
Abstract
Abstract
Purpose:
To report our results of 4 patients about the efficacy and safety of intravitreal dexamethasone implant for type 1 idiopathic macular telangiectasia (IMT).
Methods:
Four patients' charts with type 1 IMT treated with intravitreal dexamethasone implant were retrospectively reviewed. All patients underwent full ophthalmic examination including best corrected visual acuity (BCVA), spectral domain optical coherence tomography, and fluorescein angiography. BCVA, central macular thickness (CMT), and macular volume (MV) were evaluated.
Results:
The median BCVA was logMAR 0.55 (range 0.2–1.3) at baseline, improved to logMAR 0.45 (range 0.2–1) at 2 months after the first injection, and deteriorated to logMAR 0.7 (range 0.2–1) at final visit. The median CMT was 393 μm (range 283–410 μm) and MV was 2.70 mm3 (range 1.96–2.87 mm3) at baseline. Two months after the first injection median CMT decreased to 327 μm (range 269–356 μm) and MV decreased to 2.45 mm3 (range 1.93–2.57 mm3). At final visit median CMT slightly increased to 342 μm (range 258–444 μm) and MV slightly increased to 2.56 mm3 (range 1.93–2.89 mm3). None of the changes were statistically significant.
Conclusion:
Considering the effects of dexamethasone on macular edema intravitreal dexamethasone implant can be used in selected cases. Randomized clinical trials with larger sample size are needed for further evaluation.
Introduction
I
Intravitreal dexamethasone implant has been brought into use for the treatment of macular edema following retinal vein occlusion and noninfectious posterior uveitis for a couple of years. The implant has also started to be used for diabetic macular edema. As far as we know there are 2 case reports in the literature about intravitreal dexamethasone implant for type 1 IMT patients.19,20 Given the steroids' vascular stabilizator effect, intravitreal dexamethasone implant can be beneficial in the treatment of perifoveal telangiectatic vessels and aneurysms.
Herein, we report the safety and efficacy of intravitreal dexamethasone implant in the treatment of macular edema due to type 1 IMT.
Methods
Retrospective review of 4 type 1 IMT patients treated with intravitreal dexamethasone implant (0.7 mg Ozurdex; Allergan, Inc., Irvine, CA) from August 2013 to May 2015 was done. The intravitreal dexamethasone treatment was performed after approval from the local ethic committee. The study adhered to the tenets of the Declaration of Helsinki and a detailed informed consent was taken from each patient.
All patients underwent full ophthalmic examination including measurements of best corrected visual acuity (BCVA) and intraocular pressure, slit-lamp biomicroscopy, dilated fundus examination, spectral domain optical coherence tomography (SD-OCT) (Optovue; Optovue, Inc., Fremont, CA), and fluorescein angiography (FA). Classification of IMT was based on the findings reported by Yannuzzi et al. 3
BCVA was measured by a standardized Snellen chart. SD-OCT measurements of central macular thickness (CMT) and macular volume (MV) in central 3 mm were calculated with MM5 protocol consisting of 5 × 5 mm grid of linear scans around the macula. Inaccurate measurements were corrected manually.
Patients who had systemic diseases like diabetes, a history of any retinal disease, and parafoveal edema without loss of foveal contour were excluded from the study. Postoperative findings of the patients who had cataract surgery during the follow-up were not included as well.
Intravitreal dexamethasone implant (0.7 mg) was administered through pars plana injection. Topical fluoroquinolone was given prophylactically for 3 days. After each injection FA and SD-OCT were performed together with full ophthalmic examination at 2, 4, and 6 months.
Retreatment was planned whenever leakage recurred or visual acuity decreased. Outcome measures were changes in BCVA, CMT, and MV from baseline to 2 months after the first injection and to final visit.
Data analysis
Snellen visual acuity was converted to logarithm of the minimal angle of resolution (logMAR) for statistical analyses. Data were expressed as median (range). Wilcoxon signed rank test was used for the comparisons. P < 0.05 was considered to be statistically significant.
Results
Among the 4 patients included in this study 3 were male and one was female. All the patients were treated with intravitreal dexamethasone implant. The median age of the patients was 66 years (range 50–71 years). The median follow-up time was 16 months (range 10–21 months). One patient had 4 injections, 1 patient had 1 injection, and the other 2 patients had 3 injections. Previous treatments and follow-up periods of the patients are shown in Table 1.
IVB, intravitreal bevacizumab.
The median BCVA was logMAR 0.55 (range 0.2–1.3) at baseline, improved to logMAR 0.45 (range 0.2–1) at 2 months after the first injection and deteriorated to logMAR 0.7 (range 0.2–1) at final visit. Changes from baseline to 2 months after the first injection and from baseline to final visit in BCVA were not statistically significant. The median CMT was 393 μm (range 283–410 μm) and MV was 2.70 mm3 (range 1.96–2.87 mm3) at baseline. Two months after the first injection median CMT decreased to 327 μm (range 269–356 μm) and MV decreased to 2.45 mm3 (range 1.93–2.57 mm3). Changes in CMT and MV were not statistically significant. At final visit median CMT slightly increased to 342 μm (range 258–444 μm) and MV slightly increased to 2.56 mm3 (range 1.93–2.89 mm3). Changes in CMT and MV were not statistically significant. BCVA, CMT, and MV at baseline, 2 months after the first injection and final visit are shown in Table 2. SD-OCTs and FAs at baseline, 2 months after the first injection and final visit of all patients are shown in Fig. 1.

Clinical effect of dexamethasone implant on vascular leakage and macular thickness in type 1 idiopathic macular telangiectasia.
CMT, central macular thickness; MV, macular volume; VA, visual acuity.
Patient 1 showed large reduction in CMT after every injection, however, the efficacy of dexamethasone implant was temporary. Reduction in vascular leakage was compatible with decrement in CMT. In both patients 2 and 3 marked reduction in CMT was seen after the first 2 injections but the effect of third injection was not as significant as the first 2 injections. As a result CMT returned to its baseline level at final follow-up. Vascular leakage slightly decreased after the first 2 injections but returned back to its original state at final visit. Patient 4 showed only a slight reduction in both CMT and vascular leakage after the injection. Follow-up graphic displaying CMT changes of all patients before and after the injections is shown in Fig. 2.
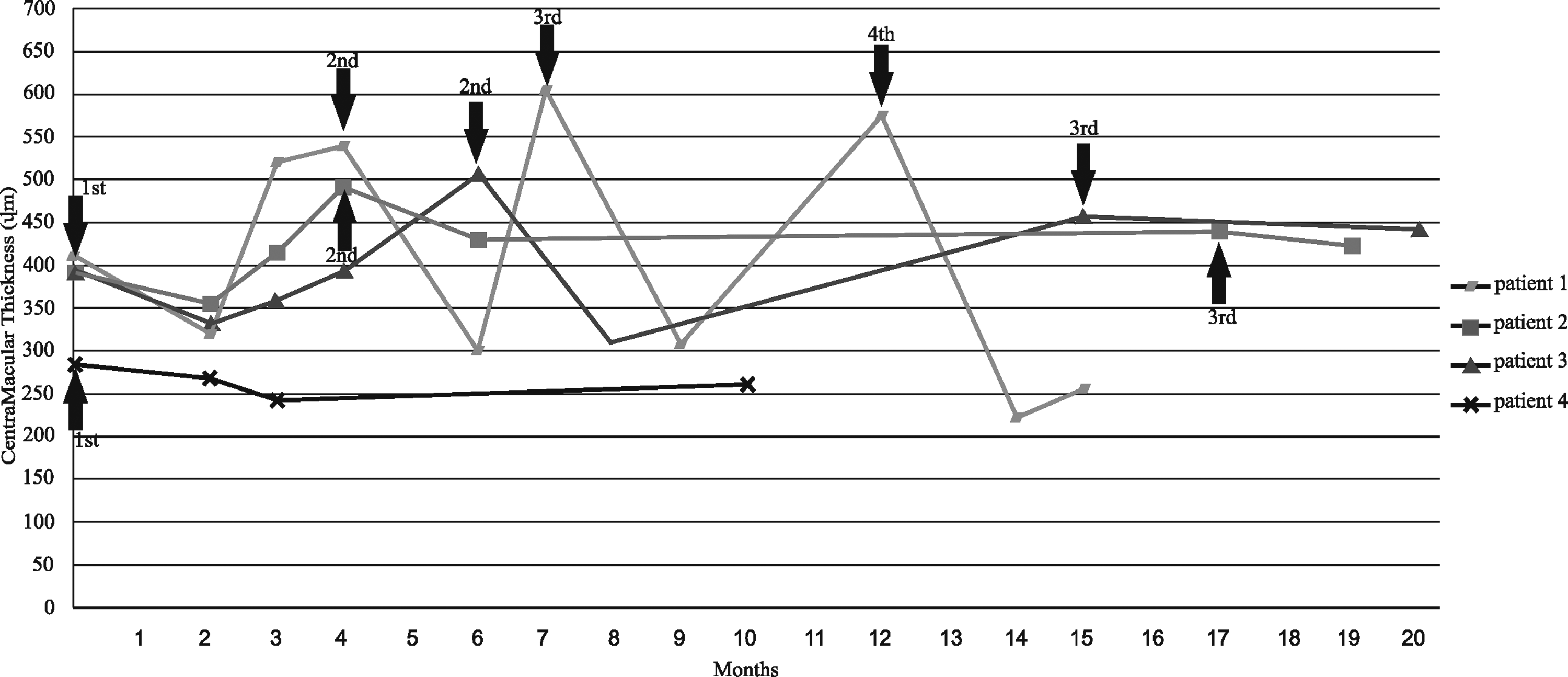
Changes in central macular thickness of all patients during follow-up period.
No serious adverse effects were seen. Two patients (Patient 1 after the first injection and Patient 3 after the second injection) had elevated intraocular pressure, which was controlled with a topical antiglaucomatous drug. Same 2 patients developed cataract. Adverse effects and treatments are shown in Table 3.
CEIOL was performed after completion of the study.
CEIOL, cataract extraction with intraocular lens implantation; IOP, intraocular lens; Max, maximum.
Discussion
Type 1 IMT is a vascular pathology, which is characterized by aneurysms and telangiectatic dilatation of capillary network accompanied by macular edema. Although the pathogenesis of the disease is yet to be discovered several treatments have been tried for the resolution of macular edema. Inconsistent results were reported.
Laser photocoagulation is an effective treatment, however, recurrence of macular edema can be seen after the treatment and also proximity of ectatic vessels and aneurysms to the fovea can limit the area of photocoagulation as well.4,12 Some researchers tried to increase the efficacy of this treatment by combinations with intravitreal ranibizumab 10 and subtenon trimcinolone. 5
Intravitreal anti-vascular endothelial growth factors (anti-VEGF) injection is an alternative treatment option. There are many reports involving intravitreal bevacizumab treatment in the literature, however, results are not consistent.13–18 Gamulescu et al. 14 and Koay et al. 17 reported single cases stabilized after 1 injection for 10 months and 3 consecutive injections for 1 year respectively. On the contrary, Takayama et al. 16 reported reduction in macular edema in only 1 among 5 patients after ∼2–3 injections for a follow-up of more than 12 months and also Matsumoto and Yuzawa 15 reported reduction in macular edema in only 1 patient among 4 patients after ∼3–4 injections for a follow-up of 12 months. Moon et al. 13 in their study of 7 cases stated limited effect of bevacizumab.
Several case reports utilizing treatment with intravitreal agents like ranibizumab and aflibercept were published lately.10–12 Requiring frequent injections, recurrences in short terms, 12 and limited effects on macular edema 11 were reported as downsides of this treatments. Terauchi et al. 9 reported 2 cases refractory to intravitreal anti-VEGF and subtenon triamcinolone treatment benefited from pars plana vitrectomy.
Intravitreal steroids were tried in the treatment of type 1 IMT. Intravitreal triamcinolone was shown to be transiently effective. 8 The adverse effects like increase in intraocular pressure and development of cataracts restrict the usage of this treatment and demand caution especially in younger patients. There are 2 case reports in which intravitreal bevacizumab and triamcinolone treatments failed and intravitreal dexamethasone implant was used after the recurrence of macular edema.19,20 Loutfi et al. 19 reported a case with 3 intravitreal dexamethasone injections in 8 months that stabilized 2 weeks after the last injection. Sandali et al. 20 reported stabilization of macular edema for 15 months with 2 intravitreal dexamethasone injections.
The macular edema resulting from microangiopathic changes such as aneurysms and telangiectasia is the main cause of vision loss in type 1 IMT. Stabilizing the vascular structures reduces the macular edema and increases the visual acuity. At this point steroids come forward with their anti-inflamatory and blood retinal barrier stabilizator effects. 21 Slowly releasing dexamethasone implant is a promising treatment for this aspect. In this study intravitreal dexamethasone injection reduced the macular edema and vascular leakage at different levels. Significant decrease in macular edema was observed especially in 1 patient (Patient 1). Other patients showed moderate reduction in CMT. Recurrence of macular edema is a downside of this treatment but recurrence is seen after other kinds of treatments as well. Failure of improvement in the visual acuity can be attributed to permanent damage to the macular retinal cells due to chronic cystoid macular edema. 22
Despite the small sample size and retrospective nature of this study intravitreal dexamethasone implant was observed to be efficient and safe in our patients. However, randomized clinical trials with larger sample sizes are needed for further evaluation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.