
Abstract
The online-ahead-of-print published article, “Azithromycin 1.5% Ophthalmic Solution for Blepharitis Treatment: Comparison of 14- Versus 30-Day Treatment,” by Altay Yesim, Demirok Gulizar, Balta Ozgur, and Bolu Hulya (DOI: 10.1089/jop.2015.0099) is being officially retracted from Journal of Ocular Pharmacology and Therapeutics (JOPT) due to post-publication authorship disputes and the discovery of simultaneous submission to both JOPT and the International Journal of Ophthalmology, which is a violation of the proper protocols of peer review.
Journal of Ocular Pharmacology and Therapeutics
and its editorial leadership are committed to maintaining the highest levels of scientific reporting and publishing, and therefore officially retracts the article based on the infringements listed herein.
Introduction
Blepharitis is one of the most commonly encountered conditions in ophthalmology practice. Anterior and/or posterior blepharitis may be present in 37%–47% of patients observed by ophthalmologists.1,2 The clinical symptoms are usually chronic and include burning, itching, foreign body sensation, redness, and crusty eyelids. The clinical signs include eyelid margin hyperemia, plugging of the meibomian gland (MG) orifices, abnormally thickened MG secretions, and foamy tears, which may be associated with dry eye due to evaporative tear loss.1,2 Treatment is difficult with no consistently successful therapies, making blepharitis a chronic condition characterized by exacerbations and remissions in a majority of patients. Because of the relapsing nature of the disease, the treatment regimen usually lasts a lifetime. Standard treatment consists of local eyelid hygiene and eyelid scrubs with warm compresses. Adjunctive treatments include topical antibiotics, systemic antibiotics (usually tetracyclines), topical corticosteroids, topical cyclosporin A, and tear replacement therapy. 2
Most cases of chronic blepharitis are associated with a bacterial component usually consisting of Gram-positive organisms such as Staphylococcal species. Azithromycin is a second-generation macrolide group antibiotic. Its antibacterial activity is directed against several Gram-positive and -negative bacteria in addition to atypical bacteria.3,4 Its other advantages are the anti-inflammatory properties, a high tissue distribution, and prolonged postantibiotic effect in vivo.5–8
Because of high tissue distribution and prolonged postantibiotic effect of azithromycin, we aimed to investigate whether a 2-week treatment of topical azithromycin ophthalmic solution combined with eyelid hygiene and warm compresses is as effective as a 1-month treatment.
Methods
A total of 60 patients diagnosed with chronic blepharitis, which is defined as the presence of symptoms more than 6 months, were randomly assigned to 2 groups. Randomization was performed according to the order of admission of the patients. This study was performed between November 2014 and March 2015, and it was approved by the Institutional Review Board, according to the principles of the Declaration of Helsinki. An informed consent was obtained from all the patients included in the study.
The exclusion criteria were the presence of eyelid structural anomaly, ocular surface infection, ocular allergy, contact lens wear, and use of any of the following medications in the past 1 month: systemic or topical antibiotics, topical or systemic steroids, and ocular nonsteroidal drugs.
All patients were treated with eyelid hygiene using baby shampoo and 10 min of warm compresses once a day. No lubricant eye drops were used by the patients during the study period because their use would affect the tear break-up time (TBUT) and Schirmer's test results.
Group 1 patients were treated with topical 1.5% azithromycin ophthalmic solution (Azyter™, Laboratories Thea, France) twice a day for 2 days and then once a day for 12 days (total 2 weeks). Group 2 patients were treated with the same drug twice a day for 2 days and then once a day for the rest of the month. The clinical symptoms and signs of the patients were recorded and graded before treatment, at the end of treatment, and 1 month after the end of treatment. The scoring system was adapted from the grading system described in the study by Foulks et al. 9
All patients were asked about the presence of the following symptoms: itching, foreign body sensation, burning, and eyelid swelling. These symptoms were categorized into 4 grades from 0 to 3 according to severity. The following clinical signs were identified by slit-lamp examination: conjunctival redness, eyelid margin redness, eyelid margin debris, MG secretion, and MG expression, and they were graded from 0 to 3 according to severity (Table 1). Because symptoms were subject rated and clinical signs were examiner rated, 1 ophthalmologist (Y.A.) examined and scored the clinical signs of all patients at baseline and at follow-up visits.
Grading of Symptoms and Clinical Signs of Patients with Blepharitis
For each symptom or sign; first, the number of patients in each grade were recorded and second, the mean scores of each symptom/sign were calculated. The study eye was determined as the eye having a higher total score for the clinical signs and symptoms of blepharitis. If the total score for each eye was equal, the right eye was selected.
Schirmer's test and TBUT values were measured for all patients before the treatment, at the end of treatment, and at 1-month follow-up.
The TBUT was measured as follows: fluorescein was instilled in each eye and while the patient looked straight ahead, the tear film was examined using cobalt blue fılter with a biomicroscope. The time from the blink to the appearance of the first tear break-up was recorded in seconds. After these measurements, 1 drop of a topical anesthetic was instilled and a sterile Schirmer's strip was placed in the temporal one-third of the lower eyelid fornix. The eyes were closed and after 5 min, the Schirmer's score was recorded in millimeters.
In group 1, after 2 weeks (at the end of treatment), the subjects underwent biomicroscopic examination; the grades of signs and symptoms of blepharitis were recorded and TBUT and Schirmer's test were performed again. In group 2, the same examination was performed at the end of 1 month. The same analyses were repeated at 1-month follow-up visits in both groups and the results were compared.
Statistical analyses were performed using the SPSS™ software version 15.0. Shapiro–Wilk's test was performed to determine the normal distribution of the variables. The results of descriptive analyses are presented as means and standard deviations for normally distributed variables. Since age, TBUT, and Schirmer's test values were normally distributed, the Student's t-test was used to compare these variables between the treatment groups, and paired t-test was used to compare these variables before and after treatment within the same treatment group. The symptom scores and clinical findings of the patients (the number of patients in each grade of symptoms or clinical signs) were compared between the groups using the Chi-square test, and they were compared within the same treatment group before and after treatment, using a Wilcoxon signed rank test. A P<0.05 was considered to be statistically significant.
Results
The mean age of the patients in group 1 was 46.36±10.86 years and that of group 2 patients was 49.96±8.98 years. Group 1 consisted of 13 men (43.3%) and 17 women (56.7%), and group 2 comprised 14 men (46.7%) and 16 women (53.3%). Age and gender distributions among the groups were not statistically different (P=0.16, Student's t-test, P=0.79, Chi-square, respectively).
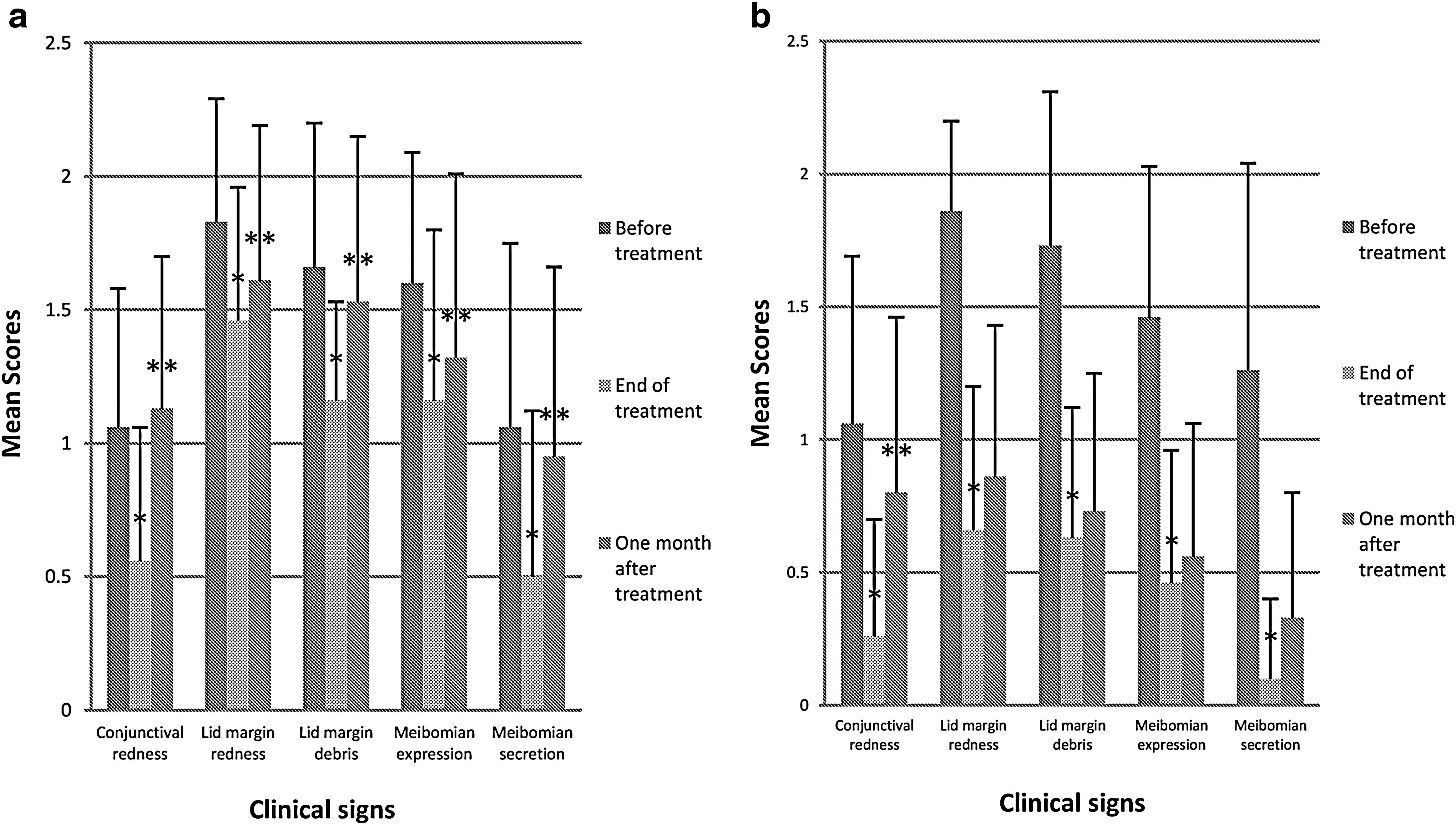
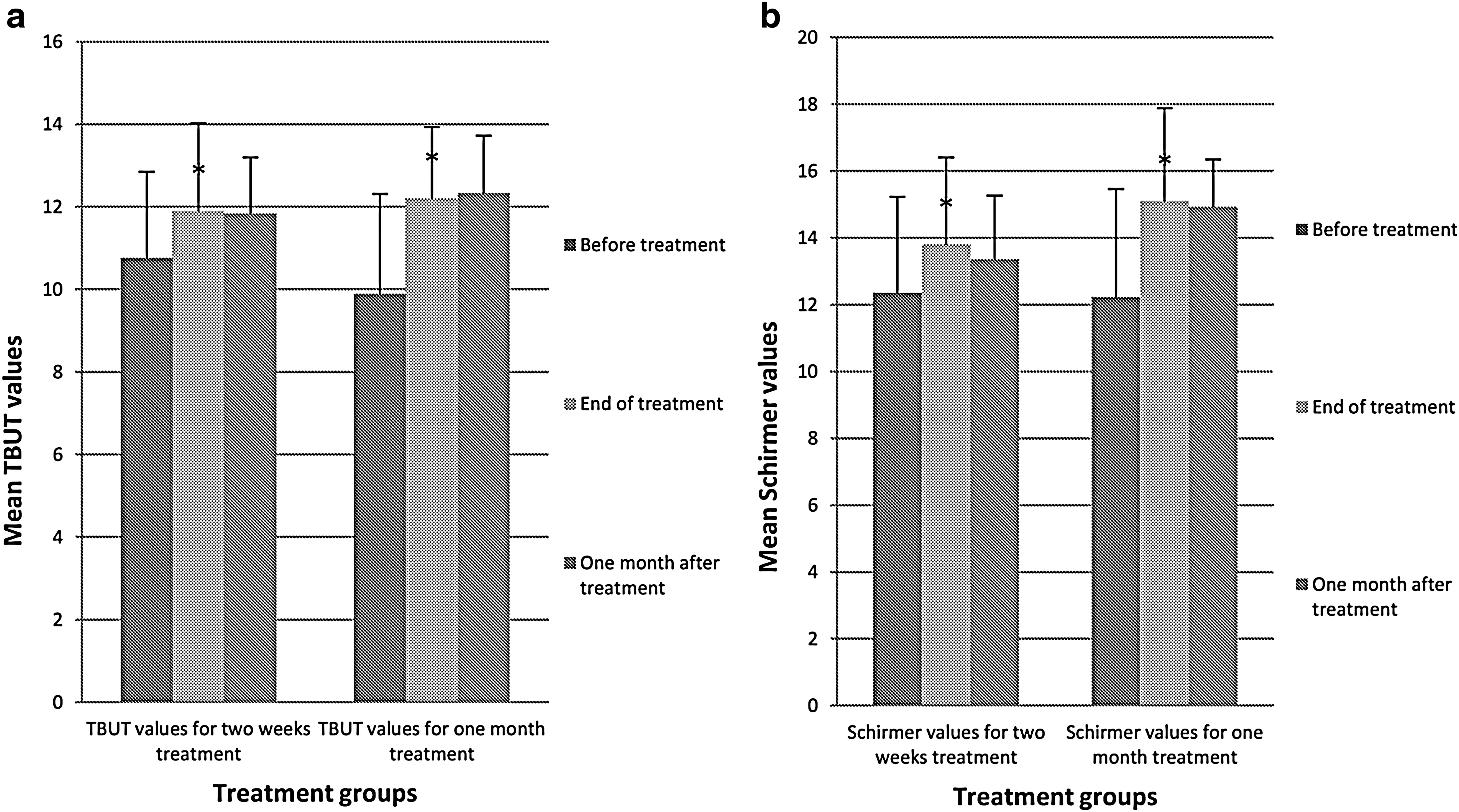
Before treatment, there were no differences in the clinical symptoms and signs and TBUT and Schirmer's test values between the 2 groups (P>0.05). At the end of treatment, both groups showed a significant improvement in the symptoms and clinical findings compared to baseline (Table 2) (Figs. 1a, b and 2a, b). The TBUT and Schirmer's test values were also significantly increased compared to baseline values (Table 1) (Fig. 3a, b).

Differences of Symptoms, Clinical Signs, TBUT, and Schirmer Values Within the Same Treatment Group Before and After the Treatment
And comparison of results between groups after treatment. The scores are presented as mean ± standard deviation (SD).
P 1 Comparison of values before and at the end of treatment within the same treatment group, Wilcoxon signed rank test. (paired t-test for TBUT and Schirmer).
P 2 Comparison of values at the end of treatment between the treatment groups, Chi-square test, (student's t-test for TBUT and Schirmer).
Statistically significant difference, within the same treatment group.
Statistically significant difference, between the treatment groups.
TBUT, tear break-up time; NS, statistically nonsignificant difference.
At the end of treatment, when the patient groups were compared by symptoms, there was no difference except the eyelid swelling score (P=0.02). However, the clinical findings of group 2 patients showed a significantly better improvement in terms of conjunctival redness, redness of eyelids, lid margin debris, MG expression, and MG secretion (Table 2) (Figs. 1a, b and 2a, b). However, there was no difference between the groups in terms of TBUT and Schirmer's test values (P=0.61 and P=0.56, respectively) (Table 2) (Fig. 3a, b).
The symptoms and clinical signs of the patients at the end of treatment and 1 month after treatment were compared within the same treatment group using Wilcoxon signed rank test. At the 1-month follow-up visit, the symptoms and clinical findings of the patients in group 1 showed significant worsening; however, group 2 patients showed a significant worsening mostly in terms of symptoms and not clinical signs (Table 3) (Figs. 1a, b and 2a, b). The TBUT and Schirmer's test values at the end of treatment and 1-month follow-up did not show any statistically significant difference in both groups (Table 3).
Differences of Symptoms, Clinical Signs, TBUT, and Schirmer Values Within the Same Treatment Group Following the Treatment and 1 Month After the End of Treatment
And comparison of results between groups 1 month after treatment.
The scores are presented as mean±SD.
P 1 Comparison of values at the end of 1 month and after the end of treatment within the same treatment group, Wilcoxon signed rank test. (paired t-test for TBUT and Schirmer)
P 2 Comparison of values 1 month after the end of treatment between the treatment groups, Chi-square test. (student's t-test for TBUT and Schirmer)
Statistically significant difference, within the same treatment group.
Statistically significant difference, between the treatment groups.
At the 1-month follow-up visit, the itching score, MG expression, MG secretion, and Schirmer's values showed a statistically significant long-lasting improvement in group 2 compared with group 1 (Table 3) (Figs. 1–3).
Discussion
Although blepharitis is a common and chronic disorder, there is no consensus on standard management. The etiology of the disorder is complex and not completely understood, but the general consensus is that bacteria and inflammation contribute to the pathology.
One theory suggests that chronic blepharitis is the result of hyperkeratinization of the epithelium lining the MG ducts.1,7,3 Once MGs are obstructed, bacterial colonization occurs and inflammatory mediators are released that contribute to the development of patients' symptoms and clinical signs. The lipolytic enzymes released by the bacteria result in highly irritating free fatty acids that compromise the integrity of the tear film. 10 Both the MG structural changes and secretions cause increased evaporation of the tear film and increased inflammatory cytokines that ultimately damage the ocular surface. Treatment generally includes eyelid hygiene, warm compresses, topical and systemic antibiotics, topical steroids, and topical cyclosporin A.11–14
In the current study, we investigated the efficacy of topical 1.5% azithromycin ophthalmic solution for the treatment of blepharitis. We also used 2 different durations of treatment (2 weeks vs. 1 month). Both groups showed a statistically significant improvement from baseline in the clinical symptoms and signs, in terms of TBUT and Schirmer's test values. However, between the groups, the clinical signs (conjunctival hyperemia, eyelid redness, eyelid debris, MG expression, and MG secretion) and Schirmer's test values showed a statistically significantly better and long-lasting improvement in group 2 compared with group 1. We decided to follow up the patients till 3 months after the end of treatment; however, most of the patients were lost to follow-up. Therefore, we could not evaluate the third-month follow-up visit as the number of patients was not enough for a statistical comparison. This is a limitation of the present study.
Azithromycin is a broad-spectrum antibiotic that has been shown as effective against Gram-positive, -negative, and atypical bacteria, including Haemophilus influenza, Staphylococcus aureus, Streptococcus pneumoniae, and Chlamydia trachomatis. The antibacterial effect of azithromycin occurs by binding to the 50S subunit of the 70S bacterial ribosome and inhibiting the RNA-dependent protein synthesis within the bacteria. Following oral administration, azithromycin is taken up primarily by the phagocytic cells and fibroblasts. During active phagocytosis, large concentrations of azithromycin are released directly to the infection site. 15 Studies have shown that following oral administration of azithromycin in rabbits as well as human subjects undergoing cataract surgery,15–17 high drug concentrations were observed in tissues (i.e., cornea, conjunctiva, iris, and ciliary body) in contrast with the low concentrations in fluids (vitreous and aqueous). Consistent with the tendency of azithromycin to distribute preferentially in tissues, the levels of azithromycin observed in the aqueous humor following ocular administration were relatively low.7,8 After approval of the dosing regimen by the Food and Drug Administration for the treatment of bacterial conjunctivitis (1 drop twice a day for 2 days, followed by 1 drop per day for 5 days), some studies have reported clinically significant concentrations of azithromycin in the conjunctiva, cornea, and eyelids as early as 1 h after the first administration, and the level of drug remained high for up to 6 days after the end of treatment.7,9 This shows that azithromycin may potentially be used in the treatment of ocular surface disorders that require chronic suppressive antibiotic treatment. Its pharmacokinetic properties also provide advantages of once- or twice-daily dosing, which may be beneficial for patient compliance.
In addition to its broad-spectrum antimicrobial activity, azithromycin demonstrates anti-inflammatory properties. It is believed to suppress the production of proinflammatory mediators such as cytokines (TNF-α and IL-1β), chemokines, and matrix metalloproteinases (MMP-1, MMP-3, and MMP-9).5,17
Most of the studies that evaluated azithromycin in blepharitis used 1% solution (AzaSite), which is formulated with DuraSite, a polycarbophil-based vehicle designed to prolong drug residence on the ocular surface. Some of the studies that used 1% azithromycin solution are summarized in Table 4.1,9,18,19 Those studies usually followed up on patients 1 month after the end of treatment.
Summary of Some Studies Using 1% Azithromycin Ophthalmic Solution for Treatment of Blepharitis
Few studies have used 1.5% azithromycin ophthalmic solution (Azyter, which is not polycarbophil based) for the treatment of blepharitis. For instance, in the study by Fadlallah et al., 20 a total of 33 patients were treated with topical 1.5% azithromycin twice a day for 3 days and 34 patients were treated with topical 1.5% azithromycin twice a day for 3 days and then at bedtime for the rest of the month. All patients also applied warm compresses and performed lid hygiene twice daily for the duration of trial. At 1-week and at 1-month follow-up, both treatment groups showed significant improvements from baseline in blepharitis symptoms and ocular signs, including lid collarettes and lid redness/swelling. The total MGD score was significantly improved at 1 month, only for the group that received azithromycin for the entire month. After 3 months of follow-up, both treatment groups continued to report improved symptoms, however, only the regimen with continued treatment for 1 month maintained improvements in signs of disease (lid redness/swelling, plugging, and quality of MG secretions). 20
In our study, at the end of treatment, both groups showed significant improvements in all symptoms and clinical findings. TBUT and Schirmer's test values also significantly increased. After the 1-month follow-up, while both treatment groups continued to report improvement in TBUT and Schirmer's test values, both groups showed significant worsening in symptoms. Group 1 also showed significant worsening of all clinical scores. However group 2 maintained improvement in clinical signs except conjunctival redness and lid margin redness scores.
As a result, since all patients in both groups applied lid hygiene and warm compresses as a standard therapy, our study showed that 1-month treatment of 1.5% azithromycin solution for blepharitis is more effective and it has a long-lasting effect. This finding is similar to the result of the study by Fadlallah et al. In addition, our study showed that 1.5% azithromycin ophthalmic solution improved TBUT and Schirmer's test results, which is not investigated or reported in previous studies.
Since blepharitis is a chronic disease with recurrences, further studies with longer follow-up periods are needed to determine the duration of remission after the 1-month treatment regimen. By knowing this, repeat doses of treatment can be applied to lengthen the period of remission.
In conclusion, the 1-month treatment regimen with 1.5% azithromycin ophthalmic solution appears as more effective and having a long-lasting improvement compared with the 2-week treatment regimen for chronic blepharitis. Convenient dosing is also an advantage of azithromycin therapy in these patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.