
Abstract
Abstract
Purpose:
To compare the efficacy of intravitreal injection of triamcinolone acetonide (IVTA) for diabetic macular edema (DME) in vitrectomized eyes with DME without vitrectomy eyes.
Methods:
This retrospective comparative study evaluated the efficacy of IVTA treatment of DME in 26 consecutive eyes (23 patients). Changes in mean best-corrected visual acuity (VA) and mean central retinal thickness (CRT) were retrospectively evaluated before IVTA and during the 6-month period after IVTA.
Results:
Subjects were divided into 2 groups: 13 consecutive eyes (11 patients) with proliferative diabetic retinopathy or DME that underwent vitrectomy (vitrectomized group), and 13 consecutive eyes (12 patients) with DME who received IVTA, but did not undergo vitrectomy (nonvitrectomized group). In the vitrectomized group, there was a significantly decreased CRT for up to 4 months as compared to the thicknesses before IVTA. In the nonvitrectomized group, there was a significantly decreased CRT for up to 5 months after IVTA. In both groups, there was significant improvement in the VA for up to 4 months after IVTA.
Conclusion:
IVTA may represent a valid treatment option for DME, even in vitrectomized eyes.
Introduction
T
Macular edema (ME) sometimes persists or recurs in eyes after vitrectomy (vitrectomized eyes) with proliferative DR and DME. 9 The metabolic clearance of intravitreal drugs in vitrectomized eyes differs from that in eyes that have not undergone vitrectomy (nonvitrectomized eyes).10–17 In an experimental rabbit model, Chin et al. found that the half-life of TA was shorter in vitrectomized versus nonvitrectomized eyes. 11 Therefore, the therapeutic efficacy of IVTA in vitrectomized eyes may differ clinically from that in nonvitrectomized eyes. Beer et al. reported a shorter half-life of TA of 3.2 days in a patient who had undergone vitrectomy. 18 However, the clinical duration of the effect and safety of IVTA in vitrectomized eyes has rarely been reported, and when studied, only an insufficient number of patients have been evaluated. 17 Therefore, the aim of our current study was to evaluate the duration of the effect and the efficacy of IVTA for DME in vitrectomized eyes.
Methods
The protocol of this retrospective comparative study from 26 consecutive eyes (23 patients) with DME treated with IVTA was approved by the Ethics Committee of the Jikei University School of Medicine and complied with the tenets of the Declaration of Helsinki.
Fluorescein angiography showed that all enrolled patients exhibited diffuse fluorescein leakage for DR that involved most of the macular area. Measurements of the central retinal thickness (CRT) by optical coherence tomography (OCT) scans revealed a >300 μm thickness. Patients with recurrent or persistent DME underwent retreatment that was applied for at least 6 months after the original vitrectomy. Subsequent OCT showed that recurrent or residual macular edema was in excess of 300 μm.
Between January 2012 and November 2014 at the Tokyo Jikei University Hospital, 26 eyes of 23 subjects with DME were administered 4 mg of IVTA (MaQaid®; Wakamoto Pharmaceutical Co., Ltd., Tokyo, Japan) using a 27-gauge needle through the pars plana. Anterior chamber paracentesis was performed after IVTA to adjust the intraocular pressure (IOP) within normal limits.
Subsequently, we then divided the patients into 2 groups. The vitrectomized group consisted of 13 consecutive eyes (11 patients) with proliferative DR or DME who underwent a 25- or 23-gauge vitrectomy. The nonvitrectomized group consisted of 13 consecutive eyes (12 patients) with DME who received IVTA, but did not undergo vitrectomy.
During the 6-month follow-up period, changes in the mean VA and mean CRT were retrospectively evaluated before IVTA and during the 6-month period after IVTA. We additionally compared the changes in the VA and CRT after IVTA between the vitrectomized and the nonvitrectomized group. Spectral-domain OCT was performed using a Cirrus™ HD-OCT system (Carl Zeiss Meditec, Dublin, CA).
VA was measured using a 5-m Landolt chart. For data analysis, visual acuities were converted to logarithm of minimum angle of resolution (logMAR) for calculation.
Patients who received other treatment or had surgery within 6 months before or after IVTA were excluded.
Statistical analysis was performed using the software programmed by Hisae Yanai (Statcel-3; OMS Publication, Saitama, Japan) with Excel (Microsoft, Redmond, WA).
Paired t-test was used to compare the postoperative VA and CRT with the preoperative measurements in the vitrectomized group and the nonvitrectomized groups. The independent sample t-test was used for comparison of the vitrectomized group and the nonvitrectomized groups. Comparison of categorical data was performed with chi-square test. Values of P < 0.05 were considered statistically significant.
Results
The vitrectomized group, which consisted of 13 consecutive eyes (11 patients) with proliferative DR or DME that underwent 25- or 23-gauge vitrectomy at the Tokyo Jikei University Hospital, was treated with IVTA postoperatively for persistent or recurrent DME. This group included 7 men and 4 women with a mean age of 55.1 ± 7.9 years (range, 46–69 years). Before IVTA, the mean logMAR VA was 0.72 ± 0.27, whereas the mean CRT was 519.7 ± 188.0 μm. Mean time from the vitrectomy to IVTA was 22.3 months (range, 6–46 months). The main reason for vitrectomy was ME in 9 eyes (7 patients) and vitreous hemorrhage in 4 eyes (4 patients). In 2 of the ME eyes, the patients underwent internal limiting membrane (ILM) peeling.
The mean IOPs in the vitrectomized group were 13.9 ±3.5 mmHg before IVTA, 14.4 ± 3.7 mmHg at 1 month after IVTA, 15.0 ± 4.3 mmHg at 3 months after IVTA, and 13.2 ± 3.4 mmHg at 6 months after IVTA. No significant increases were seen for the IOPs at 1, 3, and 6 months after the IVTA when compared with the IOP before IVTA (P > 0.05, paired t-test). All eyes had an intraocular lens (IOL) implant (pseudophakic eyes) at the time of IVTA. Three eyes (3 patients) received IVTA for persistent ME after vitrectomy. Ten eyes (8 patients) showed improvement of ME after vitrectomy, but received IVTA because ME subsequently recurred.
In this group, the vitreous body remained in the periphery with the TA trapped by the residual vitreous body. In addition, the residual vitreous body also trapped the TA behind the lens capsule (Figs. 1 and 2).
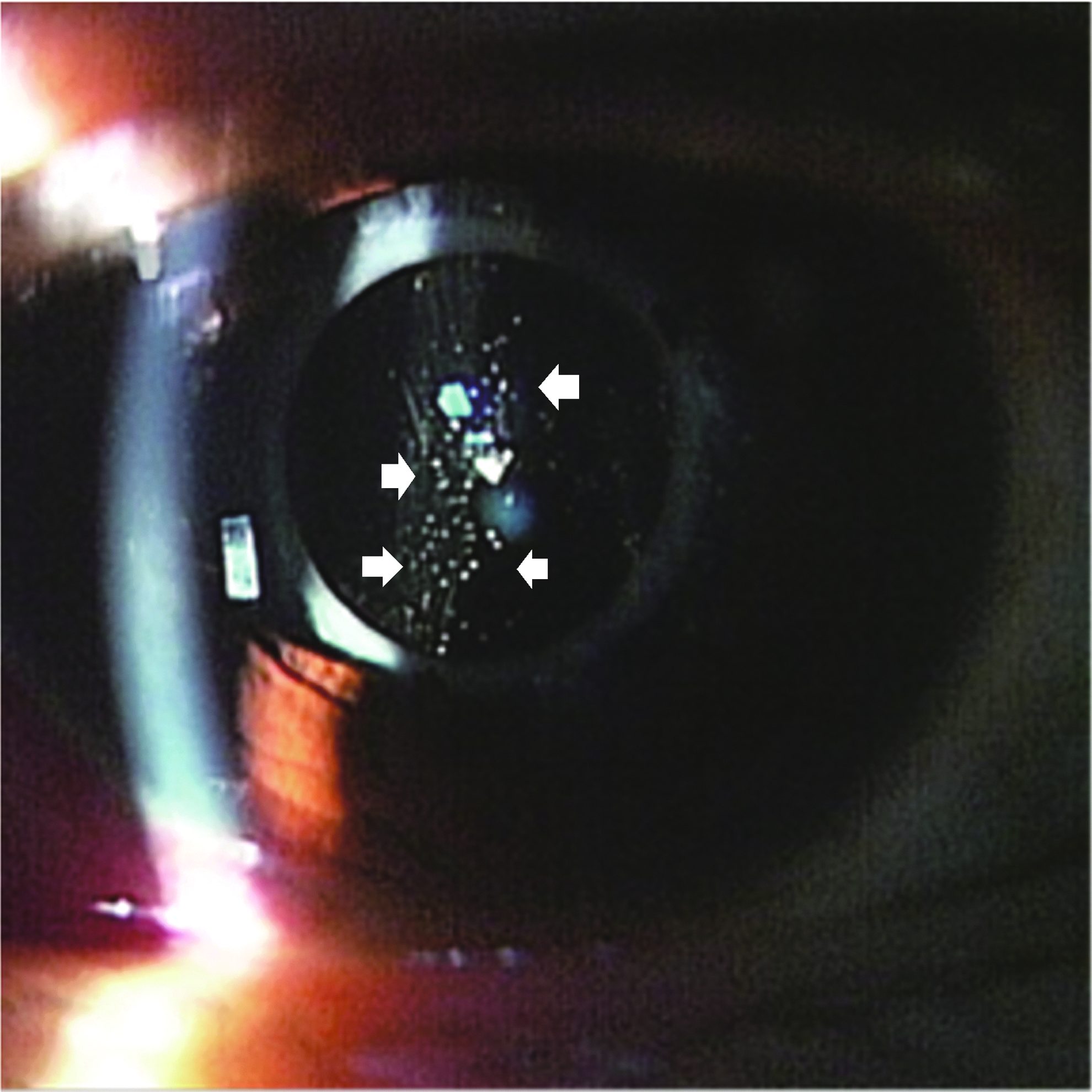
Slit lamp photography at 1 day after IVTA. Triamcinolone acetonide (TA; white arrows) was trapped behind the lens capsule by this residual vitreous body. IVTA, intravitreal injection of triamcinolone acetonide. Color images available online at www.liebertpub.com/jop
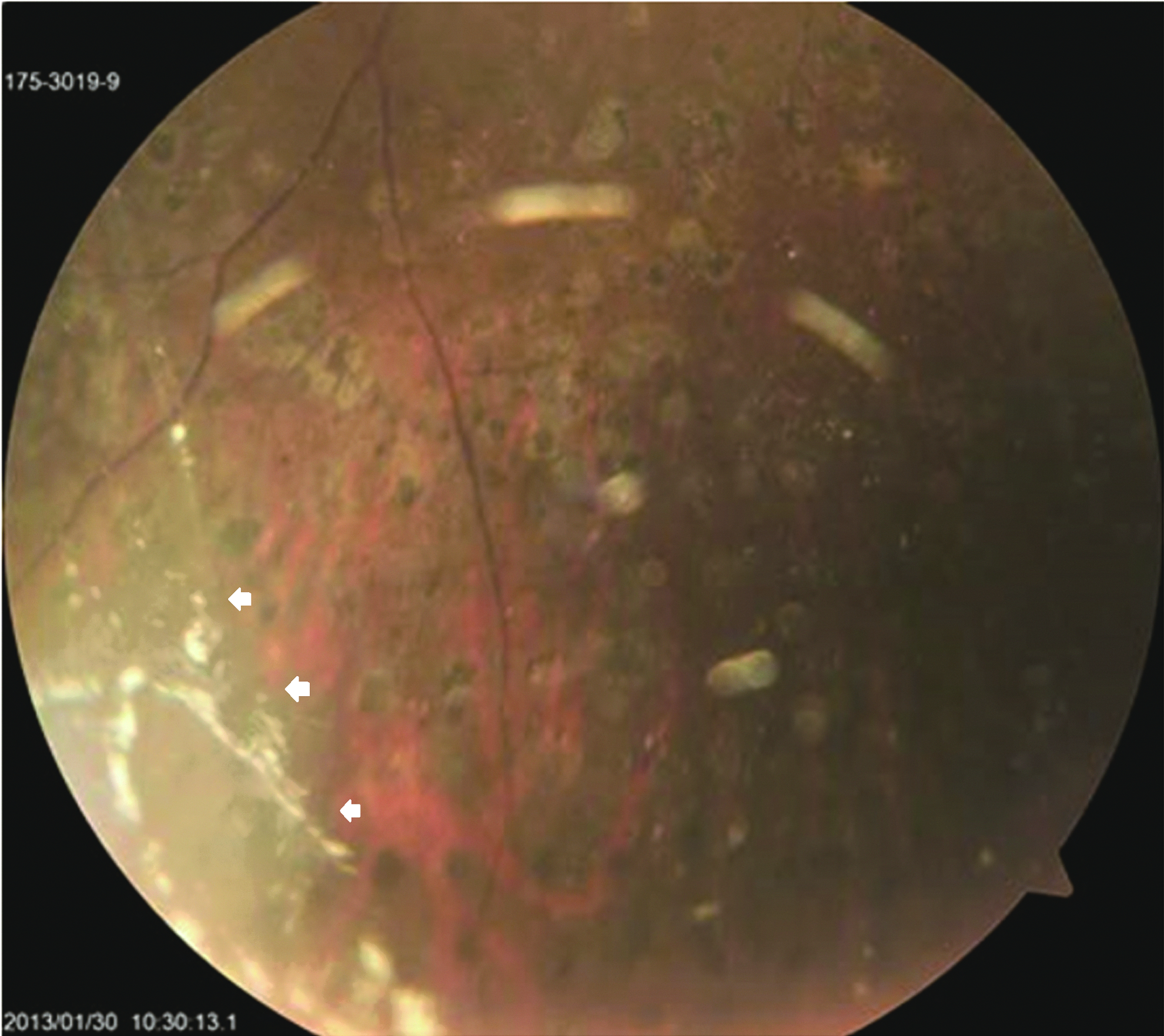
Fundus photography at 1 day after IVTA. Vitreous body remained in the periphery and TA (white arrows) was trapped by this residual vitreous body. Color images available online at www.liebertpub.com/jop
The nonvitrectomized group included 13 consecutive eyes (12 patients) with DME who received IVTA, but did not undergo vitrectomy. This group consisted of 7 men and 5 women with a mean age of 51.9 ± 10.3 years (range, 37–65 years). Before IVTA, mean logMAR VA was 0.46 ± 0.30, and mean CRT was 522.4 ± 137.3 μm. The mean IOPs in this group were 15.7 ± 2.3 mmHg before IVTA, 15.6 ± 2.9 mmHg at 1 month after IVTA, 16.9 ± 4.8 mmHg at 3 months after IVTA, and 16.4 ± 3.9 mmHg at 6 months after IVTA. No significant increases were seen for the IOPs at 1, 3, and 6 months after the IVTA when compared with the IOP before IVTA (P > 0.05, paired t-test).
Mean hemoglobin A1c (National Glycohemoglobin Standardization Program) was 6.2% ± 1.1% in the vitrectomized group and 7.4% ± 2.3% in the nonvitrectomized group (Table 1).
IVTA, intravitreal injection of triamcinolone acetonide; VA, visual acuity; CRT, mean central retinal thickness; HbA1c (NGSP), hemoglobin A1c (National Glycohemoglobin Standardization Program); IOP, intraocular pressure.
Figure 3 shows changes in mean CRT, and Fig. 4 shows changes in mean VA, in both groups. In the vitrectomized group, CRT was significantly decreased up to 4 months after IVTA as compared to before IVTA (P < 0.05, paired t-test) In the nonvitrectomized group, CRT was significantly decreased up to 5 months after vitrectomy as compared to before IVTA (P < 0.05, paired t-test). In both groups, CRT at 6 months after IVTA had returned to baseline levels. Mean CRT at 2 months after IVTA was 283 μm in the vitrectomized group and 332 μm in the nonvitrectomized group. In both groups, mean CRT was lowest at 1 month after IVTA.
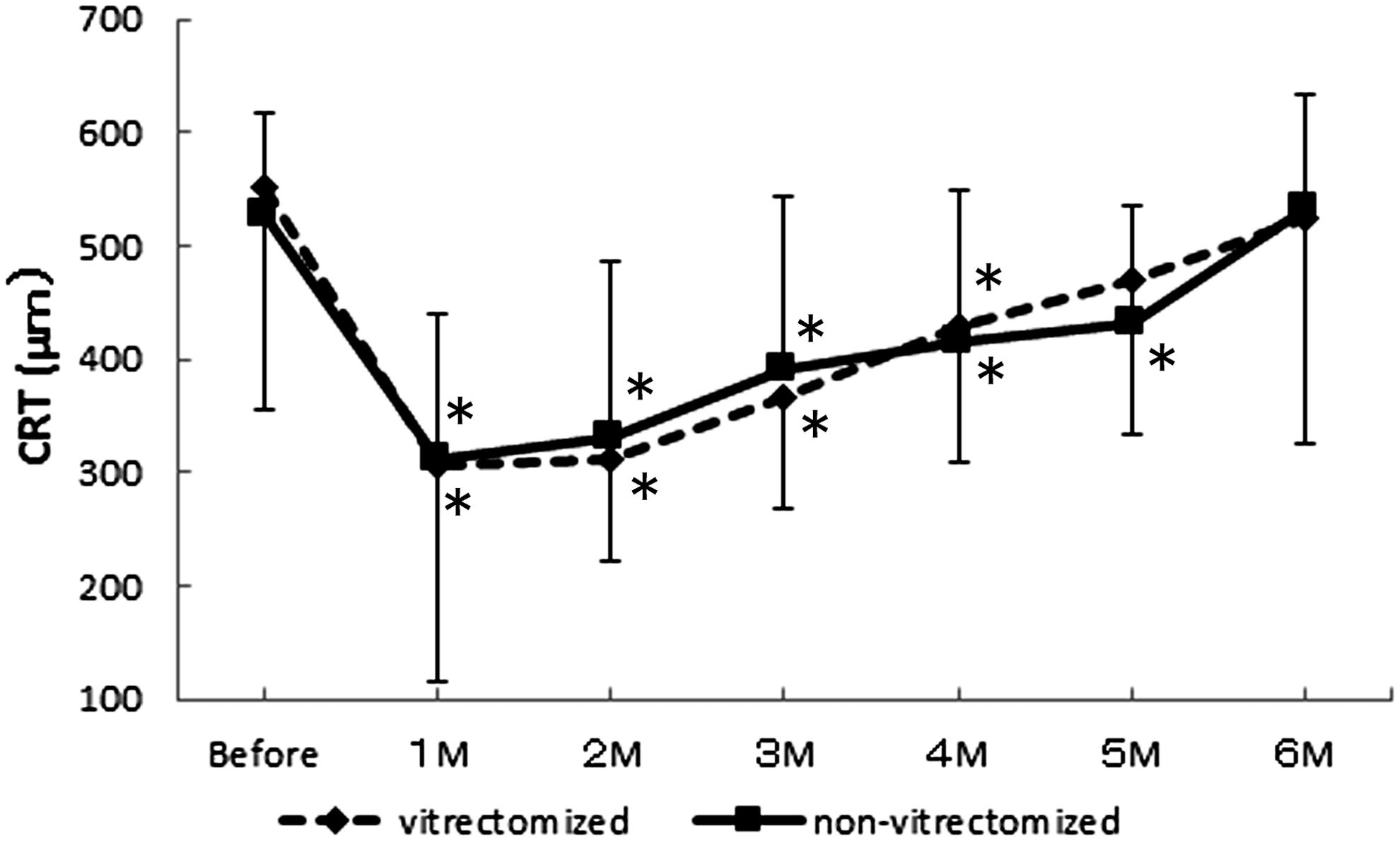
Changes in mean central retinal thickness (CRT). In the vitrectomized group, CRT was significantly decreased up to 4 months after IVTA as compared to before IVTA (*P < 0.05, paired t-test). In the nonvitrectomized group, CRT was significantly decreased up to 5 months after vitrectomy as compared to before IVTA (*P < 0.05, paired t-test). No significant differences were apparent for the mean CRT at any time of the measurement between the 2 groups.
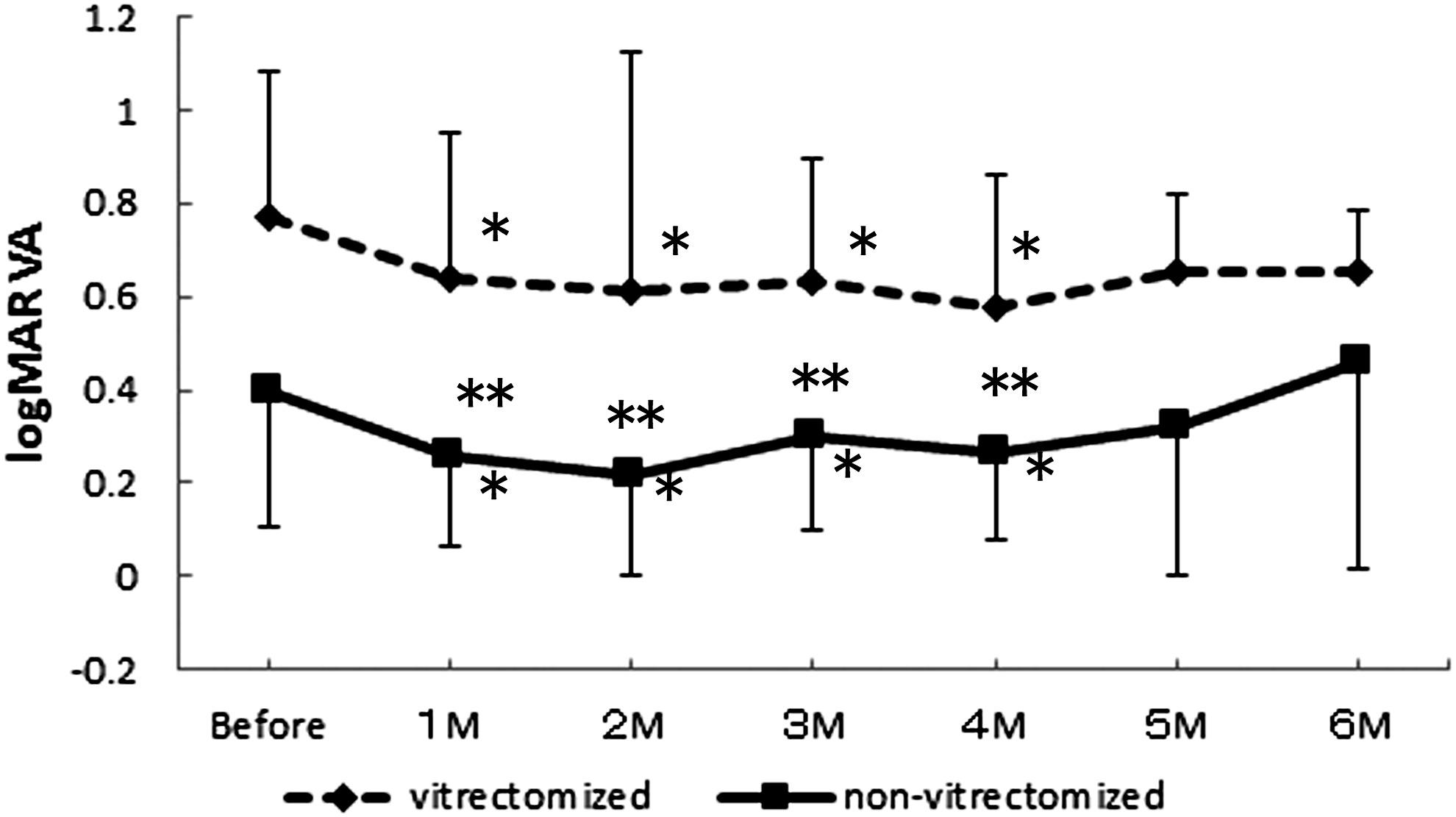
Changes in mean logMAR visual acuity (VA). In both vitrectomized and nonvitrectomized group, VA during the first month after IVTA was improved compared to before IVTA, and remained significantly improved up to 4 months after IVTA (*P < 0.05, paired t-test). At 1, 2, 3, and 4 months after the IVTA, the mean VA in the non-vitrectomized group were significantly better than the mean VA in the vitrectomized group (**P < 0.05, t-test).
In the vitrectomized group, VA during the first month after IVTA was improved compared to before IVTA, and remained significantly improved up to 4 months after IVTA (P < 0.05, paired t-test).
There were also no apparent significant differences for the CRT for any of the measurements between the 2 groups.
At 1, 2, 3, and 4 months after the IVTA, there was a significantly better mean VA compared to the preoperative mean VA (P < 0.05, paired t-test).
In the vitrectomized group, the elevated IOP did not occur until after IVTA. In the nonvitrectomized group, there was a similar improvement of the VA during the first month after IVTA when compared to the acuities before IVTA.
A temporary increase in the IOP (26 mmHg) was observed in 1 eye in the nonvitrectomized group. Topical antiglaucoma drugs were used to control the IOP in this patient during this period. No endophthalmitis was encountered in either group during the 6-month follow-up period.
Representative case
A 46-year-old woman in the vitrectomized group showed a baseline VA of 0.1 (logMAR 1.0) in the left eye. Because of ME and vitreous hemorrhage, which were associated with proliferative DR, she underwent lens phacoemulsification, IOL implantation, and vitrectomy. During vitrectomy, the vitreous body, which was cloudy due to hemorrhage, was excised. Posterior vitreous detachment was created, and laser photocoagulation of the peripheral retina was additionally performed. The ILM was not peeled.
The patient was treated with IVTA because of persistent ME at 7 months postoperatively. Before IVTA, CRT was 886 μm and VA was 0.1 (logMAR 1.0). After IVTA, intraretinal spongiform retinal edema and serous retinal detachment disappeared. At 3 months after IVTA, intraretinal edema recurred. Although no serous retinal detachment was present at 6 months after IVTA, intraretinal spongiform edema returned to almost the same degree as before IVTA (Fig. 5).

Spectral-domain optical coherence tomography images of before and after IVTA.
Discussion
Presently, there is an increasing use of intravitreal injection of steroids or anti-VEGF drugs for age-related macular degeneration and DME. Intravitreal drugs dissolve in the vitreous fluid and are excreted through aqueous humor drainage during the replacement of the vitreous fluid. However, little is known about the detailed pharmacokinetics for these drugs. It is likely that the pharmacokinetics of intravitreal drugs in eyes that have undergone lensectomy or vitrectomy are probably not that different from eyes that did not undergo the procedure.10–18 A previous animal study reported that there was a faster clearance of TA in eyes that underwent vitrectomy versus those that did not.11,12 Thus, the clinical effectiveness and duration of the effects of intravitreal drugs in eyes may differ between vitrectomized and nonvitrectomized eyes.
The pharmacokinetics of IVTA used clinically in vitrectomized eyes has not been reported in detail. In 6 patients who underwent vitrectomy after receiving 4 mg of IVTA, Mason et al. measured vitreous and aqueous concentrations of TA at the time of vitrectomy. In cases where TA was measured 1.25–2.75 months after IVTA, TA was detectable in the vitreous body and aqueous humor. However, in cases where TA was measured ≥ 3 months after IVTA, TA was not detectable. 14 In the present study, the clinical effectiveness of IVTA was assessed by measuring CRT and VA. Mean CRT in 13 eyes (11 patients) who had undergone vitrectomy and cataract surgery was the thinnest at 1 month after IVTA, then mean CRT increased at ≥ 2 months after IVTA. In the study by Mason et al., 14 TA was not detectable in the vitreous body of vitrectomized eyes at ≥3 months after IVTA. Likewise, in the present study, the increase in CRT was probably due to the elimination of TA from the vitreous body. In 13 nonvitrectomized eyes, mean CRT was also the thinnest at 1 month after IVTA. The time of peak effect was thus similar to that of the vitrectomized group. Because TA is a corticosteroid suspension and is practically insoluble in water, particles of TA are trapped in the vitreous body. Even after vitrectomy, vitreous body remains in the periphery and behind the lens capsule, and TA is trapped by this residual vitreous body (Figs. 1 and 2). This trapping of TA in residual vitreous body may account for the absence of differences in pharmacokinetics and the same time of peak effect for IVTA in both vitrectomized and nonvitrectomized eyes.
In addition to the use of pharmacotherapy with steroids for ME, anti-VEGF drug treatments have recently become more common. It has also been reported that in previously phakic vitrectomized eyes, there is a short-term improvement in the best-corrected VA and the central macular thickness after intravitreal ranibizumab for DME. 19 However, since it has been found that another anti-VEGF drug, bevacizumab, has a high clearance in vitrectomized eyes, both the effectiveness of the drugs may be lower and the duration of the effect may be shorter.10,16,19 Thus, the overall clinical effectiveness of these drugs may be limited. On the other hand, even though the duration of the effect of IVTA was 1 month shorter in the vitrectomized versus the nonvitrectomized eyes in our study, there was improvement of the CRT compared to the baseline that remained for up to 4 months after IVTA. In addition, the duration of the improved VA was similar between the vitrectomized and nonvitrectomized groups. Thus, IVTA treatments may be more appropriate for clinical treatments of DME in vitrectomized eyes as compared to the anti-VEGF drugs.
In several studies of high-dose IVTA (20-mg dose), the median residence time of TA in the eyes was longer than that of 4 mg IVTA.17,20,21 In our study, the reduction in CRT after IVTA lasted for 4 months. Whether a 20-mg dose would be more effective in maintaining CRT and improved VA is unclear. Further studies are necessary to evaluate therapeutic efficacy with different doses of TA.
IVTA for DME has previously been reported as effective, 22 but complications due to the pharmacological actions of TA can present a problem when used clinically. These complications of IVTA include cataracts, elevated IOP, 22 vitreous hemorrhage, endophthalmitis, and retinal detachment. 23
Lens phacoemulsification and IOL implantation are often performed at the same time during vitrectomy, and in the vitrectomized eyes that received IVTA in our study, lens phacoemulsification and IOL implantation were performed in all cases. Therefore, there was no need to consider complications related to cataract progression with IVTA. In the nonvitrectomized group, 6 months of follow-up observation after a single dose of IVTA, in our study, showed no obvious cataract progression in any patient. However, cataract progression leading to decreased VA has been reported with repeated IVTA.22,23 Careful monitoring for cataract progression is thus essential with repeated treatment in phakic eyes.
Elevated IOP is a potential complication with IVTA. A 20% rate of elevated IOP in patients who have received IVTA has been reported. 24 In the vitrectomized group, 8 of 11 patients had a history of a sub-Tenon's capsule injection of TA for DME. None of these 8 patients had a history of elevated IOP due to sub-Tenon's capsule injection of TA. All patients in the vitrectomized group used dexamethasone sodium phosphate eye drops for ∼4 weeks after vitrectomy. However, none of these patients had elevated IOP suggestive of being a steroid responder. Patients with DR often receive steroid treatment preoperatively, enabling prediction of whether a steroid response will occur based on findings at that time. In our study, elevated IOP did not occur after IVTA in the vitrectomized group. Because our study was retrospective in nature, patients with elevated IOP due to a history of steroid treatment did not receive IVTA. If treatment with IVTA is limited to patients without a history of elevated IOP due to steroid eye drops or sub-Tenon's capsule injection of TA, the risk of elevated IOP can be reduced.
Infections and retinal detachment have also been reported as complications of IVTA. 23 Retinal detachment after IVTA can be caused by vitreal traction due to vitreous incarceration where the needle enters the vitreous body, but if the peripheral vitreous body is adequately treated during vitrectomy, the incidence of retinal detachment is predicted to be low.
With IVTA in nonvitrectomized eyes, particles of TA, which is used as a corticosteroid suspension, are trapped in the vitreous body. The injected TA appears as white particles, so with injection in the center of the vitreous cavity, patients may complain of blurred vision (Fig. 6). In vitrectomized eyes, only the peripheral vitreous body remains, so TA particles are not trapped in the center of the vitreous cavity, and patients do not experience such symptoms.

Fundus photography at 1 day after IVTA in nonvitrectomized eyes. The injected TA appears as white particles, so with injection in the center of the vitreous cavity, patients may complain of blurred vision. Color images available online at www.liebertpub.com/jop
Given these mechanisms, the rates of adverse reactions due to the pharmacological action of TA and complications due to IVTA are expected to be lower in vitrectomized eyes. In our study, none of the patients in either group showed adverse reactions or severe complications. Future comparative studies to evaluate the incidence of complications in a larger number of patients are needed. Further comparative studies are necessary to evaluate therapeutic efficacy of the sustained dexamethasone implant therapy and IVTA.
Although repeated IVTA every 4 months seems necessary for sustained improvement in ME,14,25 the incidence of adverse reactions and complications associated with IVTA is expected to be even lower than that in nonvitrectomized eyes. IVTA may, therefore, represent an option for clinical treatment of ME even in vitrectomized eyes.
Chan et al. reported that a repeat injection of 4 mg of IVTA appeared not to be as effective as the initial injection for the treatment of DME. 25 However, it is possible that repeat IVTA could increase complications such as cataract. 24 Therefore, if a repeat injection is required in a patient, we may need to confirm the effectiveness of combined therapy with IVTA and subthreshold laser treatment or ILM peeling.26,27
The limitations of our current study include the fact that it was a retrospective study that only examined a small number of patients. In addition, there was only a fairly short follow-up period for this study. Thus, further randomized control studies with longer follow-up periods will need to be undertaken to confirm the effectiveness of IVTA as compared to other currently available treatments.
Footnotes
Author Disclosure Statement
No competing financial interests exist.