
Abstract
Abstract
Purpose:
Polyethylene glycol (PEG)-400 is a clear, colorless viscous liquid that readily dissolves many hydrophobic drugs. It is a widely used commercial solvent and vehicle for many pharmaceutical and cosmetic products. The purpose of this study is to investigate the intravitreal safety of PEG-400 to determine its suitability as a potential vehicle for intraocular drug delivery.
Methods:
Six healthy, male, Dutch Belted rabbits, weighing between 2.0 and 3.0 kg, were used for this experiment. The left eye of each animal received a single 0.1 mL intravitreal injection of PEG-400. Complete eye exams and dark- and light-adapted electroretinograms (ERG) were obtained at baseline and at 1 and 4 weeks after injection. After the 4-week ERG was completed, animals were euthanized, eyes were enucleated, and histology and transmission electron microscopy (TEM) were performed.
Results:
Ophthalmic examinations demonstrated diffuse signs of retinal degeneration and cataract formation in all 6 eyes injected with PEG-400, which was apparent at 1 week, but more evident by 4 weeks. Photopic and scotopic ERG studies demonstrated significant reduction in amplitudes at 1 and 4 weeks after injection compared to baseline. Histopathological and TEM analysis of eyes demonstrated both inner and outer retinal atrophy.
Conclusion:
Intravitreal injection of PEG-400 resulted in severe ocular toxicity.
Introduction
P
Because of its unique properties, PEG-400 may be a useful vehicle for sustained intraocular delivery of specific drug classes. Previous experimental studies have reported choroidal neovascularization, degeneration of retinal pigment epithelial cell, and reduction of photoreceptors after subretinal injection of PEG-400, but to our knowledge, there have been no published studies assessing its safety after intravitreal injection, which is more clinically relevant.3,4 Therefore, the purpose of this study is to investigate the intraocular safety of PEG-400 to determine its suitability as a potential vehicle for intravitreal drug delivery.
Methods
Animals
The Vanderbilt University Institutional Animal Care and Use Committee approved this investigation and the study adhered to the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research. Six healthy, male, Dutch Belted rabbits, weighing between 2.0 and 3.0 kg, were used for this experiment. They were housed in separate cages and maintained in a controlled environment. Food and water were administered ad libitum. Dutch Belted rabbits were chosen because of their increased pigmentation, which would facilitate observation of retinal pigment epithelium (RPE) atrophy.
Examinations
Eyes underwent baseline slit-lamp biomicroscopy, indirect ophthalmoscopy, and intraocular pressure measurement along with dark- and light-adapted electroretinogram (ERG) testing. Complete eye exams were repeated immediately after injection and again at 1 and 4 weeks postinjection. Indirect fundus photography was performed at each examination.
Experimental procedures
The left eye of each animal received a single 0.1 mL intravitreal injection of PEG-400 (Sigma-Aldrich, St. Louis, MO) that was filtered through a 0.22-μm Millipore filter (Sigma-Aldrich). The osmolarity of PEG-400 is 2.82 Osm/L. Animals were anesthetized with 1 mL mixture of equal parts xylazine hydrochloride (20 mg/mL) and ketamine hydrochloride (100 mg/mL) intramuscularly. Proparacaine (0.5%) was applied for corneal anesthesia. Pupils were dilated with topical tropicamide (0.5%), phenylephrine (2.5%), and atropine sulfate (1%). After application of 5% povidone-iodine solution, prophylactic removal of 0.1 mL anterior chamber fluid was performed. Immediately afterward, a 25-gauge needle on a tuberculin syringe was inserted 2 mm posterior to the limbus, directed toward the mid-vitreous, and 0.1 mL of PEG-400 was slowly injected under direct observation. Intraocular pressure afterward was less than 30 mmHg in all eyes and there was no evidence of accidental lens trauma. Topical moxifloxacin 0.5% and bacitracin were applied after the injection to prevent infection.
Electrophysiology
Standard scotopic and photopic ERGs were obtained by trained personnel following adequate anesthesia and pupillary dilation. Animals were dark adapted for 1 h before scotopic testing. The active electrode was positioned on the cornea. The reference and ground electrodes were placed subcutaneously in the ipsilateral pinna and left leg, respectively. Subsequent light-adapted ERGs were recorded on a continuous light-adapting white background of 30 cd/m2 after a 10-min period of light adaption. Scotopic and photopic a- and b-wave amplitudes were recorded. a-Wave amplitudes were measured from the preresponse baseline to the trough of the negative wave. b-Wave amplitudes were measured from the trough of the a-wave to the peak of the b-wave. For oscillatory potentials of the 30-Hz flicker response, the amplitude was measured from the preresponse baseline to the peak.
Histology
After the 4-week ERG was completed, animals were euthanized with intracardiac pentobarbital 200 mg. All eyes were enucleated and fixed in 10% formalin for 24 h. Gross examination was performed in conjunction with histology and transmission electron microscopy (TEM). Representative sections of the optic nerve head, medullary ray, and inferior retina (region of dependency where the drug would likely settle) were paraffin embedded. Semithin sections were stained with hematoxylin–eosin (H&E) and periodic acid-Schiff for light microscopy.
Statistics
Mean ERG a- and b-wave amplitudes (μV) were calculated for all examinations performed along with standard error. Statistical comparison was performed with paired t-test in Microsoft Excel (Microsoft Corporation, Redmond, WA). All statistical analysis was 2-sided with a 95% confidence interval used to gauge statistical significance. P values less than 0.05 were considered to be of statistical significance. Figures were made using GraphPad Prism 6.0 Software (Graphpad Software, La Jolla, CA).
Results
Clinical observations
All animals tolerated the injections well without external signs of inflammation. Slit-lamp and fundoscopic exam directly after injection and at subsequent time points did not reveal any unusual redness, purulent discharge, cellular response, or media opacity. Animals appeared comfortable and did not display any distressed behaviors suggesting pain or photophobia. Indirect ophthalmoscopic exams of PEG-400-injected eyes demonstrated widespread areas of retinal degeneration. This finding was first observed 1 week postinjection and became more pronounced at subsequent time points. In addition, there were areas of RPE atrophy with associated retinal detachment in areas of thinning and degeneration (Fig. 1). These findings were consistently present in all 6 eyes injected with PEG-400. In addition, PEG-400-treated eyes underwent rapid cataract formation, which was apparent as early as 1 week, but more evident by 4 weeks postinjection (Fig. 2). There were no significant IOP changes observed.
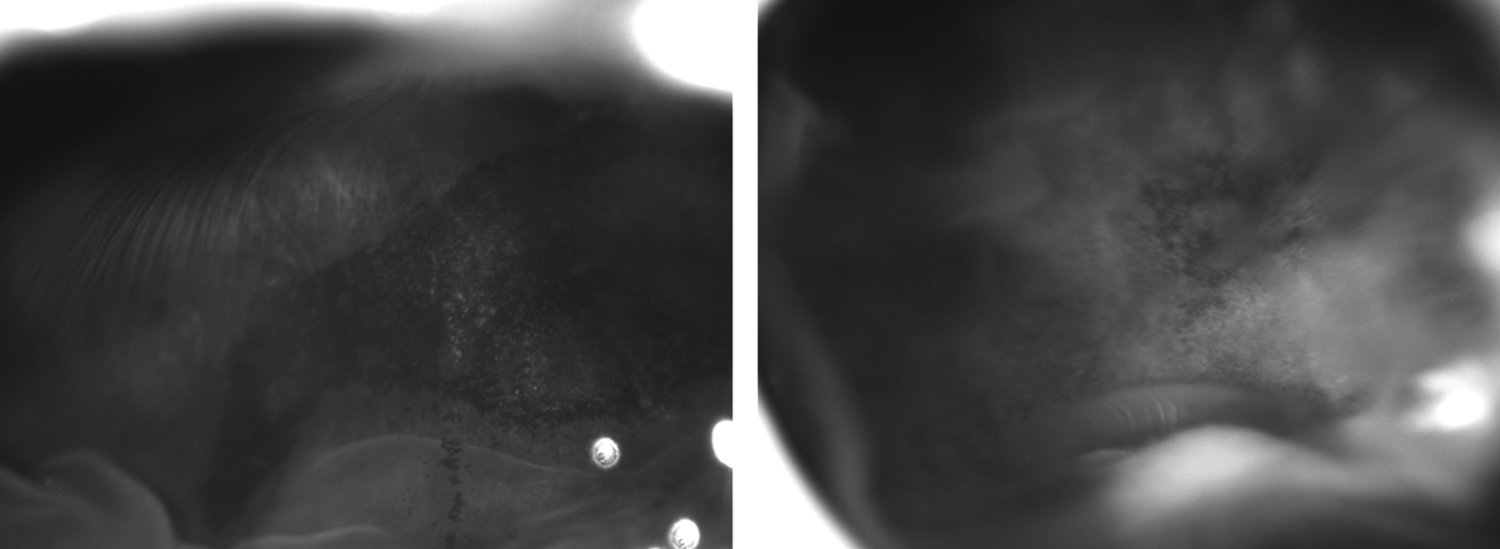
Representative fundus images demonstrating widespread areas of retinal atrophy, pigment changes, and associated areas of retinal detachment.
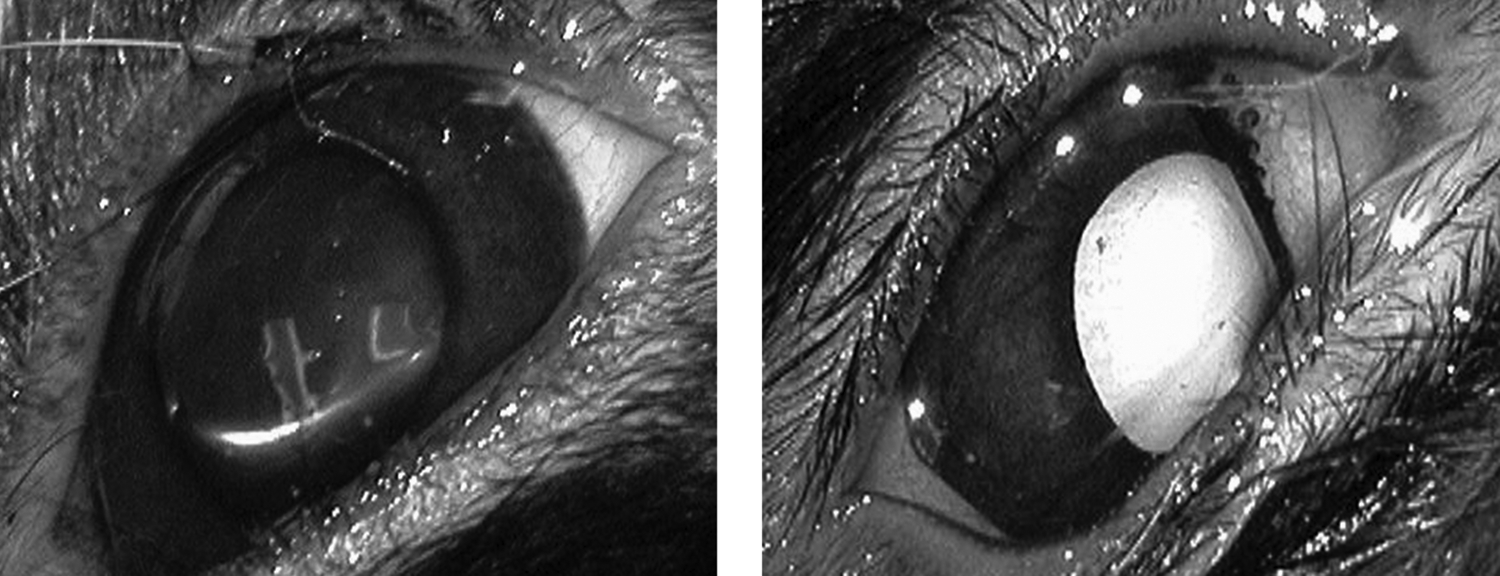
Representative external images taken the same day after injection of 0.1 mL polyethylene glycol (PEG)-400 (left) and at 4 weeks (right) demonstrating a particularly severe case of cataract formation.
ERG waveform
Representative 1- and 4-week ERG waveforms are shown in Fig. 3. All PEG-400-injected eyes showed similar ERG waveform reductions. There was significant reduction in b-wave amplitudes at 1 and 4 weeks. There was a similar significant decrease in a-wave amplitudes at 1 and 4 weeks when compared to baseline (Table 1).
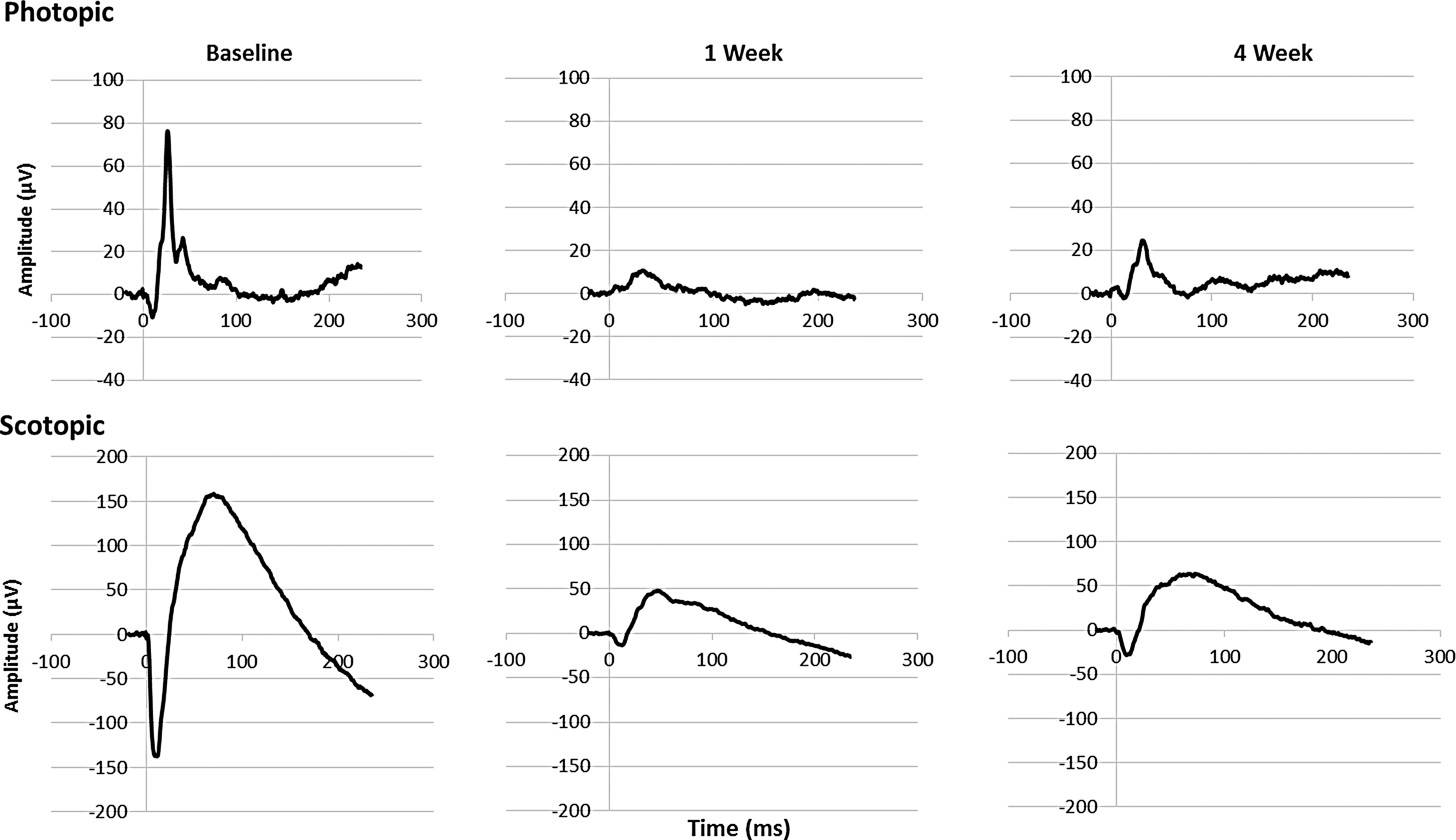
Representative photopic (above) and scotopic (below) electroretinogram (ERG) waveforms following a single 0.1 mL intravitreal injection of PEG-400. Large reduction in amplitudes at 1 week postinjection, which was sustained at 4 weeks postinjection.
P < 0.001 compared to baseline.
P < 0.05 compared to baseline.
Mean a-wave (photoreceptor) amplitudes decreased significantly from baseline. Under scotopic testing, the a-wave decreased from a mean of −141 ± 9 μV at baseline to −9.6 ± 5 μV after 1 week (P < 0.001) and remained depressed at 4 weeks with a scotopic a-wave of −28.6 ± 8 μV (P < 0.001). Under photopic testing conditions, the a-wave decreased similarly in comparison to baseline, although the changes were not as dramatic (Table 1).
Mean b-wave (bipolar and Muller cells) amplitudes were also significantly reduced in PEG-400-injected eyes. Scotopic b-wave amplitudes decreased from 305 ± 33 μV at baseline to 64.4 ± 31 μV (P < 0.001) 1 week postinjection and remained significantly depressed at 4 weeks postinjection (P < 0.001). Photopic b-wave amplitude reductions were also significantly reduced from 90.1 ± 5 μV at baseline to 17 ± 8 μV at 1 week (P < 0.001) and 36.2 ± 6 μV after 4 weeks (P < 0.001). Representative waveforms are shown in Fig. 3.
Histology
Light microscopy demonstrated the absence of intraocular inflammation in sectioned eyes. Cataract formation was clearly present. Tissue degeneration with widespread disorganization of the normal retinal histology with loss of normal cellularity was observed. There was inner and outer retinal atrophy with geographic areas of retinal degeneration (Fig. 4). Tissue electron microscopy demonstrates similar loss of normal retinal anatomy with extensive vacuolization and disorganization of photoreceptor inner and outer segments (Fig. 5).
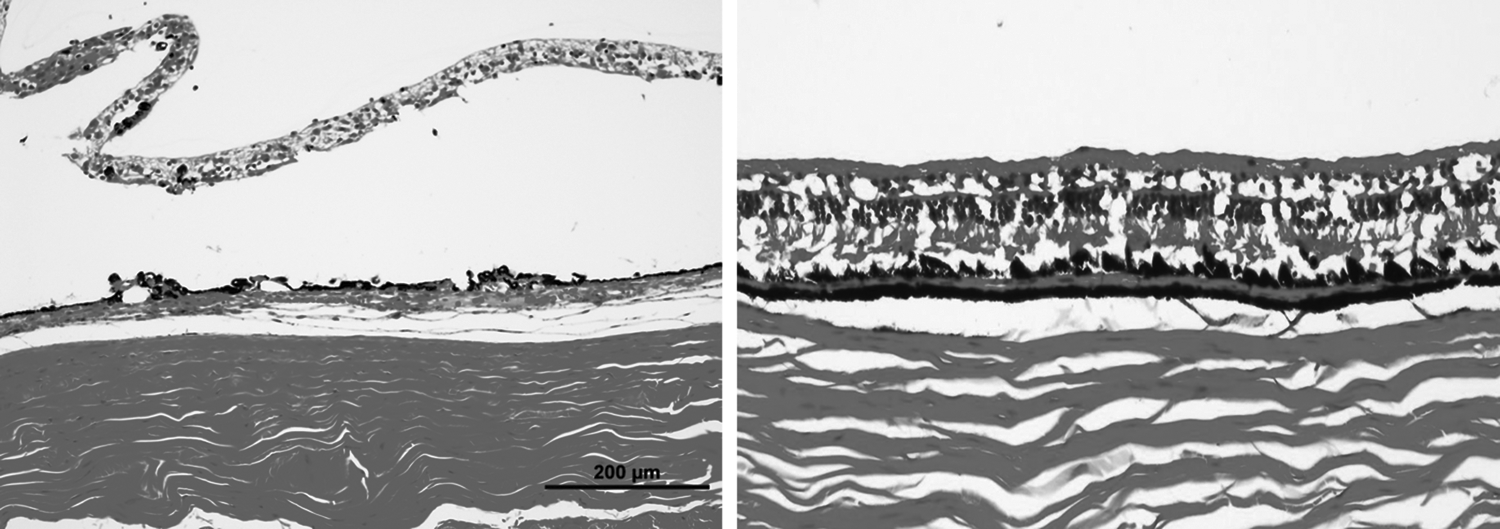
Representative histological sections of the retina following PEG-400 injection demonstrating focal areas of retinal necrosis (left) and diffuse areas of atrophy with loss of normal cellularity (right).

Representative transmission electron microscopy images of the retina after PEG-400 injection. Extensive vacuolization (asterisk) with disorganization of normal photoreceptor inner and outer segments.
Discussion
To our knowledge, this is the first study to investigate the intravitreal safety of PEG-400. Despite the general acceptance that PEG-400 has a superior safety profile in humans, 5 our results demonstrate that its intravitreal injection may cause severe ocular toxicity and therefore raises caution regarding its intraocular application. These findings are particularly noteworthy and timely since a recent human pilot study utilized PEG-400 as a vehicle for intravitreal injection of sirolimus 6 and PEG-based hydrogels are increasingly being studied for the express purpose of sustained intraocular drug delivery.7,8
PEG-400 is a clear, colorless viscous liquid that readily dissolves many hydrophobic drugs and, consequently, is often formulated alongside active ingredients of medications to facilitate drug absorption. Considering its favorable characteristics as a solubilizing agent, several studies have utilized PEG-400 as a vehicle for injectable medications. 1 Nguyen et al. recently investigated the ocular tolerability and efficacy of subconjunctival and intravitreal sirolimus packaged with PEG-400. 6 Subconjunctival application was associated with ocular pain and localized tenderness and hyperemia in 10% of injected patients that peaked at 2 weeks after injection and resolved by 4 weeks. After intravitreal injection, one study eye experienced rapid progression of cataract associated with loss of ≥6 Early Treatment Diabetic Retinopathy Study (ETDRS) lines of vision and a second study eye similarly lost ≥6 ETDRS lines of vision and required combined cataract extraction and glaucoma surgery.
Sirolimus is widely used as an oral formulation (Rapammune©; Wyeth Phramaceuticals, Collegeville, PA) for immunosuppression. The manufacturer of a proprietary formulation of sirolimus for intravitreal injection (MacuSight, Inc., Union City, CA) completed several ocular toxicity trials in the rabbit model with no observed toxicity. Based on these animal studies, Dugel et al. conducted a phase 1 clinical trial evaluating the safety and tolerability of a single intravitreal injection of sirolimus in human participants with diabetic macular edema and reported no serious ocular adverse events. 9
Although the results by Dugel et al. contrast those reported by Nguyen et al., the formulation of sirolimus injected in each study was provided by different manufacturers. Dugel et al. used a formulation provided by MacuSight, Inc., while Nguyen et al. used a formulation provided by Santen Pharmaceuticals, Osaka, Japan. While no information is provided on the exact composition of MacuSight's formulation, the Santen formulation contained PEG-400. Intravitreal injection of PEG-400 in our in vivo study resulted in rapid cataract progression in all 6 rabbit eyes that was apparent as early as 1 week, but clearly evident by 4 weeks, and may explain the rapid cataract formation observed by Nguyen et al. in some study eyes, in the absence of other plausible explanations.
In addition to cataract formation, we also observed widespread retinal toxicity after intravitreal injection of PEG-400. In direct support of our observation, Lyzogubov et al. previously reported that subretinal injection of PEG-400 in a mouse model resulted in caspase-dependent apoptosis of photoreceptors and subsequent reduction in outer nuclear layer thickness and density of cells. 3 Widespread degeneration of the RPE was also observed, which was postulated to be due to PEG activation of the complement system with consequent autophagy. Consistent with these reported findings, we observed diffuse inner and outer retinal atrophy and degeneration in a rabbit model after intravitreal injection of 0.1 mL of PEG-400, which was confirmed by both histopathology and functional testing with electrophysiology. Moreover, these changes were dramatic, proximate, and consistently seen in all eyes injected.
PEG is a polymer made up of identical ethylene glycol subunits and is oxidized by alcohol dehydrogenase (present in retinal cells) to several active metabolites.10,11 One of these metabolites is oxalic acid, which may combine with ionized calcium to form calcium oxalate.12,13 Oral application of ethylene glycol in rabbits resulted in reduced photopic and scotopic electrophysiological activity and histological changes in rabbit retinas. 14 Crystalline deposits were found predominately in the ganglion cell layer and inner nuclear cell layer of the retina, which were associated with deposition of calcium oxalate crystals in systemic organs. Furthermore, calcium oxalate crystals have been shown to cause acute inflammation-mediated necrotic cell death on other organ systems. 15
Taken together, we hypothesize that intravitreal injection of PEG-400 is metabolized to oxalic acid by retinal alcohol dehydrogenase, which then subsequently binds to calcium in the vitreous to form calcium oxalate. Subsequent deposition of calcium oxalate in retinal cells results in necrotic cell death and degeneration.
As with all experimental studies, our results should be interpreted with caution. The overall number of animal eyes injected was small and we did not perform dose escalation. We can therefore not rule out the possibility that smaller amounts may be nontoxic and potentially safely applied clinically. We also cannot rule out that an increase in vitreous osmolarity after PEG-400 injection may have contributed to toxicity in some way and a smaller injected volume may be less toxic or safe. Despite these obvious shortcomings, performance of both electrophysiology (baseline, 1-week, and 4-week) and histopathology testing, including TEM, strengthens a causal association. Equally important, 0.1 mL was studied (and not other volumes) because it is a typical volume that would be intravitreally injected in patients and therefore bestows direct clinical relevance to our study.
In conclusion, our results suggest that intravitreal injection of PEG-400 is associated with severe ocular toxicity. To our knowledge, we are the first to report this finding, which has direct clinical implications since the application of PEG-400 as a vehicle for intraocular drug delivery has garnered recent interest and momentum.6,8 Substantiation of our results by other independent groups will provide even greater confidence in these conclusions.
Footnotes
Acknowledgments
This work was supported by an unrestricted grant from Research to Prevent Blindness to Vanderbilt University School of Medicine, Department of Ophthalmology and Visual Sciences.
Author Disclosure Statement
No competing financial interests exist.