
Abstract
Abstract
Purpose:
To measure the penetration of fluorescein into the anterior ocular compartments after exposure of the cornea to a mist of aerosol droplets.
Methods:
This was an open-label proof-of-principle trial. Eighteen healthy volunteers were asked to participate. A conventional (50 μL) drop of fluorescein solution (20 mg/mL) was administered to the right eye; an ocular mist (10 μL) of the same solution was applied to the left eye. Autofluorescence (photons/s) was measured in the cornea, the anterior chamber (AC), and the lens before administration and at 1, 2, 5, 10, 20, 50, and 100 min thereafter. The area under the curve (AUC) was calculated. For the vitreous cavity, measurements were performed at baseline and after 100 min.
Results:
All participants completed the study. AUC (mean±SD) for the cornea was (363±431)×104 photons after drop application and (154±265)×104 photons after the mist (P=0.005). For the AC, these values were (6.9±10.3)×104 and (2.9±5.4)×104 photons, respectively (P=0.14). Autofluorescence data obtained in the lens did not allow reliable AUC calculations. Autofluorescence in the vitreous at 100 min did not significantly exceed the level at baseline.
Conclusion:
It was demonstrated that fluorescein applied to the ocular surface with the spray device enters the AC. The total amount of fluorescein molecules reaching the ocular surface by the 2 methods of administration, however, is not equivalent. Therefore, no definitive conclusions on relative bioavailability can be drawn from this experiment.
Introduction
D
Spillover and lacrimal clearance are largely due to the excessive volume of eye drops, varying from 25 to 70 μL depending on factors such as surface tension of the drop, angulation of the bottle during application, tip aperture diameter, and design of the eye dropper nozzle. 4
Systemic absorption after administration of ocular medication by means of drops can lead to symptomatic side effects. 5 The most prominent route of absorption is through the mucous membranes of the fornix, lacrimal, nasopharyngeal, and gastrointestinal tract. In this respect, beta-receptor blocking agents prescribed for glaucoma probably are the best investigated pharmaceutical agents. 6
A decrease in the volume of drug solutions applied to the eye would be desirable to reduce the amount of overflow, the rate of drug loss through drainage, the incidence of systemic side effects, and the cost of therapy. 4 For the administration of tropicamide 1%, for instance, a mist delivery system can be equally effective as conventional eye drops. 7 While the same concentration of tropicamide was used in both the drop and mist fluid, the volume applied to the ocular surface could be reduced by a factor 5 (ie, 6 instead of 30 μL).
Adherence to medication therapy depends, among other factors, on the specific condition and/or the characteristics of administration. A review of (a diversity of) compliance and persistency studies of glaucoma treatment (with equally diverse definitions and methods of measurement) demonstrates that noncompliance and discontinuation constitute a serious problem in optimizing patient care. 8 Self-instillation of eye drops is a generally acknowledged impediment affecting compliance, especially in the elderly, with obvious consequences for the effectiveness of ocular drug treatments.
One of the major reasons for failure of proper eye drop instillation is the incorrect positioning of the bottle relative to the eye. For conventional administration of eye drops, the head should be in a more or less horizontal position with the eye in upper gaze. The bottle has to be kept closely, and approximately vertically, above the eye. For many patients, especially those with (surgical) ocular wounds, reduced visual acuity, or reduced motor function, this can be an obstacle for correct application of the eye drops. Additional concerns are the risk of the eye to be traumatized by the nozzle tip of the bottle and infection of the nozzle by (peri)ocular flora. Many patients, therefore, rely on the help of either relatives or caregivers. Both the suboptimal treatment due to noncompliance and the involvement of professional caregivers will increase the overall costs of ophthalmic medical care.
Using monodisperse spray nozzles and mechanically driven dosage systems, an ophthalmic mist delivery device has been developed, which generates aerosols with a prespecified particle size distribution. In comparison to conventional eye drops, the advantages of this type of administration are manifold: (1) dosage can be much more accurately adjusted (ie, reduced), (2) medication can be applied in an upright position with the patient looking straight ahead (eg, in a mirror), (3) the mechanical impact of the mist on the ocular surface is minimized, and (4) a reduced risk of ocular touch by the device. The reduction of both volume and impact will (at least partially) prevent lacrimal clearance and blinking reflexes, which are quite common with conventional eye drops.
To improve the convenience of drop application by (elderly) patients and, thus, promote patient compliance, the spray device has an extension, which both makes contact to the orbital rim and slightly spreads the eyelids.
In this study, we compared the ocular penetration of fluorescein applied by this new delivery device and as conventional eye drops. As a measure for intraocular fluorescein concentration, the autofluorescence level was assessed in various anterior compartments.9,10
Methods
This study adhered to the tenets of the Declaration of Helsinki, was approved by the Medical Ethics Committee of the Erasmus Medical Center (Rotterdam, The Netherlands), and is registered on www.trialregister.nl (NTR3404). This study was designed as an open-label proof-of-principle trial for which 18 healthy volunteers (age >18) were recruited, all of whom provided written informed consent. Exclusion criteria were as follows: allergy/hypersensitivity to fluorescein, previous ocular surgery (including refractive laser surgery), corneal condition (eg, Sjogren syndrome, herpetic eye disease), other ocular morbidity, contact lens wear, concurrent use of eye drops, and pregnancy.
Administration of fluorescein (20 mg/mL) was performed in a standardized way by the same experienced optometrist in all subjects. With the subject's head tilted 30° backwards and the lower eyelid pulled down, a conventional drop was applied to the right eye by means of a laboratory quality adjustable pipette held in the vertical position with its tip close to the cul-de-sac. Drop volume was kept at 50 μL. With the subject's head in a normal upright position and the device kept horizontal in front of the eye (Fig. 1), fluorescein was applied as a mist to the left eye by an experimental mechanically controlled device.

Partial cross-section of the newly developed spray device for the delivery of topical ocular medication and its (horizontal) positioning relative to the eye.
This medical device was developed by Medspray (Enschede, The Netherlands), together with their partner SHL Medical (Nacka Strand, Sweden), under ISO13485. It is based on prototyped parts, except for the spray nozzle units, which were from serial production. The core of the device is a 1-mL glass syringe (which can hold up to 100 doses) with a microspray nozzle on the luer tip of the syringe. The eye spray device generates a soft mist (actuation time 1.5 s) tolerable to the bare eye. The device accurately meters a volume of 10 μL (in vitro delivered dose; 95% confidence interval: 9.7–10.1 μL).
On the day of testing, 20 mg/mL sterile fluorescein was filled out in a sterile 1-mL glass syringe, which could be inserted into the device by routine sterile handling. The spray nozzle was sterilized before use, and the spray device was assembled with sterile operation gloves just before the mist application. These procedures were reviewed and approved by the Infection Prevention Committee of the Rotterdam Eye Hospital.
Autofluorescence in the cornea, AC, lens, and vitreous cavity was assessed with the Fluorotron Master II (Ocumetrics, Palo Alto, CA; www.ocumetrics.com/fm2.shtml). Measurements were performed before administration and at 1, 2, 5, 10, 20, 50, and 100 min thereafter. Sequences of autofluorescence measurements of each ocular compartment were corrected for the off-set level by subtracting the minimum value within each individual curve (ie, baseline usually).
Maximum autofluorescence signal (Smax), time of Smax (Tmax), and mean residence time (MRT) were calculated (R version 3.0.1). Area under the curve (AUC) was calculated from t=0 to t=100 min by means of a linear trapezoidal rule approximation. Terminal half-life (T1/2) was determined by linear regression analysis of the log-transformed data. A paired t-test was used to compare differences between both administration techniques.
Results
Both the 10 μL mist and the 50 μL drops were well tolerated by all subjects and no adverse reactions were observed. After the mist application, both the upper and lower eyelids were colored yellow by the fluorescein containing mist; the drop applications invariably led to a generous spill over the lower eyelid and cheek. In all 18 subjects, intraocular fluorescein measurements could be obtained for all time points (a single vitreous baseline measurement excepted). With regard to the increase of autofluorescence, particularly in the cornea (Fig. 2) and the AC (not shown), considerable variation between subjects was observed.
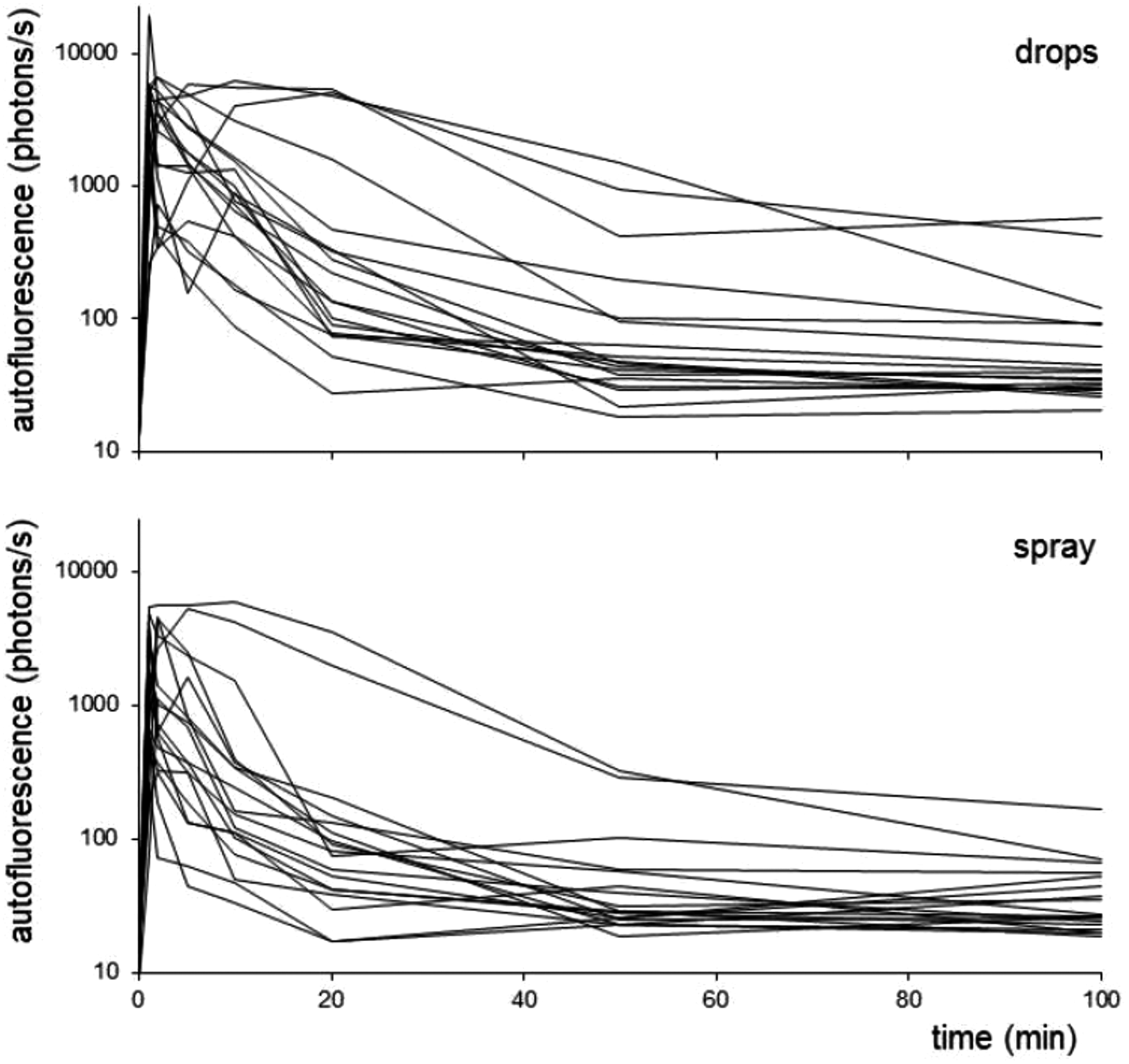
Autofluorescence (photons/s) versus time (min) in the cornea of individual participants after administration of a fluorescein drop (upper panel) and fluorescein spray (lower panel).
Figure 3 shows the mean autofluorescence level as a function of time for the cornea, the AC, and the lens. The corneal Smax (mean±SD) was 5,160±4,000 photons per second with drops administration versus 2,470±1,990 with spray (P=0.007); differences with respect to Tmax (3.1±4.8 vs. 2.2±2.3 min), T1/2 (58±47 vs. 55±29 min), and MRT (13.7±6.3 vs. 17.1±10.5 min) were not statistically significant. For the AC, merely AUCs were determined (see next paragraph) because the autofluorescence levels were still above baseline after 100 min. Initially, the autofluorescence level in the lens appears to decrease (Fig. 3). As this is supposed to be an artifact (see Discussion), these data were not used for further analysis. Autofluorescence in the vitreous at 100 min was 249±123 photons/s after drop application and 228±120 photons/s after mist application. These values did not significantly exceed baseline measurements: 230±140 and 218±130 photons/s, respectively.

Mean autofluorescence (photons/s) versus time (min) after 50 μL drop (♦) and 10 μL spray (■) applications in the cornea, the anterior chamber, and the lens. Upper dotted line: autofluorescence+standard error of the mean (SEM) after drop application; lower dotted line: autofluorescence−SEM after spray application.
For both eyes of all 18 participants, the AUCs were calculated. Results for the cornea and the AC are shown in Table 1. AUC (mean±SD) for the cornea was (363±431)×104 photons after drop application and (154±265)×104 photons after the mist (P=0.005). For the AC, these values were (6.9±10.3)×104 and (2.9±5.4)×104 photons, respectively (P=0.14). On average, the (drops/spray) AUC ratio was 4.1±3.4 for the cornea and 4.4±5.8 for the AC.
SD, standard deviation.
Discussion
To compare intraocular penetration of fluorescein, the autofluorescence (photons/s) versus time assessments were used to calculate the AUC, a method equivalent to AUC analysis of serum concentration versus time curves after (systemic) drug administration. As the correlation between the autofluorescence within subjects (cornea: R2=0.63) is rather strong, a substantial part of the variation appears to be associated with interindividual differences. The considerable interindividual autofluorescence variation we observed in the cornea (Fig. 2) and the AC (Table 1) has been reported before. 11 Although a strong correlation between subjects' age and fluorescein penetration of the AC has been reported previously, 12 our data do not appear to corroborate the existence of such a relationship.
On average, the AUC for the cornea was significantly higher after the administration of drops (P=0.005). A similar tendency, although not statistically significant (P=0.14), was observed in the AC. With both types of administration, the fluorescein will only partially reach the ocular surface; a substantial amount of the mist arrives at the upper and lower eyelid instead, and much of the drop is lost by spillover and lacrimal clearance. The exact volumes reaching the ocular surface have not been determined. Nevertheless, it can be conjectured that the differences in autofluorescence are, to some degree, due to the different volumes that were applied (10 and 50 μL, respectively). A simple comparison of the AUC/volume ratios of both the cornea (154/10 : 363/50) and the AC (2.9/10 : 6.9/50) suggests a 2-fold increase of the relative biological availability of the compound when delivered by the spray device.
A characterization of the pharmacokinetic properties of topical ocular fluorescein was not the objective of this study. However, it might be noticed that the initial decrease in the AC is succeeded by an increase of the autofluorescence level, whereas the autofluorescence curves in the cornea display a more or less exponential decrease.
In contrast with the cornea and the AC, the autofluorescence measurements in the lens initially show a decrease relative to baseline (Fig. 3). As this would seem a rather unrealistic result and may well reflect an artificial suppression caused by the high autofluorescence level in the more anterior ocular compartments, these data were not used for further analysis. After 20–50 min, however, the autofluorescence level in the lens does not appear to deviate from baseline. For logistical reasons, assessments for the vitreous cavity had to be limited to baseline and 100 min. Autofluorescence at 100 min did not exceed baseline levels.
This proof-of-principle study demonstrates the intraocular penetration of fluorescein when applied either as a drop or as a mist. We conclude that the application of fluorescein with the spray device yields substantial intraocular levels. Future studies with commonly used topical ocular drugs might be designed to investigate intraocular penetration of compounds administered before intraocular surgery. Together with aqueous and/or vitreous samples to assess the pharmacokinetic properties within the ocular compartments, serum samples could be acquired to investigate the systemic distribution of a compound when either route of administration, that is, mist or drop, is used. An alternative investigational approach to investigate systemic effects might be to examine pharmacodynamic parameters such as the mydriatic effect in the eye receiving the drug compared to the contralateral eye.
Footnotes
Acknowledgments
The authors would like to thank Bas van Hal, optometrist, for the subject recruitment and measurements, Bas Goulooze, Centre for Human Drug Research, Leiden, for his contribution to the pharmacokinetic analysis, Johan Egerström, SHL Group Sweden, for the prototype devices, and The Netherlands Enterprise Agency for the “Pieken in de Delta” grant (PID 102025), which has enabled this research project.
Author Disclosure Statement
J. van R. and R.J.W.: no competing financial interests exist. W.P.J. de K.: head of device development and co-owner Medspray BV.