
Abstract
Abstract
Purpose:
To evaluate the efficacy and safety of preservative-free triamcinolone acetonide (Triesence) for the treatment of macular edema.
Methods:
A retrospective study was conducted on patients who attended a tertiary retinal clinic from June 2009 to July 2012 with macular edema due to various causes. Patients who received at least 1 intravitreal Triesence injection and completed 6 months of follow-up were recruited. Data, including best-corrected Snellen visual acuity, central macular thickness (CMT), intraocular pressure (IOP), and adverse events (AEs), were collected at baseline, week 1, month 1, month 3, and month 6 after initiation of treatment. Snellen visual acuity was converted to visual acuity score (VAS) for statistical analysis using paired t-tests and linear regression.
Results:
One hundred two eyes from 102 patients were included in the study. Mean VAS was significantly improved at all follow-up time points compared to baseline (P≤0.002), with highest mean gain at month 1 (6.1±8.9 letters). Mean CMT decreased significantly at all follow-up points compared to baseline (P≤0.0005), with the greatest reduction at week 1 (146.6±109.4 μm). A total of 22 AEs were observed, and IOP elevation was the most common AE related to Triesence treatment (17/22, 77.3%). No sterile or infectious endophthalmitis was observed.
Conclusion:
Intravitreal Triesence improves visual acuity and reduces macular thickness in eyes with macular edema from various causes. Treatment-associated IOP elevation was manageable with antiglaucoma medications. There were no serious vision-threatening complications associated with intravitreal Triesence therapy during the study period.
Introduction
M
There have been many studies, including large randomized clinical trials, on the treatment of macular edema with intravitreal triamcinolone acetonide (IVTA).7–9,15,16 The most commonly used triamcinolone acetonide (TA) preparation that has been studied is Kenacort. Although Kenacort has been shown to be effective in the treatment of macular edema, it is associated with significant ocular adverse events (AEs), including elevated intraocular pressure (IOP), cataract formation, and acute noninfectious endophthalmitis.10,12,17 The toxic reaction of Kenacort is believed to be related to the preservative vehicle (benzyl alcohol).18–20 It is noted that Kenacort formulation is not designed initially for intraocular use.
Preservative-free formulations of TA (PFTA), including Trivaris (Allergan, Inc., Irvine, CA) and Triesence (Alcon Labs, Fort Worth, TX), have recently been developed and have addressed concerns regarding local toxicity of the vehicle and preservatives. The SCORE and DRCRnet clinical trials have confirmed the effectiveness and safety of Trivaris in treatment of macular edema secondary to retinal vein occlusion and diabetes mellitus.7,8,15 However, as Trivaris is not commercially available, Triesence remains the only commercially available Federal Drug Administration-approved PFTA. This PFTA was initially developed for the treatment of inflammatory ocular conditions and visualization of tissue planes during retinal surgery. It is now also used in an off-label setting to treat macular edema. 10 Previous studies found that the physical properties of Triesence were different from those of Trivaris, which leads to different intraocular pharmacokinetics.21,22 This may imply a different effectiveness and safety profile for treatment of macular edema from both drugs. There have been no published clinical data on the safety and efficacy of intravitreal Triesence in the treatment of macular edema in a clinical setting.
The aim of this study was to evaluate the safety and efficacy of intravitreal Triesence in the clinical treatment of patients with macular edema from differing etiologies.
Methods
Medical records of the patients attending a tertiary retinal clinic for treatment of macular edema between June 2009 and July 2012 were retrospectively reviewed. Patients who received at least 1 intravitreal Triesence injection and completed 6 months of follow-up were included in the study.
Exclusion criteria applied to the study eye were as follows: intravitreal Kenacort therapy or focal laser treatment in the macular region within 3 months before commencement of Triesence; previous anti-VEGF injection in the study eye within 2 months before initial intravitreal Triesence and uncontrolled glaucoma in the study eye (IOP ≥25 mmHg or on more than 2 antiglaucoma medications). If both eyes were eligible for the study, 1 eye was randomly selected and included in this study. All methods adhered to the tenets of the Declaration of Helsinki guidelines for research in human subjects, and institutional ethics approval was obtained for this study.
The efficacy of Triesence therapy was evaluated by visual functional and macular anatomical outcomes. Best-corrected visual acuity (BCVA) was assessed using a Snellen chart and converted to the visual acuity score [VAS=85+50×Log (Snellen fraction)]. 23 Central macular thickness (CMT) was measured using spectral domain optical coherence tomography (Spectralis HRA+OCT, Heidelberg Engineering, Heidelberg, Germany or Cirrus HD-OCT, Carl Zeiss Meditec, Dublin, CA). Each individual patient was examined using the same OCT machine throughout the entire study period.
Safety of Triesence treatment was evaluated by IOP and ocular-related AEs. IOP measurement was performed using the Goldmann applanation tonometry. IOP ≥25 mmHg or ≥10 mmHg above the baseline level at any follow-up visit was defined as a significant IOP elevation.24,25 Up to a maximum of 3 antiglaucoma medications, including the patients' existing IOP-lowering medication, were allowed to be administrated if IOP ≥25 mmHg.
Data, including BCVA, CMT, and IOP, in all patients were retrieved before Triesence treatment (Baseline) and at week 1, month 1, month 3, and month 6 after initiation of the treatment. The numbers of injections and AEs for each patient in the study were recorded at each visit. Patients who failed to respond or responded poorly to Triesence therapy (visual loss >2 lines and increase in CMT >100 μm comparing to the baseline) or had significant AEs after 6 months of treatment were offered other therapies. Since advanced cataract formation is unlikely to be observed within a 6-month IVTA treatment period, we further collected safety data from patients who did not switch to other therapy up to 24 months after Triesence initiation as a supplement of this 6-month study.
The study drug was manufactured as a sterile, preservative-free, single-use, intravitreal injectable suspension of 40 mg/mL TA (Triesence, Alcon Labs, Fort Worth). Intravitreal injections were performed under the sterile conditions and topical anesthesia by a single vitreoretinal surgeon (A.A.C.) in an ophthalmic procedure room. After instillation of 1% proparacaine anesthetic drops and preparation of the injection site with 5% povidone–iodine, 4 mg Triesence in 0.1 mL was injected into the vitreous cavity 3–4 mm posterior to the limbus with a 30-gauge needle. Chloramphenicol eye drops were administered for 1 week postinjection. A follow-up phone call to monitor postinjection AEs was conducted within 24 h after the injection.
Repeated injections were performed in eyes with persistent or recurrent macular edema and met at least 1 of the following criteria: (1) loss of visual acuity of 2 or more Snellen chart lines with fluid in macula showing on OCT scan; (2) an increase in CMT of ≥100 μm comparing to the baseline or previous results; and (3) evidence of persisting fluid on OCT scan 2 months after the previous injection.
Statistical methods
Data are summarized as frequencies and percentages, or mean±standard deviation. Paired t-tests were used to evaluate the change in VAS, CMT, and IOP at each follow-up time point compared to their baseline levels. Regression analysis was used to evaluate the associations between various factors, including baseline VAS/CMT and the initial diagnosis subgroup, and change from baseline to 6 months for VAS/CMT outcome. P values≤0.05 were considered to be statistically significant. Statistical package for the social sciences (SPSS Version 19.0.0.1, 2010; IBM, Chicago, IL) was used for all statistical analyses presented here.
Results
The study included 102 eyes from 102 patients satisfying the inclusion and exclusion criteria. Table 1 shows the baseline characteristics of these patients. There were a total of 159 intravitreal injections during the first 6-month follow-up, while 56.9% of eyes had a single Triesence injection, 30.4% had 2 injections, and 12.7% had 3 injections. Eyes with macular edema due to diabetes mellitus had a lower multiple injection rate (26.1%, 6/23) compared to other etiologies [post-pars plana vitrectomy (PPV) with 57.1% (8/14), central retinal vein occlusion (CRVO) with 52.0% (13/25), branch retinal vein occlusion (BRVO) with 50.0% (5/10), and postcataract surgery with 36.4% (4/11)].
Other diagnoses include uveitis, macular telangiectasia, epiretinal membrane, retinal schisis, and tractional maculopathy syndrome.
BRVO, branch retinal vein occlusion; CRVO, central retinal vein occlusion; DME, diabetic macular edema; PDT, photo dynamic therapy; PPV, pars plana vitrectomy; SD, standard deviation.
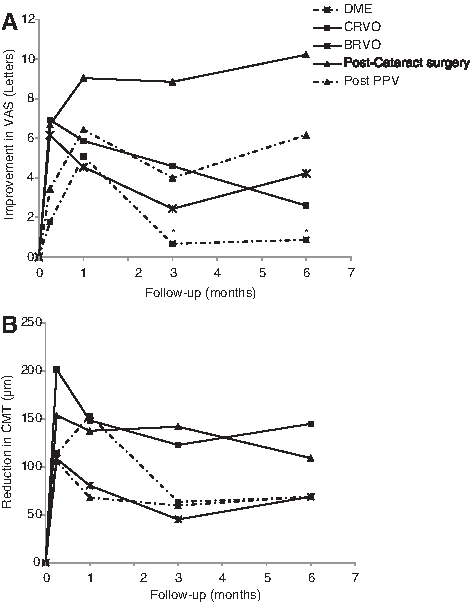
VAS change after Triesence treatment, at various times until 6 months, is shown in Table 2. Mean VAS was significantly improved 1 week after the initial injection (P<0.0005), while there was no significant further improvement thereafter over the 6 months of follow-up (P>0.05). Table 3 and Fig. 1A show the mean change in VAS at each time point from baseline by the diagnosis subgroup, including diabetic macular edema (DME), CRVO, BRVO, post-PPV, and postcataract surgery. VAS of the postcataract surgery group had the highest improvement through 6 months of the follow-up period and the vision increased by 10.2 letters over the 6 months. The DME group showed a clear VAS increase until month 1, but the average VAS returned to about baseline level thereafter. Among all factors, including age, gender, baseline VAS, history of diabetes, hypertension, hypercholesterolemia, lens status, and prior PPV, only baseline VAS was found to be negatively associated with vision (VAS) change over the first 6 months among patients without hypertension (P<0.004). That is, a poorer baseline VAS was associated with a greater improvement in VAS. However, such an association was not detected among patients with hypertension (P=0.99). The diagnosis subgroup was not shown to be associated with the change after adjusting for other factors studied, possibly due to small numbers of patients.
Change in visual acuity score (VAS)
P-value comparing to baseline by paired t-tests.
Other diagnoses include uveitis, macular telangiectasia, epiretinal membrane, retinal schisis, and tractional maculopathy syndrome.
P-value from paired t-test of baseline, no change.
Change of postinjection value from baseline value.
There were significant reductions in macular thickness at each follow-up point compared to the baseline (P≤0.0005, Table 2). The greatest reduction occurred at week 1 in most of the diagnosis subgroups, except for the DME group with CMT change peaked at month 1 (Table 3 and Fig. 1B). Regression analysis found that eyes with thicker baseline CMT were more likely to have a greater improvement (reduction in CMT) over 6 months of follow-up, even after adjusting for age, gender, and other potential confounding factors (P<0.0005).
Eighteen patients (17.6%) experienced at least 1 ocular AE during the 6-month follow-up (Table 4). A total of 22 AEs were observed and 4 eyes had 2 AEs during the 6-month follow-up period. IOP elevation was the most common AE (17/22, 77.3%), 70.6% (12/17) of which occurred within the first month after Triesence injection. The average IOP elevation from the baseline was 1.6±4.6 mmHg at week 1 (P=0.002) and 1.2±5.0 mmHg at month 1 (P=0.032), and the IOP returned to the baseline level after month 1 (all Ps>0.05). Elevated IOP was controlled in 10 of 15 eyes (75%, IOP measurement ≤21 mmHg) with the administration of antiglaucoma medications. Three patients with elevated IOP after the initiative of Triesence returned to ≤21 mmHg after being observed for 3–4 weeks without treatment. The other 2 eyes were not treated due to their maximum IOP value being less than 21 mmHg. Two eyes (9.1%) experienced mild vitreous hemorrhage and 1 eye suffered a subretinal hemorrhage. No eyes underwent cataract surgery due to advanced cataract formation within the 6-month follow-up period. There were no cases of sterile or infectious endophthalmitis related to Triesence use and no other serious procedure-related complications, including retinal detachment or lens penetration, during the 6-month follow-up period.
AE, adverse event; BL, baseline; IOP, intraocular pressure.
After the initial 6 months, 28 patients (27.5%) switched to intravitreal Avastin injection, 28 patients (27.5%) were lost to follow-up, and 46 (45.1%) continued Triesence treatment and had been followed up until month 24. In the 46 eyes with Triesence treatment for 24 months, VAS, CMT, and IOP maintained stable compared to the 6-month treatment outcomes (all P>0.05).
During the period of month 6 to month 24, a total of 17 AEs were observed in 46 eyes. IOP elevation was still the most common complication among all AEs (11/17, 64.7%), followed by pain in the eye (1/17, 5.9%), floaters (1/17, 5.9%), vitreous hemorrhage (1/17, 5.9%), retinal detachment (2/17, 11.8%), and cataract removal surgery due to advanced cataract formation (1/17, 5.9%). No cases of sterile or infectious endophthalmitis were observed during this extended study period. In patients who missed follow-up or switched to Avastin treatment, no AEs were observed at their last visit or the visit before switching treatment, except one single case of IOP elevation of 30 mmHg at month 15 was detected and this patient then was lost to follow-up afterward.
Discussion
Vision and CMT
Our study demonstrates that most patients experienced significant anatomical improvement (CMT reduction) 1 week after initiation of Triesence treatment, and was maintained for the rest of the 6 months. The maximum visual improvement occurred subsequent to the anatomical change and was also maintained for the next 5 months for most etiologies. Eyes with a poorer visual acuity and higher CMT value at baseline were more likely to have greater improvement at month 6, which may be partly explained by a ceiling effect of vision. Our findings show that those with good vision and minimal edema have less potential to improve, whereas eyes with more severe macular edema and poorer baseline vision having a greater potential for improvement suggest that patients with advanced maculopathy may benefit from treatment and should be encouraged to receive treatment to improve their vision.
It is worthy noticing that although statistically a meaningful change is usually considered as at least 1 line, or 5 letters change in VAS in the follow-up visits compared to the baseline, this does not seem to be true for all the conditions. For example, in our DME subgroup, VAS improvement was not as significant as CMT reduction and did not reach the 5-letter statistically significant level. In addition, in the cases of prolonged vision damage, it is difficult to obtain statistical 5-letter improvement. Therefore, in a real clinical situation, the treatment given to the patients may be considered to maintain the VAS and reduce further retinal damage rather than the improvement of VAS at the statistically significant level.
Etiology-based analysis
Patients with pseudophakic macular edema were the most likely to have a favorable functional and anatomical outcome. Although the pathogenesis of pseudophakic cystoid macular edema is complex and multifactorial, acute inflammation caused by surgical manipulation appears to be the trigger. 11 This acute inflammatory reaction potentially responds well to intravitreal steroid injections.
In contrast, patients with DME demonstrated transient visual improvement even though significant anatomical improvements were achieved at all follow-up time points. Grenga et al. studied patients with persistent DME and also observed transient visual acuity improvement at month 1 with a return to baseline level at month 6. 26 The inconsistent correlation between vision and OCT change in diabetic maculopathy suggests that macula edema is not the only cause of vision loss in diabetic patients and is consistent with previous study results. 27
Safety
The SCORE study reported elevated IOP as the most common complication associated with 4 mg intravitreal Trivaris treatment. Approximately, 26%–36% of eyes had an IOP rise of >10 mmHg above baseline, 35%–41% of them required IOP-lowering medication.7,15 In our study, 16.7% of eyes had IOP ≥25 mmHg or an IOP elevation of >10 mmHg from the baseline level, 75% of them required topical medical therapy. The lower rate of IOP elevation associated with Trisence in this study may be due to the shorter study follow-up period (6 months) and a smaller and more heterogeneous study population compared to the SCORE study. The different physical properties of the 2 PFTA preparations may also contribute to the variable pharmacokinetics in eyes influencing their IOP elevation profile.21,22
Intraocular inflammation is a potentially serious side effect of non-PFTA treatment and has encouraged the development of PFTAs such as Triesence.28,29 The occurrence of sterile endophthalmitis associated with non-PFTA injections reported in studies ranges from 0.20% to 6.73%.29–32 In our study, there were no cases of infectious or noninfectious endophthalmitis during the observed period. This is consistent with the low rate of inflammatory reactions observed with Trivaris in the SCORE study (0.1%).7,15 The single treating physician in a single study center with an established standard practice protocol for patient assessment, treatment in an operating theatre setting, and post-treatment phone call follow-up may also contribute to the low serious AE rate in our study.
The SCORE study reported that 33%–35% of phakic eyes experienced progression of lens opacity after Trivaris treatment, resulting in 2.8%–4.5% of eyes undergoing cataract surgery in the 12-month period.7,15 In our study, 50% of the eyes were phakic, with no eyes undergoing cataract surgery during the 6-month follow-up period. Our 24-month follow-up data showed similar results, with 2.2% of eyes (1/46) undergoing cataract surgery due to advanced cataract formation after 6 months of initial treatment. However, 2 cases of retinal detachment were observed for the extended study period.
Limitations
This is a relatively small, clinic-based short-term retrospective study; however, data were adherent to the collection time point to warrant the accurate information provided to the study. In clinical practice, the patients who did not respond or poorly responded to the Triesence after the 6-month period were generally offered alternative therapies. Six months of data collection and study period are therefore an appropriate period to evaluate the efficacy and safety of Triesence in the treatment of macular edema. Progression of cataract associated with Triesence treatment could not be evaluated due to a lack of regular lens opacity grading data and the short time course of the study than the timing of intravitreal steroid-related cataract progression.7,15 Further studies are required to more comprehensively define the safety and efficacy profile of this medication.
Conclusions
Our study showed that Triesence was effective in improving visual acuity and reducing macular thickness in eyes with macular edema. Patients with pseudophakic macular edema were more likely to have the best visual and anatomical outcomes with Triesence treatment and those with DME responded less favorably. Triesence-induced IOP elevation was manageable with antiglaucoma medications. There was no sterile endophthalmitis associated with intravitreal Triesence therapy. Therefore Triesence may be considered as an efficacious and safe alternative steroid preparation for the treatment of macular edema.
Footnotes
Acknowledgment
Partial statistical support from Dr. Alexandra Bremner (School of Population Health, The University of Western Australia, Australia).
Author Disclosure Statement
No competing financial interests exist.