not change IOP in the combination use of timolol 0.5% and a PGA and was well tolerated by patients without severe ocular or systemic side effects.
Introduction
V
Regarding the IOP-lowering effects of non-PGAs, the beta-blocker timolol elicits a strong reduction in IOP; however, there are some concerns regarding systemic side effects associated with the pulmonary and circulatory systems. Timolol often lowers the heart rate (HR) and blood pressure (BP) and may induce asthma and worsen chronic obstructive pulmonary diseases.1–3 In addition, timolol induces a local anesthetic effect on the ocular surface, leading to poor tear secretion. 4 Interestingly, tachyphylaxis has been reported during the long-term use of timolol. 3 In contrast, brimonidine lowers IOP without any pulmonary side effects. 5 However, systemic hypotension and allergic follicular conjunctivitis have been reported.6–9
Among the various regimens using these 2 types of glaucoma drugs, combination therapy with a PGA and timolol is popular because of the presence of fixed-combination drugs or the concomitant use of a PGA. Additionally, the once daily use of timolol may be favorable for decreasing the number of drops required. Treatment options with a topical CAI or brimonidine in addition to a PGA are also preferred over beta-blockers to reduce side effects. For appropriate decision making regarding the choice of second-line drugs for medical treatment in addition to a PGA, the additional IOP-lowering effects of the second-line drugs should be known. However, the additional IOP-lowering effects of timolol and brimonidine when used in combination with a PGA have not been fully investigated.10,11,12
In this prospective, open-label multicenter study with over 100 patients, we examined the efficacy and safety of switching from timolol to brimonidine in the combination use of a PGA and timolol in Japanese patients with open-angle glaucoma (OAG) or ocular hypertension (OH).
Methods
Patients
In this study, patients attending the Eye Rose Clinic, Unoki Eye Clinic, Omiya Hamada Eye Clinic, Koseki Eye Clinic, Matsuo Eye Clinic, Honda Eye Clinic, and Miyata Eye Hospital were enrolled from March 2013 to December 2013 and followed for 12 weeks. The study was approved by the local ethics committee at Miyata Eye Hospital and was conducted according to the tenets of the Declaration of Helsinki. Adult patients with OAG or OH treated with a PGA for at least 12 weeks and timolol 0.5% for at least 4 weeks were eligible for inclusion. Additional inclusion criteria were that IOP values at the entry and the switching were controlled at 12 mmHg or higher and the difference between both IOP values was less than 3 mmHg.
Exclusion criteria were as follows: (1) pseudoexfoliation glaucoma; (2) patients with any active ocular disease (eg, extraocular and intraocular inflammation, ocular infection, severe dry eye); (3) a history of intraocular surgery less than 12 weeks before entry; (4) a history of trabeculectomy, trabeculotomy, or laser in situ keratomileusis; (5) patients who changed or discontinued glaucoma medications within 4 weeks before baseline IOP; and (6) patients judged ineligible by an investigator. In instances where both eyes were eligible for the study, the eye with the higher IOP was selected for the evaluation of IOP reduction, but both eyes were investigated for the evaluation of safety.
Procedures
The main outcome measure was the change in IOP. Additional outcome measures were hyperemia, conjunctival follicular formation, superior punctate keratitis (SPK), BP, and HR. After the initial evaluation, informed consent was obtained from all patients. Eligible patients were instructed to continue the use of their current PGA, discontinue the use of timolol 0.5%, and start brimonidine 0.1% twice daily. Patients were required to attend 3 visits in the morning, including on the day of transition, and at 4 and 12 weeks after switching.
Intraocular pressure
IOP was measured in the morning with a Goldmann applanation tonometer. Two measurements were required; if the difference between the 2 values was greater than 3 mmHg, the IOP was measured once more, and the middle value was used for the analysis. Baseline IOP on PGA and timolol was the average of the IOP on the day the patient switched medications and on the last visit at least 2 weeks before entry.
Other ophthalmic examinations
At baseline, 4 weeks, and 12 weeks, the grade of conjunctival hyperemia, follicle formation, SPK score, HR, systolic BP, and diastolic BP were assessed. Conjunctival hyperemia was classified using a 4-grade photographic scale (slight, mild, moderate, and severe). SPK was assessed by fluorescein staining observed employing a blue-free filter and evaluated using National Eye Institute classifications. 13 Conjunctival follicle formation was observed under a microscope. HR and BP were measured with a conventional automatic tonometer. In detail, after a 5-min rest, HR and BP were measured twice; if the pressure difference was greater than 5 mmHg, they were measured once more and the closer of the 2 values was used for the analysis. Adverse events related to the medications were recorded on the transition day, at 4 weeks, and at 12 weeks. Compliance for the drop regimen was classified into 5 grades: (1) almost compliant with the regimen or forget once a week, (2) forget twice a week, (3) frequently forget, but drop more than 50%, (4) frequently forget and drop less than 50%, and (5) drop overdose. The patients reported the grading. If a patient forgot to use eye drops thrice during the week, the patient was excluded from the study.
Sample size and power analysis
A sample size was selected to provide sufficient statistical power (at least 80%) to detect outcome differences between before and after switching based on following premises: (1) decrease of 1.0 mmHg in IOP after switching; (2) standard deviation of 3.0 mmHg; and (3) significance level of 5% (2-tailed test).
All data were analyzed at a center independent of the clinics where the patients were enrolled. Changes in IOP, SPK, BP, and HR were compared using paired t-tests. Changes from baseline in hyperemia grade and follicular formation were compared using Wilcoxon signed-rank tests.
Results
Patients
One hundred seven patients were enrolled in this study. Among the 107 eligible eyes from 107 patients, 4 patients were excluded because 3 were lost to follow-up and 1 had poor eye drop compliance. One hundred three patients were eligible for the analysis, and 99 patients completed the 12-week protocol. The demographic data of the 103 patients are indicated in Table 1. Their average age was 66.4±12.4 years. Most patients had OAG (95.1%; 98/103), while OH patients accounted for 4.9% (5/103). Among the 103 patients, 41 were men and 62 were women. Two cases were excluded after 4 weeks because of adverse events, including itching of the eyelid and drowsiness, and 2 cases were lost to follow-up after 4 weeks.
OAG, open-angle glaucoma; OH, ocular hypertension; SD, standard deviation.
Intraocular pressure
The mean IOP at baseline was 15.7±2.7 mmHg. After switching to brimonidine, IOP values at 4 and 12 weeks were 14.3±2.8 and 14.0±2.8 mmHg, respectively (Fig. 1). The reduction rates at 4 and 12 weeks were 8.8% and 10.0%, respectively. These reductions in IOP at 4 and 12 weeks after switching to brimonidine were statistically significant compared with baseline IOP values (paired t-test, p<0.001). The distribution of the reduction rate with a 10% scale at 12 weeks is indicated in Fig. 2.
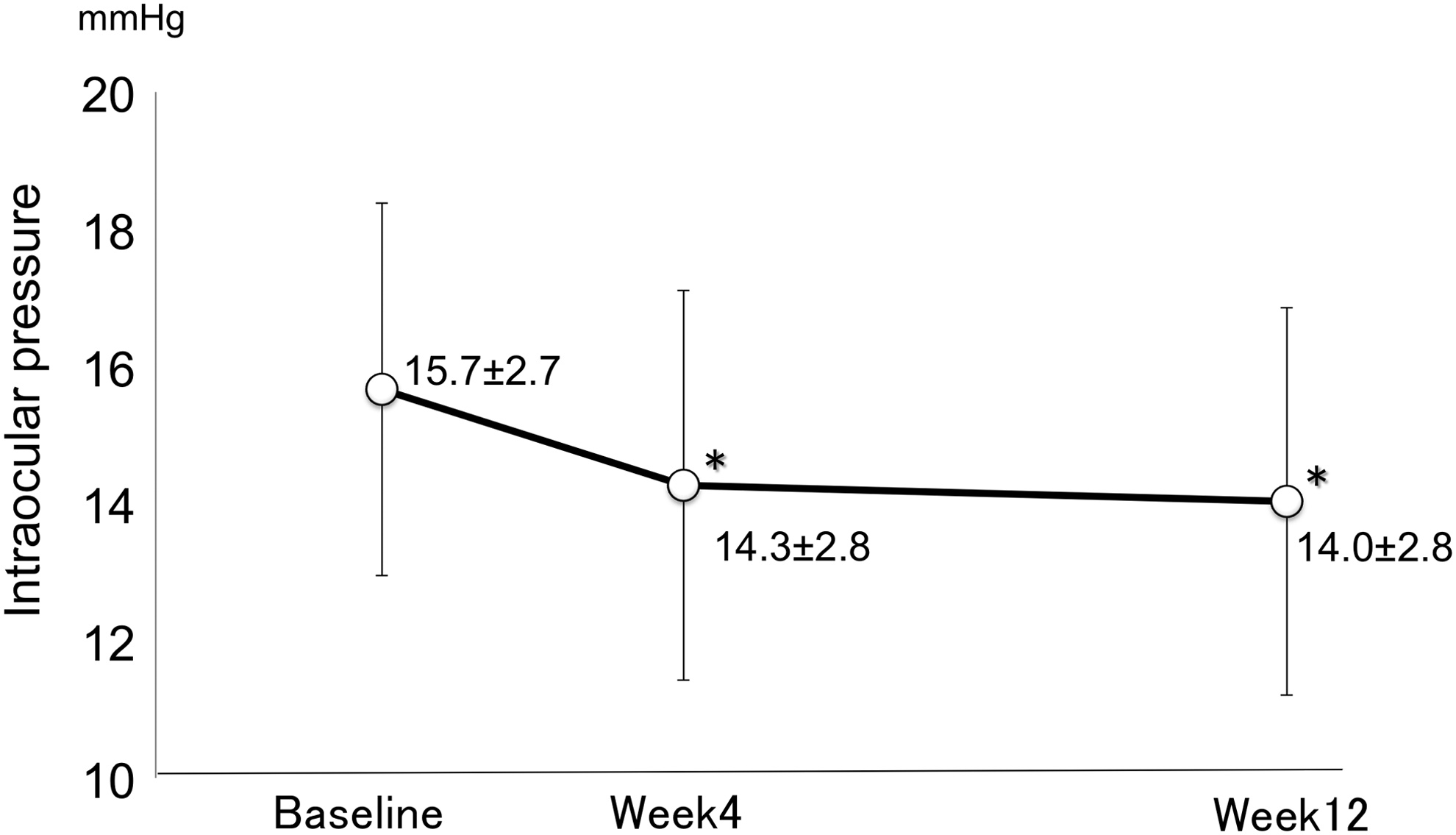
Intraocular pressure (IOP) measurements. IOP is presented as the mean±standard deviation. An asterisk indicates a significant change in IOP compared with the baseline value by a paired t-test (p<0.001). Baseline: before switching from timolol to brimonidine; 4 and 12 weeks: the time after switching.

The distribution of the IOP reduction rate at 12 weeks of treatment with brimonidine added to prostaglandin analogs (PGAs) in patients with ocular hypertension or glaucoma.
Conjunctival hyperemia, follicle formation, and superficial punctate keratitis
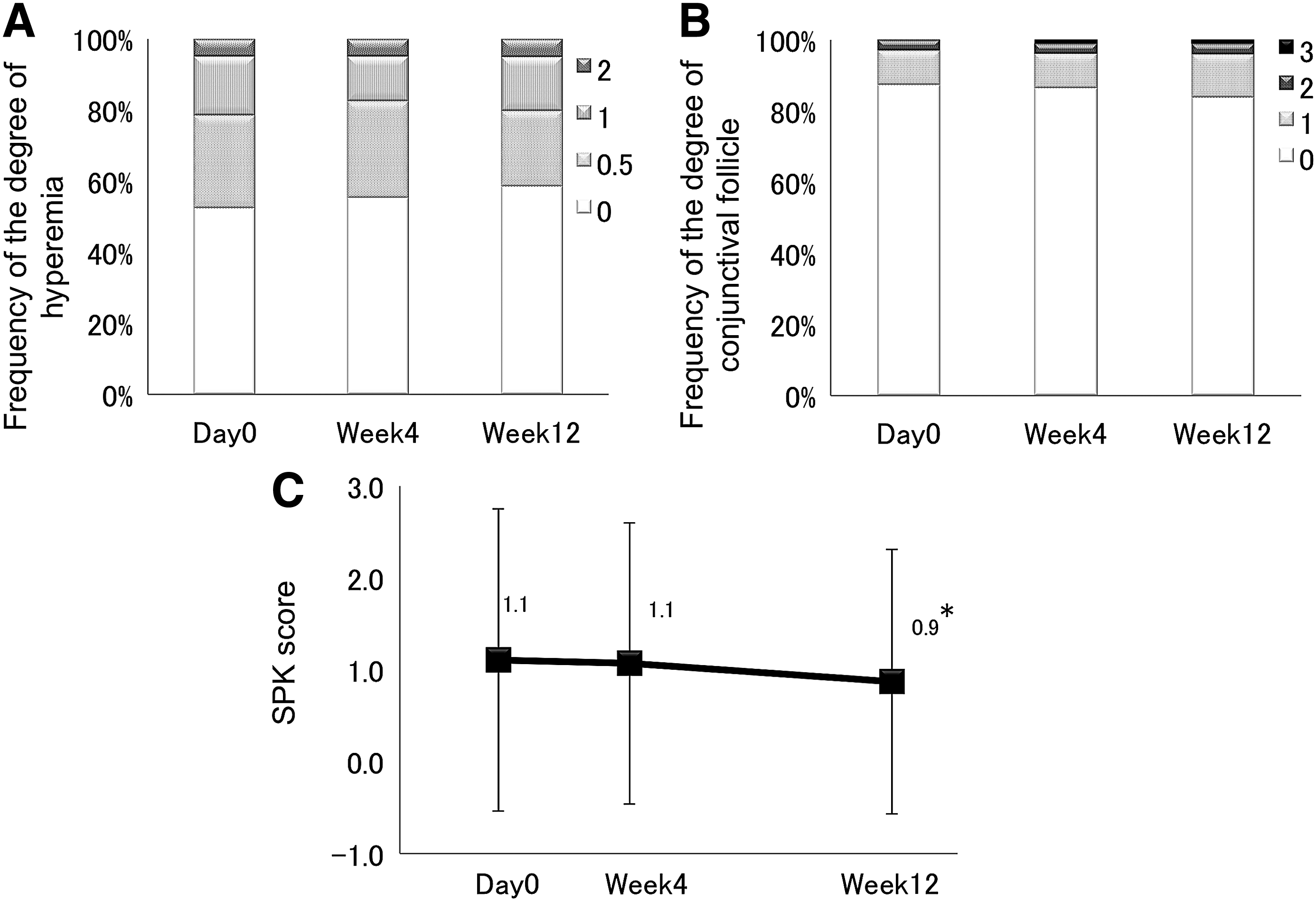
Neither conjunctival hyperemia nor follicle formation significantly changed during the 12-week period (Fig. 3A, B). Conjunctival follicles were newly observed in 5 cases. The SPK scores in 5 areas of the cornea at baseline, 4 weeks, and 12 weeks were 1.1±1.6, 1.1±1.5, and 0.9±1.4, respectively. At 12 weeks, the score was significantly reduced compared with that at baseline (p<0.05); however, this result was not clinically significant (Fig. 3C).
BP and HR
Systolic BP values at baseline, 4 weeks, and 12 weeks were 137.7±18.7, 130.0±18.8, and 128.2±19.8 mmHg, respectively. Diastolic BP values at baseline, 4 weeks, and 12 weeks were 80.1±14.0, 74.7±13.3, and 75.3±13.1 mmHg, respectively. Systolic and diastolic BP values at 4 and 12 weeks were significantly decreased compared with those at baseline (p<0.05, paired t-test; Fig. 4A). HR values at baseline, 4 weeks, and 12 weeks were 67.9±10.8, 75.5±12.8, and 74.0±11.4 beats per minute, respectively. HR values at 4 and 12 weeks were significantly increased compared with those at baseline (p<0.001, paired t-test; Fig. 4B).

Discussion
This multicenter prospective study investigated the effect of replacing timolol 0.5% with brimonidine 0.1% in OAG patients treated with a combination of a PGA and timolol 0.5%. Ninety-nine patients completed the study; only 4 of 103 patients discontinued the study during the 3-month follow-up period. Two cases of itching of the eyelid and drowsiness were completely cured during the follow-up period. There were no severe adverse events during the study.
The alpha-2 agonist brimonidine is known to reduce aqueous humor production and increase uveoscleral outflow. 5 Brimonidine effectively reduces IOP, as do beta-blockers and topical CAIs.8,14 Only 3 studies have reported that the additional IOP-lowering effect of brimonidine administered with a PGA is comparable with the IOP-lowering effects of timolol.10,11,12 Netland et al. compared the outcomes of brimonidine/bimatoprost and timolol/latanoprost groups in 28 patients with OAG or OH for 3 months. 11 Stewart et al. conducted a crossover study using a latanoprost/timolol fixed combination with concomitant use of brimonidine and latanoprost in 32 patients with OAG or OH for a 6-week period. 12 Reis et al. compared the additional effects of brimonidine, timolol, and brinzolamide in combination with travoprost in 52 patients with OAG or OH for a total of 4 weeks. 10 Although there are some differences in study design, there was no significant difference in IOP reduction or safety. However, the number of subjects in each group was small, the baseline IOP values were over 25 mmHg, and the observation period may have been too short to evaluate side effects. Thus, we conducted this 3-month study in Japanese patients with OAG who had low baseline IOP values of around 15 mmHg to evaluate the efficacy and safety of brimonidine after switching from timolol with concomitant use of a PGA.
In this study, brimonidine significantly lowered IOP compared with timolol and a PGA. However, care should be taken in interpreting these results since this study did not have a crossover design. In this one-way switching study, the investigators were not masked to the IOP measurement, and the patients were not masked to the treatment. After switching, regression to the mean may occur, and the adherence of patients to their drug regimens may improve. Thus, our results indicating a significant increase in the IOP-lowering effects of brimonidine may be underestimated. Alternatively, because timolol is known to induce tachyphylaxis with long-term use, 3 brimonidine may demonstrate an additional IOP reduction after switching from timolol. Therefore, considering these points and the previously reported IOP-lowering effects of brimonidine,8,14,15 we could conclude that brimonidine had IOP-lowering effects similar to those of timolol 0.5% in PGA-treated Japanese patients with OAG who had relatively low baseline IOP values of ∼15 mmHg. However, due to the limitations of our study design, a multicenter 2-arm comparative study should be conducted to further identify the risks and benefits of treatment with brimonidine versus beta-blockers.
We also examined the side effects of brimonidine when used as a treatment with a PGA. Brimonidine often induces allergic follicular conjunctivitis with long-term use. 14 However, in this 3-month study, there was no obvious allergic conjunctivitis, although an increase in follicles was newly observed in 5 cases. Therefore, care should be taken to evaluate patients for increases in allergic follicular conjunctivitis after long-term brimonidine use.
On the ocular surface, SPK was significantly reduced at 12 weeks. One of the reasons may be differences in the base ingredients. Timolol-containing drugs include benzalkonium chloride (BAK), and timolol/travoprost-containing drugs include polidronium chloride, whereas AIPHAGAN® ophthalmic solution brimonidine 0.1% contains sodium chlorite and boric acid as preservatives instead of BAK. Although BAK is a useful preservative from the standpoint of its strong antibacterial activity and solvency, its cytotoxicity to the ocular surface may not be negligible. 16 Moreover, since timolol has an anesthetic effect on the ocular surface, 17 the secretion of tears may be disturbed before switching. Thus, switching from timolol to brimonidine may improve ocular surface conditions.
Regarding systemic side effects, BP decreased and HR increased after switching from timolol. Beta-blockers often reduce BP by blocking sympathetic beta-receptors in the peripheral vascular system,1,2,15 whereas alpha agonists can reduce BP by stimulating alpha-2 receptors in the central nervous system in cases where it penetrates into the brain through the blood–brain barrier. 6 Although brimonidine significantly reduced BP in this study, there were no critical cases of hypotension. The increase in HR after switching to brimonidine 0.1% may be caused by the reduction in the beta-blocking effect, consistent with the findings of a previous study. 15
In conclusion, our study suggests that switching from timolol 0.5% to brimonidine 0.1% may not change the reduction in IOP and may restore changes in the HR resulting from the combined use of timolol 0.5% and a PGA. The combination of brimonidine 0.1% and a PGA was well tolerated by patients without severe ocular or systemic side effects.
Footnotes
Author Disclosure Statement
No competing financial interests exist.