
Abstract
Abstract
Purpose:
To establish the efficacy of topical N-acetylcysteine (NAC) as a treatment to reduce protein deposition on the contact lens surface.
Methods:
In this prospective, nonrandomized clinical trial, a total of 10 eyes (9 patients) were enrolled from a single center. All patients had a prior ocular history of either a Boston Keratoprosthesis type I or trichiasis from Stevens–Johnson syndrome, which necessitated full-time contact lens wear. Four visits were required to complete the study. During visit 1, a new contact lens was inserted and a baseline examination was performed. Visit 2 served as the control month, whereas visits 3 and 4 were month 1 and 2 on treatment with 20% NAC. At the end of each visit the contact lens was replaced. The lenses from visit 2 (control month—without NAC) and from visit 3 (treatment month—with NAC) were collected for proteomic analysis. The main outcome measures were to quantify protein deposition, as well as to assess the visual acuity and ocular surface symptoms before and after treatment.
Results:
Topical NAC resulted in a 20% decrease in protein deposition. This correlated with a trend for improvement in visual acuity and increased subjective improvement in vision at month 1 (P=0.0153) and 2 (P=0.0016).
Conclusions:
NAC reduced protein deposition, decreased ocular surface symptoms, and improved contact lens transparency, thereby providing increased optical clarity.
Introduction
L
In the KPro population, it has been exhibited that full-time contact lens wear is crucial in maintaining the integrity of the donor cornea ring by providing a thin fluid meniscus around the edge of the KPro front plate. Enhanced corneal moisture has been found to decrease the rate of chronic inflammation, epithelial defect, stromal melting, tissue recession from the front plate, dellen formation, resultant donor melt, and perforation.17,18 Unfortunately, due to the large diameter (16–22 mm) of these contact lenses the nature of insertion and removal is complicated and cannot be removed by the patient for routine cleaning and disinfection. Instead they are exchanged on an average every 1–3 months, exclusively during physician visits. The inability to clean these lenses is compounded by an increased level of protein accumulation, a common side effect of chronic contact lens wear.3,6–13
In recent years, mass spectrometry has been used to identify numerous proteins from the deposits on contact lenses. Proteomic analyses have revealed high levels of the following proteins: lysozyme, lactoferrin, albumin, lipocalin, lacritin, proline rich 4, keratin 1, keratin 2a, keratin 6, keratin 10, cytokeratin 2, cytokeratin 9, prolactin-induced protein, poly Ig receptor, and Ig alpha.19–22 In particular, lysozyme deposition accounts for up to 80%–90% of all protein found on silicone hydrogel contact lenses. 19 Thus, lysozyme levels are often considered the gold standard when assessing for protein accumulation.19,23
Lysozyme, lactoferrin, and various immunoglobulins, exhibit antimicrobial properties and are natural components of tear film. 24 While proteins in tear film may aid in preventing infection, once deposited on the lens surface these proteins denature and may lose their antimicrobial effect.25,26 Furthermore, the accumulation of inactive proteins on the contact lens surface may inhibit the eye's natural defenses against infections. Thus, ocular conditions, such as giant papillary conjunctivitis and increased rates of bacterial infection, have been linked to protein accumulation.3,6–13,27–29
Currently, there is no ophthalmic drug on the market to prevent the buildup of protein deposition on the surface of soft contact lenses. To date, there have been numerous studies touting the efficacy of topical or oral N-acetylcysteine (NAC) for decreasing ocular mucous plaques/buildup on the corneal surface in such diseases as keratoconjunctivitis sicca, meibomian gland dysfunction, and Sjogren's syndrome.30–34 However, NAC is more commonly utilized for reducing pulmonary mucous plugging and as a treatment for acetaminophen overdose.35–38
NAC functions as an antioxidant 39 and this study addresses the potential effect on the ocular surface. Oxidative mechanisms contribute to the development of many vision-impairing conditions of the ocular surface.40,41 Studies on mucus have shown the mechanism of action of NAC is the reduction of disulfide bonds (S−S) to sulfhydryl bonds (−SH) 42 within the glycoprotein mucin, in turn disrupting crosslinking between monomers. 41 Similarly, we postulate that the use of an antioxidant that reduces mucin oligomerization will have a downstream effect on protein deposition on the contact lens. Furthermore, this study demonstrates that the use of topical NAC can be linked to the improvement in protein deposit-related symptoms, such as decreased visual acuity and comfort.
Methods
Study design
This study was a single-center, nonrandomized, prospective trial. All patients asked to participate in this study were informed of the risks, benefits, and alternatives before participation in this study. An informed consent detailing the proposed procedures, purpose, benefits, risks, alternatives, and potential side effects, was obtained from each patient. This study was in compliance with the Health Insurance Portability and Accountability Act of 1996. The protocol was approved by the New England Institutional Review Board before initiation and adhered to the tenants of the Declaration of Helsinki.
Inclusion and exclusion criteria
Inclusion criteria for participation required all patients to have a stable ocular condition that necessitated full-time contact lens wear. All patients included had either a history of having had a Boston KPro type I and/or trichiasis secondary to Stevens–Johnson syndrome. Patients that exhibited any sign of active corneal disease on clinical exam were excluded from the study; this included corneal infection and melting/thinning around the donor cornea ring. Additionally, all patients enrolled were required to be of at least 18 years of age and not pregnant or breastfeeding. If at any point during this study, a patient satisfied the exclusion criteria, they were immediately disqualified from further participation.
Treatment protocol
Four patient visits were required to complete the study. The length of time between all patient visits was a minimum of 28 days and a maximum of 31 days. Visit 1 served as the baseline at which the first contact lens was inserted. At the second visit, the initial contact lens was removed and replaced, and the patient was started on 20% N-acetylcysteine, 1 drop 4 times daily in the affected eye. On the third visit, the contact lens was replaced and the patient continued using the medication as was directed during the period from visit 2 to visit 3. On patient visit 4, the contact lens was removed and the trial was completed. All replacement contact lenses throughout the trial were of equal size in diameter and base curve to the original baseline contact lens worn by each patient. Only Kontur Precision Sphere® contact lenses were used in this study. It has a composition of 55% water, methafilcon A.
At the beginning of each visit, the patient was evaluated twice to measure visual acuity. A standard Snellen chart was used to assess the visual acuity in change in letters. The patient's first assessment of the visit was with the contact lens in place that they had been wearing for the determined 28–31 day window. Following that measurement, it was replaced with a fresh contact lens and the visual acuity was reassessed. Furthermore, the patient was assessed for a list of their current ophthalmic drop regimen. Additionally, they were screened for any side effects or toxicity, as well as to participate in a general ocular health questionnaire. All patients were surveyed on each study visit to assess their level of foreign body sensation, mucus production, tearing, dryness, and itchiness on a scale from 0–10. Zero being asymptomatic and 10 being most symptomatic. These scores were then used to trend changes in symptoms throughout their participation in the study. Patients were also asked to grade their fluctuation of vision throughout the month on a scale from 0–10. Zero meant that there was no change/decline in vision throughout the month and 10 meant that there was a definite disabling change in vision by the end of the month before the next contact lens change. Only patients with a baseline visual acuity of ≥20/200 were included in the visual assessment analysis.
Lens collection and processing
The insertion and removal of the contact lens on each visit was done using sterile latex-free gloves. Following the removal of the contact lens, it was placed in a vial with 2 mL of a protein extraction solution [50:50 mix of 0.2% trifluoroacetic acid (TFA) and acetonitrile (ACN)]. 43 The contact lens was left in the extraction solution for a total of 24 h before removal. Upon removal, the protein solution was dried down using a vacuum centrifuge. The dried sample was then resuspended in 500 μL of 10 mM ammonium bicarbonate (Ambic) with 5% NP-40 detergent. The total protein was evaluated using a bicinchoninic acid (BCA) analysis (Pierce) with colorimetric comparison to an albumin standard through monitoring at 550 nm on a photospectrometer. 44 Digestion methodology was optimized utilizing an in-solution protocol utilizing 10 μg of protein.
Tryptic digest for proteomic analysis
Ten micrograms of each sample was denatured in 6 M guanidine hydrochloride, reduced with 10 mM DTT, and alkylated with 100 mM iodoacetamide. After overnight microdialysis in 10 mM ammonium bicarbonate, the samples were digested with trypsin (Roche) (1:50, trypsin:sample) in 10% acetonitrile (ACN) overnight at 37°C. 45 Digests were dried and resuspended in LTQ loading buffer, 3% ACN and 0.1% formic acid. All digests were performed in deplasticized tubes to reduce plastic polymer contamination.
Nano-liquid chromatography–tandem mass spectrometry
All samples were injected at a concentration of ∼50–100 ng/μL. Peptides were purified and concentrated using an online enrichment column (Agilent ZORBAX C18, 5 μm, 5×0.3 μm column, Agilent 1100 nanoHPLC). Subsequent chromatographic separation was performed on a reverse phase nanospray column (ZORBAX C18, 5 μm, 75 μm ID×150 mm column). Samples were eluted using a flow rate of 300 nanoliters/min with the following gradient profile: 0% B for 0–5 min, 0%–15% B for 5–8 min, 15%–55% B for 8–98 min, and 55%–100% B for 98–103 min (A=3% ACN, 0.1% TFA, B=100% ACN, and 0.1% TFA). This elongated method was optimized to separate complex samples. Mass spectra were collected over a m/z range of 200–2000 Da using a dynamic exclusion limit of 2 tandem mass spectrometry (MS/MS) spectra of a given peptide mass for 30 s (exclusion duration of 90 s). Compound lists of the resulting spectra were generated using BioWorks 3.0 software (Thermo Scientific) with an intensity threshold of 5,000 and 1 scan/group. All samples were injected in triplicate.
Database searching
All tandem mass spectra (.raw files) were extracted by LCQ_DTA.exe (www.matrixscience.com) for subsequent loading into the Mascot (version: 2.3.02; Matrix Science) 46 MS/MS search form or into BioworksBrowser (version 3.3.1 SP1) for subsequent analysis with SEQUEST (version 27, rev.11; ThermoFinnegan). Mascot was used to search the UniProt human database (version, 112612) (www.uniprot.org/) that contains 169,776 entries. SEQUEST and X!Tandem (Version 2007.01.01.1) were set up to search the database listed above. All searches were performed assuming trypsin digestion, with a fragment ion mass tolerance of 1.50 Da and a parent ion tolerance of 2.50 Da. Oxidation of methionine (+16) and iodoacetamide derivative of cysteine (+57) were specified as variable modifications. Additionally, all .raw files were searched in Mascot against the NCBI database with the filters for Streptococcus pneumonia, all bacteria, all fungi, and all viruses.
Calculation of false discovery rates
To calculate the false discovery rate (FDR) for each of the data sets, all .raw files were searched against a decoy database. The decoy databases contain a reversed version of the proteins included in the UniProt Human database or NCBI. The resulting files were pooled in Scaffold. The equation for the FDR is FP/(FP+TP), where FP is the total number of false positives and TP is the number of total positives found in each data set.
Criteria for protein identification
All Mascot and SEQUEST data files were compiled in Scaffold (version 3.6.1, Proteome Software, Inc.), to validate MS/MS-based peptide and protein identification. The Scaffold program adds another level of stringency utilizing the Peptide and Protein Prophet statistical analysis. Proteins and peptides were disqualified below a 95% threshold.47,48 All proteins identified were subject to manual validation for final confirmation. False positives were identified using a protein solution collected from washing an unused contact lens, handled with the same latex-free gloves.
Relative quantification and statistical analysis
Spectral counts were obtained from the scaffold output and comparisons were made from these values with the paired Student's t-test to determine significance. Similarly, paired Student's t-test was performed on all clinical data and analyzed using the statistical package within the GraphPad Prism 6 software.
Main outcome measures
The primary outcome of this study was the evaluation of the total protein deposition, as well as protein content on the contact lens surface before and after use of topical NAC. These data were obtained through liquid chromatography (LC)-MS/MS spectral counting analysis. The secondary outcome was the clinical assessment of change in visual acuity. Visual acuity was tested with a Snellen chart at 6 m and converted to log of the minimal angle of resolution (LogMAR) units for statistical analysis. The final outcome was an assessment of subjective symptoms. During every visit, each patient was required to evaluate their level of foreign body sensation, mucus production, tearing, dryness, and itchiness on a scale from 0–10. Zero being asymptomatic and 10 being most symptomatic.
Results
Patient demographics
Out of a total 16 eyes (14 patients) that were initially enrolled in the study, 10 eyes (9 patients) made it to completion. Patient No. 1 (2 eyes) and patient No. 9 (1 eye) discontinued the medication during the first month of the NAC treatment due to transient burning sensation upon installation of the drop. Patient No. 2 (1 eye) was disqualified from the study after developing viral conjunctivitis during the first month while undergoing NAC treatment. Patient No. 13 (1 eye) discontinued the medication within the first few days of NAC treatment secondary to increased blurry vision. Lastly, patient No. 14 (1 eye) was disqualified from the study because his contact lens consistently fell out in-between study visits. A listing of the demographics and background ocular history of each patient that was initially enrolled in the study is shown in Table 1. Of the patients initially enrolled, 14 out of 16 eyes had a KPro, 2 of which were bilateral KPros. Out of the 9 patients (10 eyes) that completed the study, 8 patients had a KPro and 1 had bilateral KPros. The only 2 patients that were initially enrolled in the study without a KPro both had a history of Stevens–Johnson syndrome with clinically significant conjucntival cicatrization and trichiasis, which required full-time contact lens wear to protect the corneal surface.
Patients listed in bold completed clinical trial.
Status post.
Penetrating keratoplasty.
Patient without KPro.
Patient survey and experience
All patients were surveyed on each study visit to assess external ocular surface symptoms. All results can be seen in Fig. 1. The most common complaints noted while on this medication were transient burning sensation upon instillation and unpleasant odor of medication. During the study no patient had an allergic reaction to the medication or an increase in intraocular pressure.
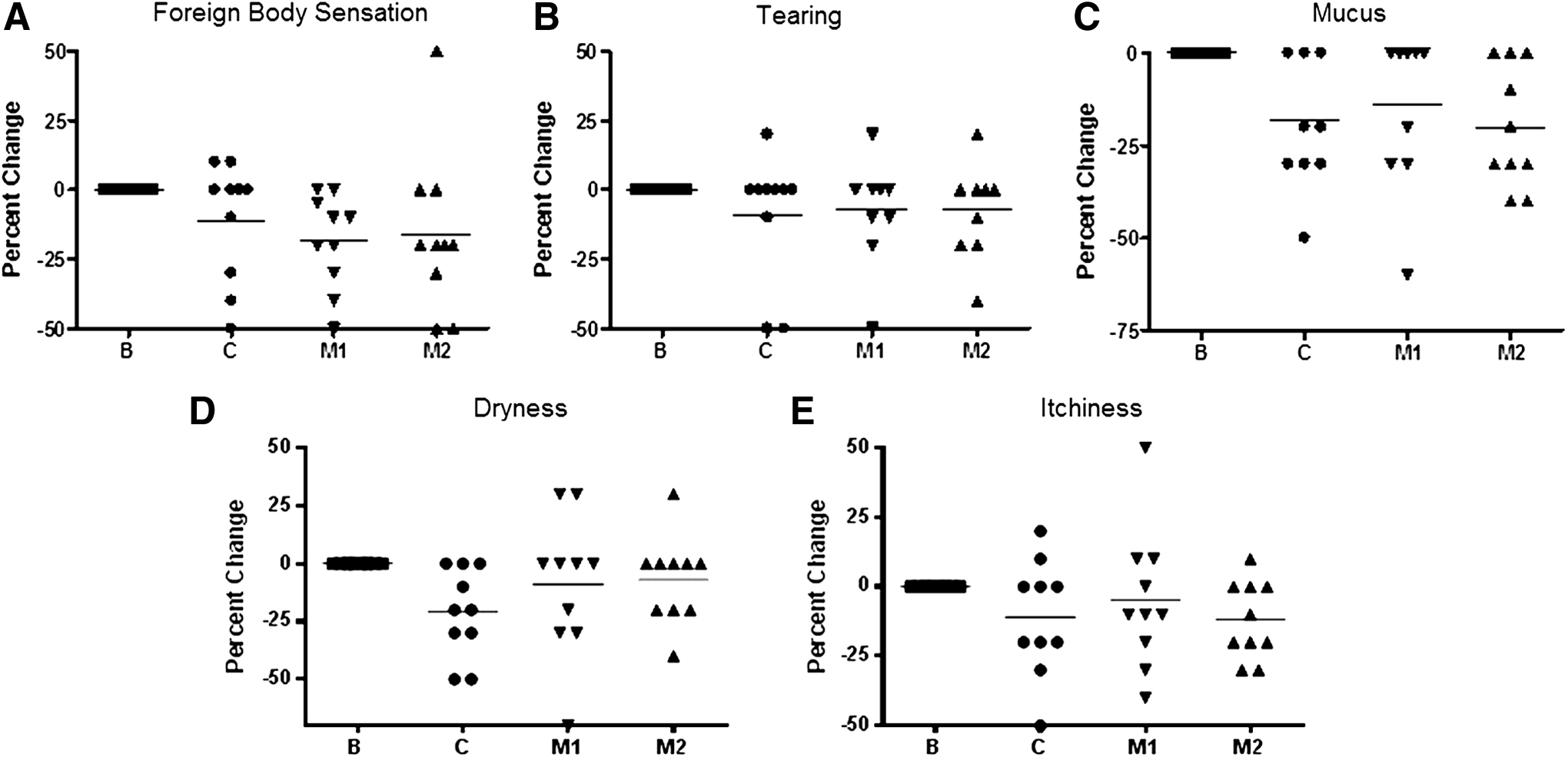
Comparison of Survey Results. For each category the baseline was normalized to zero. This enabled us to make direct comparisons of each patient based on % improvement. Baseline (B), fresh lens; control (C), 1 month of use with no drug application; M1 and M2, 1 and 2 months post drug use, respectively.
Visual outcomes
Patients were assessed for change in best corrected visual acuity (BCVA) on each visit using a standard Snellen chart. When analyzing change in BCVA, only eyes with a functional visually acuity at baseline (≥20/200) were included (7 out of 10 eyes). During the first month of the trial without NAC use, there was a mean decrease of 0.089 LogMAR. Five out of 7 patients had improved Snellen score after 1 month of NAC when compared with the control (the month prior without NAC use). Of the remaining 2 patients, 1 had no change and 1 had a decline in score. The average change in BCVA LogMAR after 1 month of NAC use was 0.031. At the second month of NAC use, 5 out of 7 patients showed improvement in LogMAR values when compared with the control month, whereas 2 out of 7 patients showed a decline. When compared to the control, the average change in BCVA LogMAR after 2 months of NAC use was 0.029. Although changes in vision were not shown to be statistically significant, there was a clear trend seen when compared to baseline visual acuity with fresh contact lens and the control month without NAC use that pointed toward improvement in vision closer to baseline with the use of NAC (Fig. 2).

Comparison of visual acuity. Top. Baseline (B), fresh lens; control (C), 1 month of use with no drug application; M1 and M2: 1 and 2 months post drug use, respectively. There is a clear decrease in visual acuity after 1 month of wear as compared to the fresh lens (P=0.1300); however, after 1 (P=0.6278) and 2 months (P=0.7171) of drug use when compared to the control period, the visual acuity level increases and are more similar to the baseline. Bottom. Mean change in LogMAR over time.
Changes in visual acuity directly correlated with improvement in protein deposits noted on the contact lens surface (Fig. 3). Therefore, patients were also asked to subjectively assess their visual acuity with regard to decrement throughout the month, a common complaint of chronic contact lens wearers. Patients showed a significant improvement in their subjective visual acuity throughout month 1 and 2 while on NAC when compared to the control month (Fig. 4).
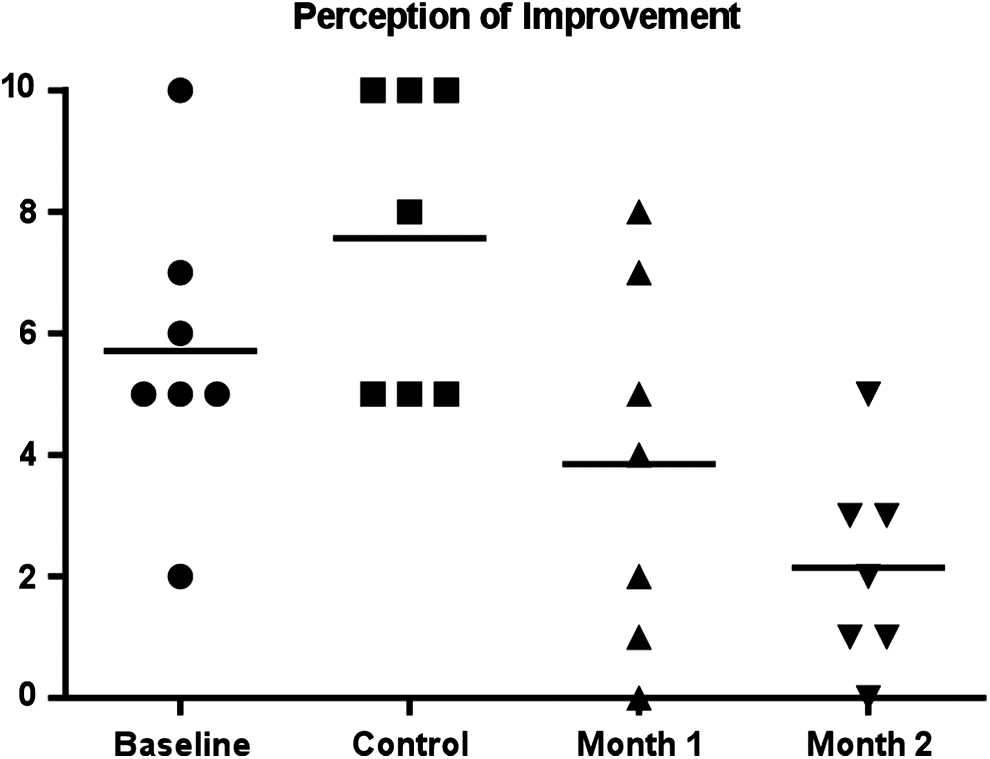
Comparison of perception of visual acuity. Baseline (B), fresh lens; control (C), 1 month of use with no drug application; M1 and M2: 1 and 2 months post drug use, respectively. There was a significant trend toward subjective improvement in visual acuity (C vs. M1: P=0.0153; C vs. M2: P=0.0016).

Clinical results for patient No. 11. Before the application of NAC (left) and after the application of NAC (right). Diffuse protein deposits are observed only on the contact lens surface before the initiation of NAC (left).
Mass spectrometry data
From each eye included in the study, contacts lenses were analyzed at 2 time points. The lens collected at visit 2 served as the control, representing typical protein deposition after 1 month of wear without the drop. The second time point was at visit 3, 1 month post application of the NAC drop. Since many of the patients had different underlying diseases and used varying topical medications, this design allowed for direct comparative data, having the first month serve as their own control.
The concentration of protein extracted from each lens was determined by BCA assay and used for all downstream proteomic analyses. The total amount of peptides identified in each contact lens extract through the LC-MS/MS analysis was normalized to the corresponding total protein yield observed by BCA. Both the BCA data (data not shown) and the average spectral count (P=0.284) showed a trend in protein reduction. Figure 5 shows the percent change in protein abundance as extrapolated from matched mass spectra after normalization to total protein observed by BCA. The majority (8/10) of patients saw a decrease in the protein levels and 2/10 saw an increase in protein levels. The average protein decrease was 20% (Fig. 6).

The percent change in protein abundance as extrapolated from matched mass spectra after normalization to total protein observed by BCA. Majority (8/10) patients saw a decrease (negative change in %) in the protein levels and 2/10 saw an increase (positive change in %) in protein levels. Average protein decrease was 20%.

Change in the number of peptides identified during the analysis of each sample after normalization to total protein observed by BCA. The average decrease is 10k counts (P=0.284).
Contact lens proteome analysis
A shotgun proteomic analysis was conducted and allowed for the identification of over 85 proteins across the 20 lens extracts. The dominant proteins identified on the lenses included previously reported tear film proteins such as lysozyme, keratin, and albumin.19–22 Based on SDS-PAGE and Western blot analyses, the samples are consistent with the literature, indicating that lysozyme is the most dominant band and often the only protein visualized by Coomassie staining (data not shown). The spectral count analysis corroborates, identifying the most abundant protein in the majority of contact lens extracts as lysozyme (66%) followed by albumin (16%). In fact, there was a statistically significant (P=0.0186) increase in the level of lysozyme (Fig. 7a). Although overall there was a trend toward an increase in total keratin (Fig. 7b, P=0.2368). In addition, there were global trends in decreased lactoferrin and increased matrix metallopeptidase-16 (Fig. 7c). Of note, spectral counts identifying mucin were relatively low in both control and 1 month post-NAC treatment. In theory, mucin should be very abundant on the ocular surface; however, based on the method of detection used in this study and the high level of glycosylation of this protein, low spectral counts are not surprising.

Individual protein spectral counts.
Microbial findings
Our global analysis included a screen for the presence of peptides unique to specific microbial pathogens, including bacteria, fungi, and viruses. Of the 20 lens extracts tested, 3 were noted to have bacterial pathogen contamination in the month before NAC use and 1 after. Specifically, we identified Escherichia coli both before and after NAC treatment in patient No. 5, whereas S. pneumonia and E. coli peptides were identified in patients No. 11 and No. 12, respectively, only in the month before NAC use.
Discussion
The aim of this study was to evaluate the efficacy of topical NAC for decreasing the level of protein deposition on the surface of long-term contact lenses, with the end goal of increasing patient comfort and visual acuity. The majority of patients in this study had a positive experience with the use of topical NAC with regard to improvement in their eye health and comfort when compared to baseline. A statistically significant decrease in mucus production and foreign body sensation was observed, which is consistent with published studies wherein topical NAC was used to treat meibomian gland dysfunction and Sjogren's syndrome.29,30 Williamson et al. noted that patients with Sjogren's syndrome and dry eye not amenable to prior treatment with artificial tears alone had a 30% response rate of improvement in subjective and objective findings when trialled on 20% NAC. 31 This percentage is in line with our results—3 out of 9 patients (33%) experienced beneficial outcomes and continued using the medication after the 2 month trial period. A trend in the improvement of dryness and itchiness corroborates with previous studies and indicates efficacy for the use to treat these symptoms.29,30 Ocular surface disease and the associated symptoms are often related to one's inflammatory status. The antioxidant properties of NAC may help to reduce the oxidative stress associated with inflammation, as seen in many of the patients included in this study who display hyperinflammatory conditions.
The most common complaint amongst patients before NAC use was progressive decline in visual acuity before the exchange of new contact lens. The population of patients that were most apt to notice these subtle changes and fluctuations had functional baseline visual acuity (≥20/200). Accordingly, the patients in this study who felt that they had experienced the greatest benefit from NAC use were those that could perceive the results. In our study, 5 out of 7 patients had an improvement in their visual acuity with NAC use and often these patients showed continued improvement upon month 2 of NAC use. In addition, the improvement in LogMAR correlated with the subjective improvement in fluctuation in vision throughout the month as reported by the majority of patients who participated in the study. The authors would like to address the outlier who experienced a drop in vision while on NAC. During the second month of NAC use, patient No. 8 (2 eyes) displayed a decline in visual acuity. This patient had a history of advanced glaucoma in both eyes. Oftentimes, she had difficulty with vision testing due to significant scotomas in her visual field. Therefore, although we included her data as part of the full analysis because her baseline vision was ≥20/200, we feel that it may not have been reliable and conversely affected the integrity of the visual acuity results.
When applied topically to the ocular surface, NAC was well tolerated by the study group and no adverse events were reported. The most common complaint with NAC usage was transient burning upon instillation. In addition, an unpleasant odor of medication was noted. The safety profile of this medication is consistent with previously reported studies using NAC topically on the ocular surface.30–32
Current contact lens cleaning solutions available have been shown to remove daily accumulation of lysozyme, lactoferrin, and lipocalin. 20 Full-time contact lens wear has the disadvantage of protein buildup due to the deviation from preferred daily contact lens removal and cleaning protocols. In our patient population it is not uncommon for these contacts to be in use for up to 12 weeks, during which detrimental levels of tear proteins accumulate, inhibiting visual clarity and hindering the natural ability of the eye to ward off infection. The most abundant proteins naturally found on the ocular surface aid in combating pathogens. Numerous studies have reported up to 80%–90% of all protein recovered from the contact lens surface to be lysozyme.19,23 Interestingly, despite an overall decreased level of protein accumulation on the contact lenses post-NAC use, lysozyme quantities increased significantly. One can hypothesize that this serves as a positive side effect to NAC use, and may improve the external ocular surface environment. One caveat to this theory was our inability to decipher the active versus inactive form of lysozyme; although a decrease in microbial buildup is consistent with an increase in the enzymatically active form. We also found an overall uptrend of total keratin deposited. Certain patients did experience a significant rise in total keratin levels, patient No. 4 (P=0.0038) and No. 6 (P=0.053). We felt that this may have been linked with the subjective complaints of increased itchiness that these patients experienced after 1 month of NAC use. We postulate that this is related to the significant converse trend observed in lipocalin abundance in both patient No. 4 (P=0.0038) and No. 6 (P=0.0079). Tear lipocalin deficiency has been linked to dry eye syndrome and an increase in mucus; notably patient No. 6 had the highest mucus levels reported throughout this study and patient No. 4 had an increase in mucus after 1 month of NAC use.
Patients with KPro type I are especially vulnerable to microbial infections which often lead to corneal melt and endophthalmitis.49,50 Furthermore, routine culturing of the contact lenses worn by KPro patients has demonstrated that a high prevalence of microbes can be isolated. 51 For these reasons, patients with KPro type I are routinely prescribed prophylactic dual topical antibiotic therapy to prevent microbial infections. In our patients, we prescribe topical fortified vancomycin in combination with a fourth-generation fluoroquinolone to prevent such complications. Although we do not make the claim in this study that NAC has antimicrobial properties, we would like to note that out of the 3 patients found to have peptides specific for microbial pathogens by LC-MS/MS analysis during the control month, 2 of the patients did not have these bacterial contaminants present on their lenses upon follow-up analysis post-NAC use. It is known that protein deposits and the subsequent accumulation of biofilm buildup on the contact lens surface is a common harbinger of microbial disease.3,6–13 We speculate that decreased protein and biofilm loads found on the contact lenses post-NAC use may have aided in preventing microbial overgrowth.
Given the low incidence of KPro performed worldwide, roughly 6,000 cases since the year 2000, 52 the enrollment of 14 patients (16 eyes), is high for any single site study. Although the authors acknowledge that improved data and analysis may be found if this study was to be repeated as a larger multicenter study, it is important to note that this study was aimed at analyzing patients with large-diameter contact lens that are normally worn for prolonged periods (4–12 weeks), and those with a KPro. A second limitation to this study is compliance. For this population of patients the average number of prescriptive topical medications used before beginning the study was 4.9 topical medications (range 2–7). The addition of an extra medication can often be quite challenging, especially given the varying degree of visual impairment and social support. Finally, the lack of a control group in this small pilot is a noteworthy limitation; future research may involve a double-masked, randomized, controlled trial to mitigate any observer and/or patient bias. Additionally, these future studies may allow for further evaluation of antibiotic prophylaxis regimens and long-term safety of NAC.
The results of this prospective clinical trial suggest that topical administration of NAC is an effective and well-tolerated topical medication to treat protein deposition in patients with chronic contact lens use. It may aid in improving visual acuity and comfort. The ramifications of this may lead to improved ocular surface health, a decreased rate of infection or corneal melt, and prolonged time intervals between patient visits for routine contact lens exchange and surveillance. We believe that this pilot study establishes the efficacy of topical NAC use, although we feel that a larger population controlled clinical trial with a longer follow-up period is necessary to corroborate our results.
Footnotes
Acknowledgments
Design and conduct of the study (J.N.K., N.A.K.G., C.S.F.); collection (J.N.K.), management (J.N.K., C.S.F.), analysis (J.N.K., N.A.K.G.), and interpretation of the data (J.N.K., N.A.K.G.); and preparation, review, and approval of the article (J.N.K., N.A.K.G., C.S.F.).
Author Disclosure Statement
No competing financial interests exist.