
Abstract
Abstract
Purpose:
To investigate a clinical outcome after more than 4 years for polypoidal choroidal vasculopathy (PCV) treated with anti-vascular endothelial growth factor (VEGF) therapy and to investigate the factors predictive of long-term visual outcomes.
Methods:
This retrospective study included 31 eyes, with PCV treated with anti-VEGF therapy (either ranibizumab or bevacizumab, or both), and were followed up for 4 years or longer. The best-corrected visual acuity (BCVA) at baseline was compared with that measured at 3 months and at the final follow-up. Factors associated with final visual acuity were also analyzed.
Results:
The mean follow-up period was 53.0 ± 4.3 months. During the follow-up period, the patients were treated with an average of 8.8 ± 3.0 intravitreal anti-VEGF injections. BCVA at diagnosis at 12, 24, and 36 months, and at final follow-up was 0.52 ± 0.35, 0.46 ± 0.36, 0.57 ± 0.45, 0.76 ± 0.56, and 0.83 ± 0.60, respectively. When compared to the baseline value, the BCVA was significantly improved at 3 months (P = 0.006), whereas the BCVA at final follow-up was significantly decreased compared to the baseline value (P = 0.018). Among the included eyes, 48.4% experienced deterioration of visual acuity and 51.6% showed stable vision. BCVA at 12 months was most strongly associated with visual acuity at final follow-up.
Conclusions:
Although the long-term treatment outcome of PCV is generally unfavorable, stable vision can be achieved in approximately half of the patients. Visual acuity at 12 months after the initial treatment is predictive of long-term visual outcomes.
Introduction
A
Polypoidal choroidal vasculopathy (PCV) is a unique type of choroidal neovascularization and is characterized by polypoidal vascular lesions and branching vascular networks seen on indocyanine green angiography (ICGA).4,5 Although anti-VEGF therapy is generally considered to be an effective treatment for PCV,6,7 previous studies have reported that some cases of PCV respond poorly to this therapy. 8 Several studies have reported the long-term outcomes of anti-VEGF therapy in PCV.9–11 As ICGA was not routinely performed in early clinical trials of anti-VEGF therapy,1,2 the follow-up period of these studies was generally limited to less than 4 years.
In addition, all patients in the previous study who reported longer than 3 years of treatment outcomes were treated with ranibizumab (Lucentis, Genentech) monotherapy.10,11 Bevacizumab (Avastin, Genentech) is widely used for treating exudative AMD. It is reported that bevacizumab has comparable efficacy to ranibizumab in treating exudative AMD. 12 The efficacy of bevacizumab for treating PCV is also comparable to ranibizumab up to 1 year. 13 In clinical practice, long-term ranibizumab monotherapy is not possible in many cases, primarily due to the high cost of ranibizumab. In these cases, bevacizumab can be considered an alternative treatment. 14 Long-term clinical outcomes of PCV treated with both ranibizumab and bevacizumab remain to be elucidated.
The purpose of the present study was to report a longer than 4-year clinical outcome of PCV treated with anti-VEGF therapy. We additionally investigated factors predictive of long-term visual outcome.
Methods
This retrospective observational case series was performed at a single center. The study was approved by the Institutional Review Board of Kim's Eye Hospital and was conducted in accordance with the tenets of the Declaration of Helsinki.
The present study included patients who were diagnosed with treatment-naive PCV between September 2009 and March 2011 at our institution and were treated with anti-VEGF therapy. Only patients who were followed up for 4 years or longer were included. All subjects had undergone a comprehensive initial ophthalmologic examination, including measurement of best-corrected visual acuity (BCVA), 90-diopter lens slit lamp biomicroscopy, fundus photography, fluorescein angiography, spectral domain optical coherence tomography (OCT; Spectral OCT/SLO®; OTI Ophthalmic Technologies, Inc.), and ICGA, which was performed using a confocal laser-scanning system (HRA-2; Heidelberg Engineering GmbH).
The exclusion criteria included severe media opacity, −6.0 D or greater myopia, an axial length of 26.0 mm or greater, or concomitant retinal vascular disorders (eg, macroaneurysms, proliferative diabetic retinopathy, and central retinal vascular occlusion). Patients who underwent photodynamic therapy (PDT) or intraocular surgery during the follow-up period were also excluded. Where both eyes met the eligibility criteria, the first treated eye was included in the study. We recorded the BCVA at diagnosis and at 3 months in patients who met the eligibility criteria and who were treated with 3 ranibizumab injections as an initial treatment but were lost to follow-up before 4 years. The values at the 2 time points were compared between patients with and without 4 years or longer of follow-up.
Diagnosis of PCV was based on ICGA results. Two examiners (Y.S.C. and J.H.K.) performed the analyses. PCV was diagnosed by the presence of polypoidal lesions with or without branching vascular networks. Any disagreement was settled by discussion between the examiners. Central foveal thickness was defined as the distance between the internal limiting membrane and Bruch's membrane at the fovea, and was manually measured using calipers provided by an OCT software program. The greatest linear dimension of the entire PCV lesion, including the entire polypoidal lesions and branching vascular networks on ICGA, was also measured using the built-in calipers of the ICGA software program. Choroidal vascular hyperpermeability was defined as multifocal hyperfluorescent areas present in late-phase ICGA images. 15
All eyes included in the study were initially treated with 3 monthly intravitreal ranibizumab (0.5 mg/0.05 mL) injections. Afterward, patients were scheduled to visit the hospital at clinician discretion. Retreatment with intravitreal anti-VEGF, either ranibizumab (0.5 mg/0.05 mL) or bevacizumab (1.25 mg/0.05 mL), was performed in cases with remaining intraretinal/subretinal fluid after initial treatment, reaccumulation of subretinal or intraretinal fluid after the fluid had completely resolved, or retinal/subretinal hemorrhage.
The BCVA at diagnosis was compared with the BCVA at 3 months and at the final follow-up. The central foveal thickness at diagnosis was compared with measurements at 3 months. Eyes treated with ranibizumab monotherapy during the follow-up period were included in the ranibizumab group, and eyes treated with both ranibizumab and bevacizumab were included in the mixed-use group. BCVA at baseline and at final follow-up and the degree of change in BCVA during the follow-up period were compared between the 2 groups. To evaluate the factors predictive of visual acuity outcome, the following factors were selected as variables: patient age, greatest linear dimension, BCVA at diagnosis, central foveal thickness at diagnosis, duration of follow-up, number of anti-VEGF injections, and BCVA at 12 months. Factors with a P value <0.1 following univariate analysis were included in the multivariate analysis.
The included eyes were classified into 2 groups, according to the OCT findings at 3 months: a dry macula group (eyes without any intraretinal or subretinal fluid, regardless of retinal pigment epithelial detachment [RPED]) and a remaining fluid group (eyes exhibiting intraretinal or subretinal fluid). The BCVA at diagnosis and at the final visit and the degree of change in the BCVA during the follow-up period were compared between the 2 groups.
The BCVAs were changed to the logarithm of the minimal angle of resolution (logMAR) value for analysis. As recommended by Holladay, 16 the counter finger visual acuity was changed to logMAR value 2.
Data are presented as mean ± standard deviation, where applicable. Statistical analyses were performed with a commercially available software package (SPSS ver. 12.0 for Windows; SPSS, Inc.). Differences at various time points were analyzed using repeated-measures analysis of variances, and individual comparisons were made using Bonferroni's method. Associations between variables were analyzed using Pearson's correlation analysis and multiple linear regression analysis. Differences between the 2 different groups were analyzed using the Mann–Whitney U test or the independent samples t-test with Bonferroni's correction. Comparison of the central foveal thickness between the 2 time points was performed using the paired t-test. A P value <0.05 was considered significant.
Results
During the study period, 3 ranibizumab injections were administered to 213 patients with PCV (213 eyes) as an initial treatment. A total of 182 patients (85.4%) were lost to follow-up before 4 years. As a result, 31 eyes from 31 patients (21 men and 10 women) met the inclusion criteria (Table 1). Mean age was 67.9 ± 7.9 years. Mean central foveal thickness was 358.3 ± 74.8 μm and the mean greatest linear dimension was 2,132.8 ± 816.8 μm. Choroidal vascular hyperpermeability was observed in 7 eyes (22.6%). The mean follow-up period was 53.0 ± 4.3 months (48–64 months).
Data presented as mean ± standard deviation, where applicable.
BCVA, best-corrected visual acuity; logMAR, logarithm of minimal angle of resolution.
The mean number of visits was 20.5 ± 3.1 during the follow-up period and the recurrence of fluid or persisting fluid requiring anti-VEGF injection was noted on 5.1 ± 2.4 visits. During the follow-up period, patients were treated with an average of 8.8 ± 3.0 intravitreal anti-VEGF injections, including 5.8 ± 2.3 ranibizumab injections and 2.9 ± 2.8 bevacizumab injections. Recurrence of fluid was observed in 30 eyes (96.8%) during the follow-up period, and these eyes received additional anti-VEGF therapy. The incidence of intraretinal fluid at the fovea, subfoveal fluid, serous subfoveal pigment epithelial detachment, geographic atrophy, and disciform scar is presented in Table 2.
Data presented as number of eyes (%).
The mean BCVA was 0.52 ± 0.35 at diagnosis, 0.39 ± 0.32 at 3 months, 0.46 ± 0.36 after 12 months, 0.57 ± 0.45 after 24 months, 0.76 ± 0.56 after 36 months, and 0.83 ± 0.60 at final follow-up (mean 53.0 months) (Fig. 1). When compared to the baseline value, the BCVA was significantly improved at 3 months (P = 0.006), whereas the BCVA at final follow-up was significantly decreased compared to the baseline value (P = 0.018). Compared to baseline BCVA, deterioration of ≥0.2 logMAR BCVA was observed in 15 eyes (48.4%) at the final follow-up. The remaining 16 eyes (51.6%) had stable visual acuity. None of the eyes included showed an improvement of ≥0.2 logMAR BCVA. Figure 2 shows the proportion of patients with ≥20/40, 20/200–20/40, and <20/200 visual acuity. At diagnosis, 16 eyes (51.6%) had ≥20/40, 14 eyes (45.2%) had 20/200–20/40, and 1 eye (3.2%) had <20/200 visual acuity. At final follow-up, 8 eyes (25.8%), 14 eyes (45.2%), and 9 eyes (29.0%) had the aforementioned visual acuity, respectively. At 3 months, the mean central foveal thickness was 289.4 ± 97.3 μm. There was a significant difference between the central foveal thickness at diagnosis and at 3 months (P < 0.001). Figure 3 shows a representative case of PCV treated with anti-VEGF therapy.

A line plot
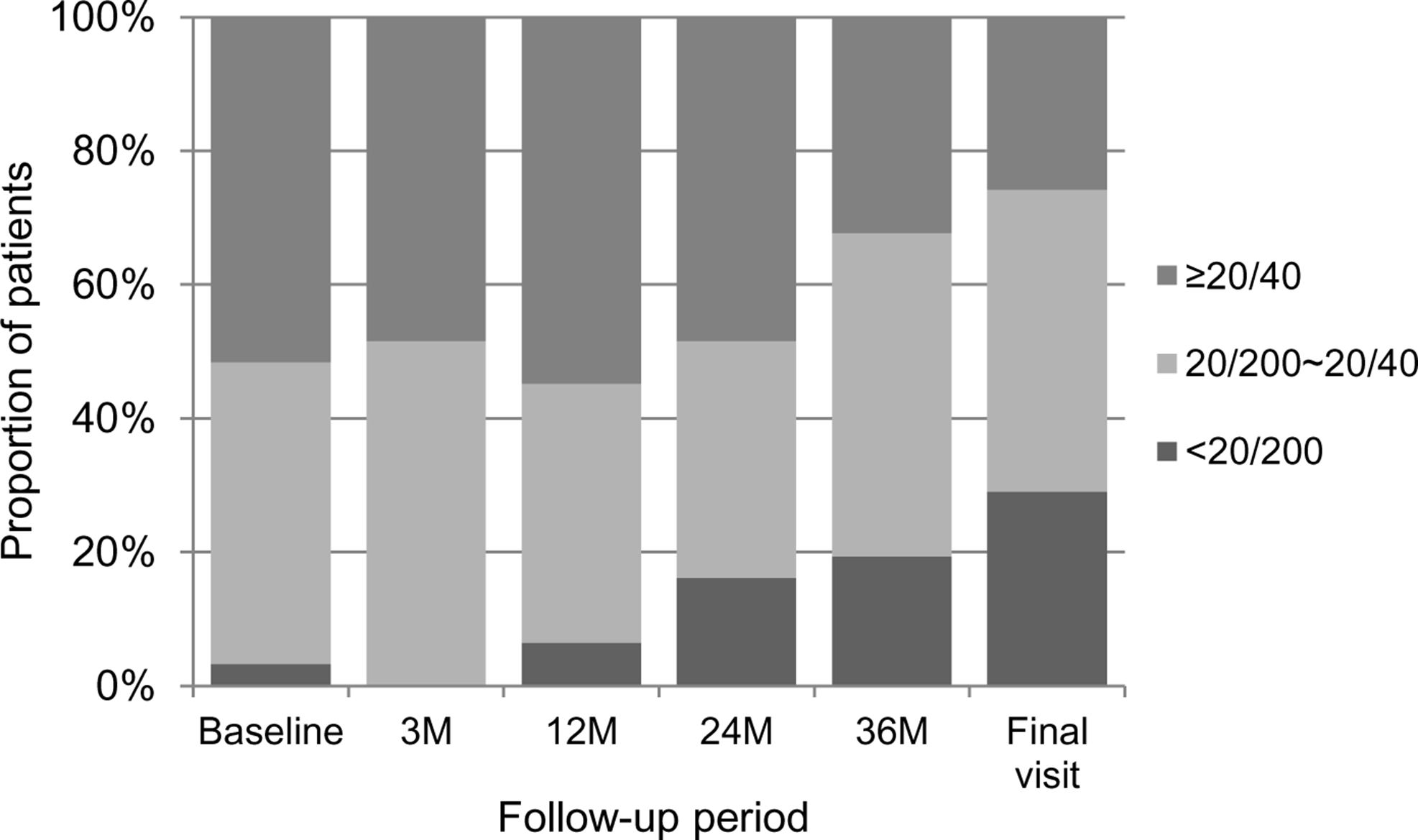
Changes in the proportion of patients with ≥20/40, 20/200–20/40, and <20/200 visual acuity, according to follow-up period. Final visit, mean 53.0 ± 4.3 months.

Optical coherence tomography images taken at diagnosis
Nine eyes (29.0%) were included in the ranibizumab monotherapy group and the remaining 22 eyes (70.9%) were included in the mixed-use group. The ranibizumab monotherapy group showed significantly better BCVA at baseline (P = 0.018) and at final follow-up (P = 0.003). However, the degree of change in BCVA during the follow-up period was not different between the 2 groups (P = 0.084).
The mean number of visits was 21.5 ± 3.1 during the follow-up period. Recurrence of fluid or persistent fluid requiring an anti-VEGF injection was noted during 5.3 ± 2.7 visits. The ocular findings at final follow-up are summarized in Table 2. In 9 eyes (29.0%), neither intraretinal fluid at the fovea nor subfoveal fluid was observed. In the remaining 22 eyes (70.9%), pathologic findings, including intraretinal fluid at the fovea or subfoveal fluid (22.6%), serous subfoveal pigment epithelial detachment (19.4%), geographic atrophy (3.2%), and disciform scar (6.5%), were observed.
Table 3 summarizes the results of analyses of factors associated with BCVA at the final visit. In the univariate analysis, final visual acuity was significantly associated with greatest linear dimension (P = 0.032, r = 0.386), BCVA at diagnosis (P = 0.036, r = 0.378), and BCVA at 12 months (P < 0.001, r = 0.793). Final visual acuity was not associated with age (P = 0.493), central foveal thickness at diagnosis (P = 0.419), duration of follow-up (P = 0.638), or the number of anti-VEGF injections (P = 0.379). In the multivariate analysis, the most significant predictive factor of BCVA at the final visit was BCVA at 12 months (P < 0.001).
Statistics analyzed by Pearson correlation analysis.
Statistics analyzed by multiple linear regression analysis.
VEGF, vascular endothelial growth factor.
When classified into 2 groups according to the OCT findings at 3 months, 23 and 8 eyes were classified in the dry macula group and the remaining fluid group, respectively. In the dry macula group, the mean BCVA at diagnosis, the BCVA at the final visit, and the degree of deterioration in the BCVA during the follow-up period were 0.47 ± 0.33, 0.70 ± 0.61, and 0.24 ± 0.49, respectively. In the remaining fluid group, the values were 0.58 ± 0.37, 0.99 ± 0.59, and 0.41 ± 0.70, respectively. The difference in the BCVA at diagnosis (P = 0.359), at the final visit (P = 0.157), and in the degree of deterioration in the BCVA during the follow-up period (P = 0.465) between the 2 groups was not significant.
In the 182 patients lost to follow-up before 4 years, the BCVA at diagnosis and at 3 months was 0.64 ± 0.53 and 0.46 ± 0.44, respectively. The BCVA at diagnosis (P = 0.240) and at 3 months (P = 0.842) was not different between patients with and without 4 years or longer of follow-up.
Discussion
Recently, Cheung et al. reported the long-term natural history of 32 eyes with PCV. 17 At a mean of 59.9 months postdiagnosis, visual deterioration was observed in 62.5% of eyes examined. At the final follow-up, 53.1% of eyes exhibited worse than 1.0 logMAR visual acuity. 17 Although there was no control group in the present study, visual prognosis of our patients was relatively favorable, with visual deterioration in 48.4% eyes and worse than 1.0 logMAR observed in 9 eyes (29.0%) at final follow-up. This result may suggest a long-term benefit of anti-VEGF therapy in PCV.
Several studies have reported a long-term visual outcome of PCV treated with intravitreal ranibizumab monotherapy.10,11 Kang and Koh retrospectively evaluated the outcome of a mean of 42.6 months of ranibizumab treatment in 36 eyes with PCV. 10 The mean logMAR visual acuity at baseline was 0.68 ± 0.43 and after 3 years was 0.78 ± 0.53. After 3 years, 7 eyes (19.4%) showed improved vision, 21 eyes (58.4%) had stable vision, and in 8 eyes (22.2%) the vision had deteriorated. More recently, Hikichi prospectively evaluated the 3-year treatment outcome of 128 eyes with PCV. 11 The visual acuity at baseline was 0.61 ± 0.51 and after 36 months was 0.52 ± 0.47. After 3 years, visual acuity had significantly improved compared to baseline values. Compared to previously reported results, the treatment outcome was relatively unfavorable in our patients.
We postulate that the following factors may contribute to discrepancies between our study and previous studies. The study by Hikichi is prospective and therefore strict treatment and follow-up may have been performed. 11 In contrast, our study was retrospective and no single treatment protocol was followed for all patients. Follow-up was performed every 1–4 months at the discretion of the treating physician. It has been reported that a delay in treatment is associated with poor visual prognosis in exudative AMD. 18 We postulate that the detection of recurrence may have been delayed in some patients and therefore influenced poor prognosis. Recurrence of exudation is associated with poor prognosis in PCV. 10 In a study by Kang and Koh, 10 stable visual acuity was maintained throughout a 3-year follow-up period in eyes without recurrence, whereas continuous visual acuity deterioration was observed in eyes with recurrence after 12 months. In the present study, recurrence of fluid was observed in almost all patients, whereas 66.7% of patients in the study by Kang and Koh experienced fluid recurrence. 10 This high rate of recurrence in our patients may partially contribute to their poor prognosis.
Intravitreal bevacizumab is a useful treatment option for PCV.19–21 In a study by Cho et al., 13 bevacizumab and ranibizumab showed comparable 12-month efficacy in terms of functional and anatomical outcomes. In the present study, the majority of patients were treated with intravitreal ranibizumab and bevacizumab, and was termed the mixed-use group. The ranibizumab-only group showed better final visual outcome than the mixed-use group. However, the ranibizumab-only group also showed better visual acuity at diagnosis and received fewer injections, suggesting that this group of patients exhibited more indolent disease activity. Thus, our data may not support the superior efficacy of ranibizumab monotherapy compared to the use of both ranibizumab and bevacizumab. The degree of visual acuity change during the follow-up period was not different between the 2 groups. As our study was not controlled to identify differences in the efficacy of both treatment methods, further prospective studies are required in this area.
Factors predictive of long-term visual outcomes in PCV were age, 22 baseline visual acuity, 22 presence of cluster of grape-like polypoidal lesions, 22 greatest linear diameter, 10 pigment epithelial detachment, 10 and recurrence during follow-up. 10 In the present study, greater linear dimension, baseline visual acuity, and visual acuity at 12 months were closely associated with final visual acuity. Among them, visual acuity at 12 months was found to be the most reliable predictive factor for final visual acuity. This result suggests that response to initial anti-VEGF therapy is important in determining long-term visual outcome.
In the present study, the dry macular group showed a slightly better BCVA at diagnosis and at the final visit, and a lesser degree of deterioration in the BCVA than the remaining fluid group. However, the difference was not significant. We postulate that the relatively small sample size contributed to this insignificant result. The association between the results at 3 months and the long-term clinical outcome needs further investigation using a larger study population.
In addition to its retrospective nature, this study has other limitations. Results were analyzed for only a limited proportion of patients who were diagnosed with PCV. Although patients lost to follow-up showed relatively better visual acuity at diagnosis and at 3 months, the values were not significantly different from those of the included patients. In addition, the trend in BCVA changes over 36 months in our patients was relatively comparable to previously reported values. 10 For these reasons, we postulate that our data may not be significantly different from the clinical outcome of ordinary PCV cases. Nevertheless, further studies with consecutive patients are required to verify our findings. All patients received initial treatment with 3 monthly intravitreal ranibizumab. However, there was no single treatment guideline for recurred cases. There was no macular thickness guideline for recurrence of fluid. Further treatment decisions may differ between physicians and this may influence the study results. Following a strict treatment strategy in the long term is generally not possible in clinical practice. In addition, a previous study that investigated real-world experience showed that the injection frequency is relatively lower in routine clinical practice than in clinical trials. 23 The result of the present study reflects long-term treatment outcomes in a clinical setting. Although anti-VEGF therapy is a widely used first-line therapy for PCV, previous reports suggest that rescue PDT is beneficial for cases refractory to anti-VEGF therapy. 24 In this retrospective study, there was no common guideline for rescue PDT and patients who underwent PDT were excluded from the analysis. The effect of rescue PDT on long-term treatment outcomes needs further investigation.
In summary, the present study reports a mean 53.0-month long-term treatment outcome of anti-VEGF therapy for PCV. Although long-term outcome is generally unfavorable, severe visual loss was prevented in approximately half of the eyes examined, suggesting that anti-VEGF therapy has a long-term benefit for these patients.
Footnotes
Acknowledgment
This study was supported by the Kim's Eye Hospital Research Center.
Author Disclosure Statement
No competing financial interests exist.