
Abstract
Abstract
Purpose:
The use of sutureless clear corneal incisions (CCIs) for phacoemulsification is an established surgical technique, but the dynamic morphology of the wound and poor construction can lead to an increased risk of postoperative endophthalmitis. Stromal hydration with balanced salt solution (BSS) can improve the self-sealing status. Intracameral cefuroxime has reduced endophthalmitis rates. This study investigates the safety profile of stromal hydration with cefuroxime, as sequestering antibiotic at the wound may potentially provide added protection against infection.
Methods:
MF-1 mice underwent bilateral CCI, followed by stromal hydration with 5 μL of 10 mg/mL cefuroxime, cefuroxime-texas red conjugate (for detection using confocal microscopy), or BSS. Corneas were harvested from 1 h to 12 weeks postoperatively; gross morphology, histology, and apoptotic cell death levels were investigated to determine the safety profile. Bactericidal activity of cefuroxime was assayed using homogenized whole cornea following stromal hydration at 1 h, 24 h, and day 7 against gram-negative Escherichia coli.
Results:
Cefuroxime stromal hydration did not alter corneal morphology, with no evidence of corneal scarring or vascularization. Corneal histology and levels of apoptosis were minimal and comparable to the BSS groups up to 12 weeks. Confocal microscopy detected cefuroxime-texas red up to 1 week surrounding the corneal wound. Whole corneal tissue homogenates displayed bactericidal activity up to 24 h postoperatively.
Conclusions:
Stromal hydration of CCI with cefuroxime is safe in mouse corneas. A reservoir of antibiotic at the wound can potentially act as a barrier of defense against infection following cataract and associated ocular surgery.
Introduction
C
In 2007, the European Society of Cataract & Refractive Surgeons (ESCRS) Endophthalmitis Study Group reported that the use of intracameral cefuroxime at the end of surgery significantly reduced the occurrence of postoperative endophthalmitis. 10 The Cochrane review on perioperative antibiotics for prevention of acute endophthalmitis after cataract surgery found the results of the ESCRS study, the only prospective and randomized multicenter clinical trial, to provide the best evidence for antibiotic prevention of endophthalmitis. 1 In a recent survey investigating the adoption of intracameral antibiotic prophylaxis by 193 ophthalmic surgeons affiliated with private and public hospitals and clinics across Europe, 74% reported they always or usually used intracameral antibiotics (of which 82% used cefuroxime) in their cataract procedures. 11
Cefuroxime is a bactericidal β-lactam second-generation cephalosporin. It acts by binding to specific penicillin-binding proteins, which subsequently interfere with the peptidoglycan synthesis of the bacterial cell wall. 12 Cell lysis ensues following activation of bacterial cell wall autolytic enzymes such as autolysins. Cefuroxime is effective against aerobic gram-positive microorganisms (Staphylococcus aureus, Streptococcus pneumoniae, and Streptococcus pyogenes); aerobic gram-negative microorganisms (Escherichia coli, Haemophilus parainfluenzae, Klebsiella pneumoniae, Moraxella catarrhalis, Haemophilus influenzae, and Neisseria gonorrhoeae, including β-lactamase-producing strains); and spirochetes such as Borrelia burgdorferi.
Safe perioperative measures that can be implemented as prophylaxis against intraocular microbial contamination may further reduce the rates of postoperative endophthalmitis. In this study, we suggest that stromal hydration of CCIs using cefuroxime may provide a safe and effective method of sequestering therapeutic levels of antibiotic at the wound site, with the potential of providing another barrier of defense against infection.
Methods
Animals
Six-week-old MF-1 albino mice (from Harlan UK) were used in this study. They were maintained in a 12-h light–12-h dark cycle with free access to water and food at the Imperial College London animal facility according to standard protocols and the guidelines of the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research. The local institutional review board approved this study.
Before performing surgical CCIs and stromal hydration, the mice were anesthetized by intramuscular injection (0.01 mL/10 g body weight) of a mixture of 100 mg/mL ketamine hydrochloride (Narketan-10; Vétoquinol UK Ltd.), 1 mg/mL medetomidine hydrochloride (Domitor®; Orion Pharma), and double distilled water at a ratio of 3:5:42, respectively. The anesthesia was later reversed by the intramuscular injection (0.01 mL/10 g of body weight) of 0.1 mg/mL atipamezole hydrochloride (Antisedan®; Orion Pharma). At the end of the follow-up period (1 h, 24 h, and weeks 1, 6, and 12 postoperatively), the mice were euthanized by intraperitoneal injection of an overdose (80–90 mg/kg body weight) of sodium pentobarbital (Euthatal; Merial Animal Health Ltd.). The eyes were then enucleated and the corneas excised. Nonoperated corneas were used as the negative control.
CCI and stromal hydration
The cornea was lubricated with a drop of Hypromellose 0.3% w/v (Martindale Pharma®, chemical name hydroxypropyl methylcellulose C56H108O30) and excess fluid removed using a spear-shaped sponge (Harvard Apparatus). A 0.6 mm CCI was then placed in the temporal aspect of each cornea using an incisional micrometer diamond knife (DGH Technology Ltd.). Intracorneal stromal hydration through the lips of the wound was performed using a 34-gauge Hamilton needle mounted onto polyethylene tubing (Intramedic™) and a gas-tight 50 μL Hamilton glass barrel. The right corneal stroma was hydrated with 5 μL of 1 mg/0.1 mL (or 10 mg/mL) cefuroxime solution. The left eye was hydrated with 5 μL BSS© (Alcon Laboratories) to serve as a control.
Cefuroxime and cefuroxime-Texas Red®-X conjugate
Cefuroxime sodium powder (GlaxoSmithKline) was dissolved in BSS (Alcon Laboratories) to a concentration of 1 mg/0.1 mL (or final concentration 10 mg/mL). This was made up fresh for each application. To assess sequestration of cefuroxime at the site of the CCI following stromal hydration, confocal microscopy was used to monitor the presence of cefuroxime-Texas Red®-X conjugate. To prepare the conjugate, 0.3 mL of 2 mg/mL stock solution of Texas Red®-X succinimidyl esters (Invitrogen Molecular Probes) dissolved in DMSO was agitated with 2.2 mL of cefuroxime (50 mg/mL stock) overnight at 4°C in the dark. This preparation was diluted with double-distilled water to a concentration of 10 mg/mL cefuroxime-Texas Red-X and 5 μL was used to stromally hydrate the cornea; and 5 μL of 10 mg/mL Texas Red-X alone was also injected into the corneal stroma as a control. Stacked images of the cornea were taken using the Leica SP5 inverted confocal microscope at 1 h, 24 h, and day 7. Total fluorescence intensity was measured (using Leica LAS AF Lite software) from each dissected cornea, n = 3 at each aforementioned time point, providing a mean ± standard error of the mean fluorescence intensity per cornea for each treatment group.
Bactericidal assay
To determine the bactericidal activity of cefuroxime, harvested corneas at 1 h, 24 h, and day 7 poststromal hydration were homogenized by sonication (3 × 15 s, XL-2000 Qsonica LLC) and the whole tissue homogenate was added to 50 μL gram-negative bacteria E. coli DH5α cells incubated with 5 mL Luria-Bertani medium overnight at 37°C (n = 3 corneas per time point). BSS-hydrated corneas at corresponding time points were used as the negative control, alongside untreated corneas (n = 3). Direct inoculation of 5 μL of 10 mg/mL cefuroxime was used as a positive control. Following this, 10 μL of each culture was plated on agar plates overnight at 37°C to assess levels of bactericidal activity. The number of colony-forming units (CFU) per milliliter was calculated by counting each colony on 3 agar plates per condition, using a Molecular Imager (Gel-Doc XR; Bio-Rad Laboratories), and determining the mean colony count per milliliter plated, divided by the total dilution factor.
Corneal histology and morphological studies
Freshly excised corneas were fixed in 4% paraformaldehyde (PFA) for 4–6 h at room temperature, then washed thrice in phosphate-buffered saline, dehydrated through a graded ethanol series (50%, 70%, 90% and 3 times in 100%), and finally embedded in paraffin wax. Microtome sections of 5 μm were cut, mounted on Superfrost Plus slides, and stained with hematoxylin and eosin.
Corneal morphology and histology at various time points between 5 min and 12 weeks were taken using a Nikon 5100 mounted on a Stemi 2000 C 7:1 zoom stereomicroscope. The central corneal thickness (CCT) was measured from the histological sections using ImageJ, and mean CCT ± SEM (n = 3 at each time point per treatment group) was calculated.
TUNEL assay
Excised corneas with cefuroxime and BSS stromal hydration were fixed in 4% PFA and embedded in wax as described above at 1 h, and weeks 1, 6, and 12 postoperatively (n = 3 at each time point per treatment group). Corneal sections were dewaxed by washing twice in histoclear (National Diagnostics), followed by 2 washes in 100% ethanol and once in 70% ethanol, before rinsing in deionized H2O. Sections were digested with proteinase K (10 mg/mL) for 15 min. Following the manufacturer's instructions, the ApopTag® Peroxidase In Situ Apoptosis Detection Kit (Millipore) was used to detect levels of apoptotic cell death to determine the safety profile of the stromal hydration.
Statistical analysis
All results are expressed as mean ± SEM, unless specified. As sample sizes are small, nonparametric tests were used. Differences between control nonoperated and BSS- and cefuroxime-hydrated groups were assessed by pair-wise comparisons using the Mann–Whitney test or the Kruskal–Wallis analysis of variance if more than 2 groups were investigated, followed by Dunn's multiple comparison test where appropriate, unless otherwise stated. A P-value of <0.01 was considered statistically significant.
Results
Stromal hydration of CCI with a 10 mg/mL concentration of cefuroxime did not adversely affect the cornea using an in vivo mouse model. The right and left eyes were stromally hydrated with 5 μL of 10 mg/mL cefuroxime and 5 μL of BSS, respectively. This volume of solution was chosen for intrastromal hydration as it maximally hydrated the wound edges. Corneal morphology was comparable in both cefuroxime and BSS hydration groups at each time point from 1 h to 6 weeks (Fig. 1A). By week 6, there was no gross morphological difference in appearance between operated and nonoperated eyes. There was no evidence of corneal scarring or vascularization up to 12 weeks postoperatively.

Morphology, histology, and cell death assay comparing stromal hydration of a clear corneal incision with CEF (10 mg/mL) or BSS in the mouse eye postoperatively.
Levels of apoptosis were assayed using TUNEL staining in both BSS and cefuroxime stromal hydration groups up to 12 weeks postoperatively. From day 1 through week 12, there was minimal evidence of cell death, and each cornea was comparable in both groups to a nonoperated eye (Fig. 1C).
Corneal histology showed an increase in corneal thickness at 1 h poststromal hydration in both the BSS (mean 121.3 ± 2.6 μm) and cefuroxime (mean 121.0 ± 1.6 μm) groups. Each group had a comparable CCT at each time point investigated (Fig. 2), with no statistical difference (P > 0.95): at 1 week postoperatively, the mean CCT was 98.0 ± 1.4 μm in the BSS and 96.3 ± 1.2 μm in the cefuroxime group; at 6 weeks postoperatively, the mean CCT was 93.7 ± 2.6 μm in the BSS and 92.0 ± 2.1 μm in the cefuroxime group; and at 12 weeks, the mean CCT was 87.3 ± 2.1 μm in the BSS and 88.3 ± 1.7 μm in the cefuroxime group similar in thickness to an untreated cornea, mean CCT was 87.7 ± 1.69 μm (no statistical difference, P > 0.98).
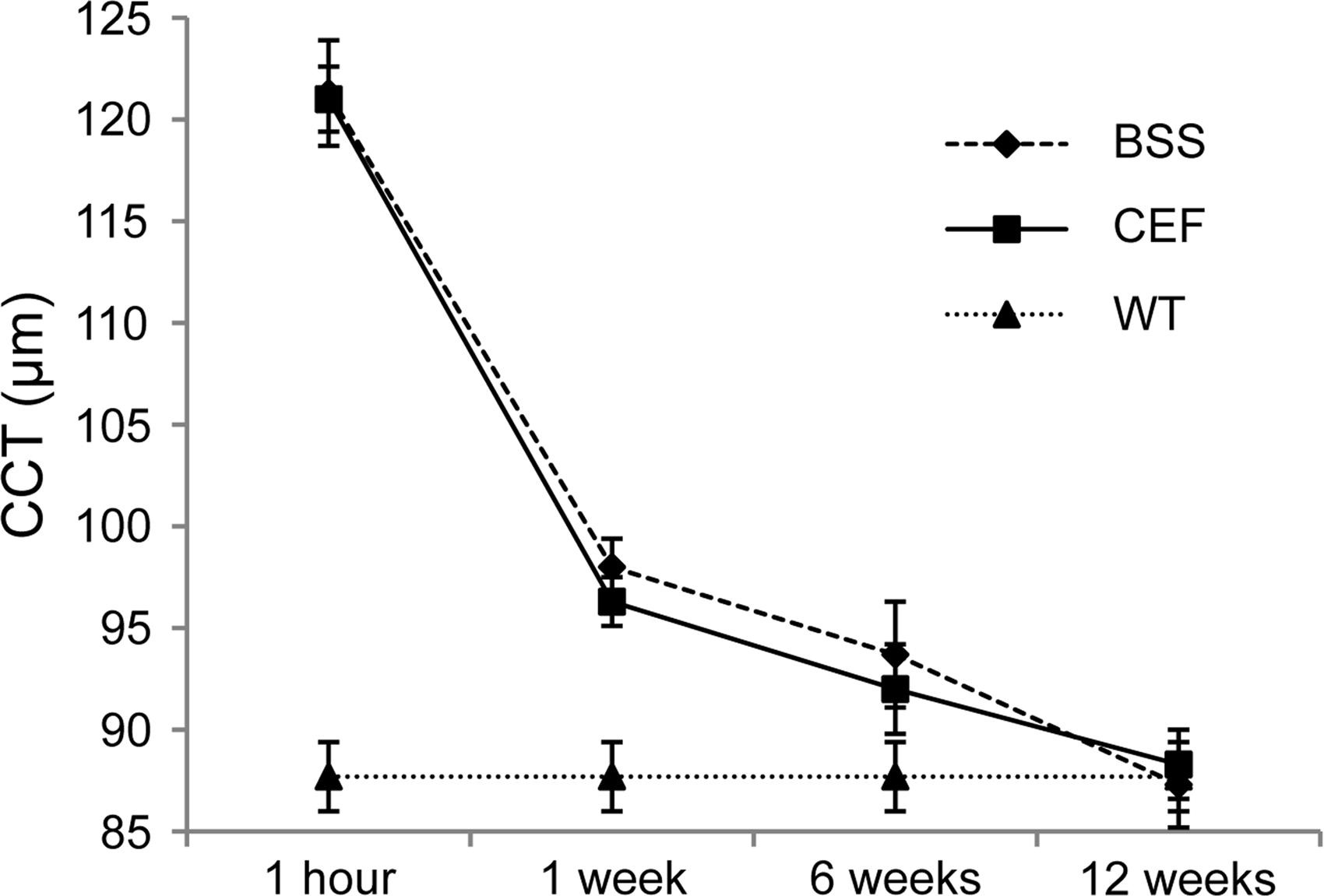
Graphical representation showing the mean ± standard deviation reduction in CCT (in μm) following stromal hydration with CEF (10 mg/mL) or BSS over time postoperatively from 1 h up to 12 weeks (n = 3 per time point per group; WT, control nonoperated eye). CCT, central corneal thickness.
Cefuroxime-texas red conjugate and texas red alone were detected by confocal microscopy up to 1 week surrounding the corneal wound (Fig. 3). Cumulative levels of fluorescence were measured from stacked images of each dissected cornea stromally hydrated with cefuroxime-texas red (mean 42.5 × 105 ± 4.4 × 104 fluorescence intensity/cornea) and texas red alone (mean 35.1 × 105 ± 4.0 × 104 fluorescence intensity/cornea) at 1 h postoperatively. This dropped by 42.1% by day 1 postoperative in the cefuroxime-texas red group (mean 17.9 × 105 ± 5.2 × 104 fluorescence intensity/cornea) and 42.7% in the texas red group (mean 15.0 × 105 ± 8.0 × 103 fluorescence intensity/cornea). At 1 week postoperatively in the cefuroxime-texas red group (mean 4.1 × 105 ± 1.6 × 104 fluorescence intensity/cornea), less than 10% fluorescence intensity was detected compared to the 1 h postoperative time point. This was similar in the texas red group (mean 3.6 × 105 ± 8.0 × 103 fluorescence intensity/cornea). No fluorescence was seen in the BSS-hydrated corneas, which were used as the negative control.
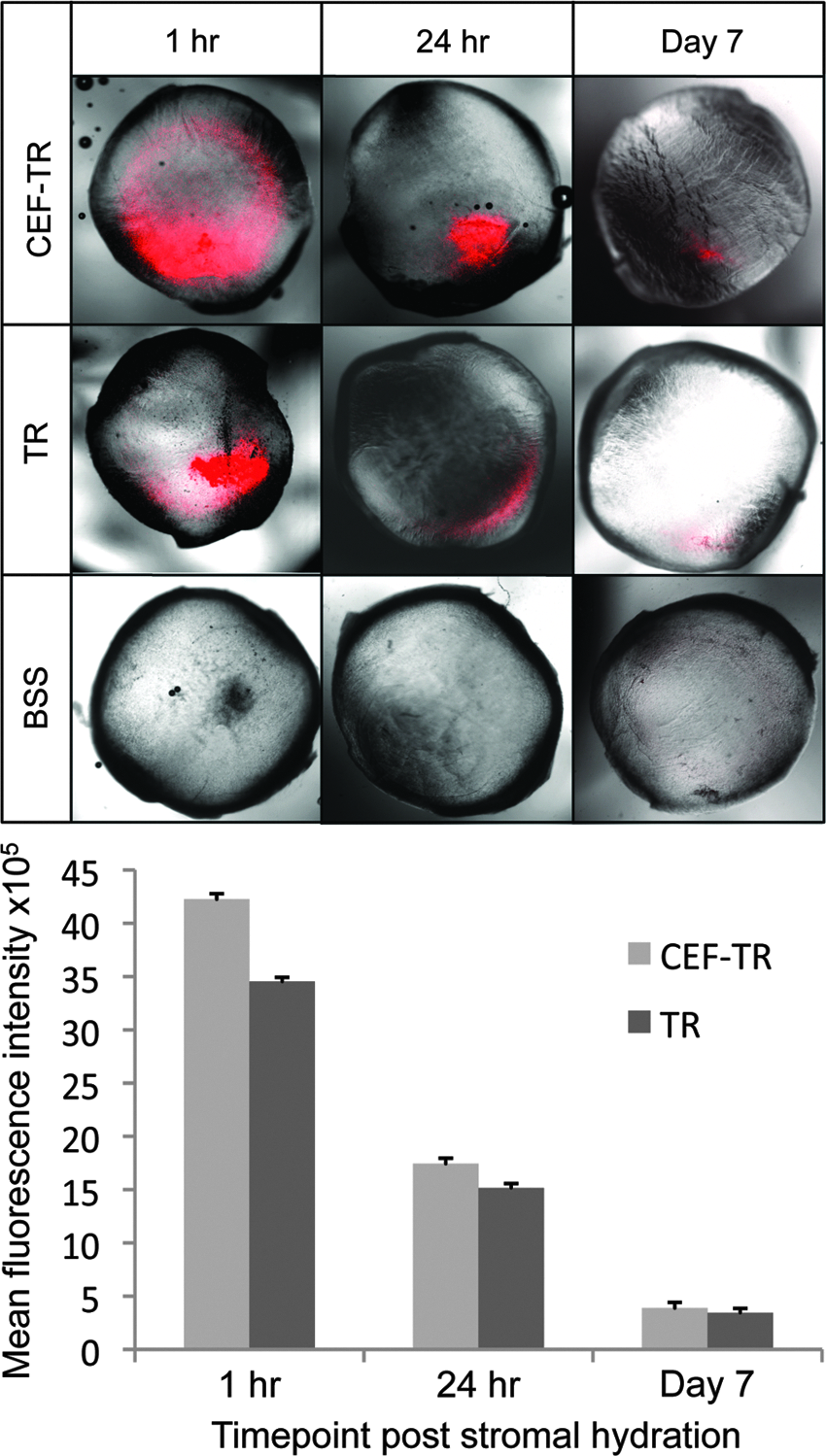
Fluorescence levels of cefuroxime-texas red conjugate following stromal hydration of the corneal wound. Stacked confocal fluorescence merged with bright field images of the cornea hydrated with CEF-TR conjugate, TR alone, and BSS at 1 h, 24 h, and day 7 postoperatively. Corresponding graph showing the mean fluorescence intensity × 105 per whole cornea ± standard error of the mean (n = 3 per time point per group) of CEF-TR and TR. CEF-TR, cefuroxime-texas red; TR, texas red. Color images available online at www.liebertpub.com/jop
Microbiological tests to assess the bactericidal activity of cefuroxime in the stromally hydrated cornea showed a significant efficacy at 1 h postprocedure (2.1 × 106 ± 4.8 × 106 CFU/mL) compared to the BSS-hydrated corneas at the same time point (7.6 × 108 ± 3.2 × 107 CFU/mL) and nonoperated cornea controls (7.7 × 108 ± 1.3 × 107 CFU/mL), P < 0.01 (Fig. 4). Although less than at 1 h, a significant degree of bactericidal activity was still seen at 24 h (2.4 × 108 ± 2.7 × 107 CFU/mL) compared to the BSS-hydrated corneas (7.5 × 108 ± 4.1 × 107 CFU/mL) and negative control group, P < 0.01. By day 7, there was no difference in cefuroxime-hydrated corneas (7.4 × 108 ± 3.9 × 107 CFU/mL) compared to the BSS-hydrated corneas (7.2 × 108 ± 6.6 × 107 CFU/mL) and nonoperated cornea controls, P < 0.95. When 5 μL of 10 mg/mL cefuroxime was added directly to the E. coli DH5α cells, no growth was seen in the agar plates, suggesting that this dose is bactericidal and optimum for administration into the eye (Fig. 4).
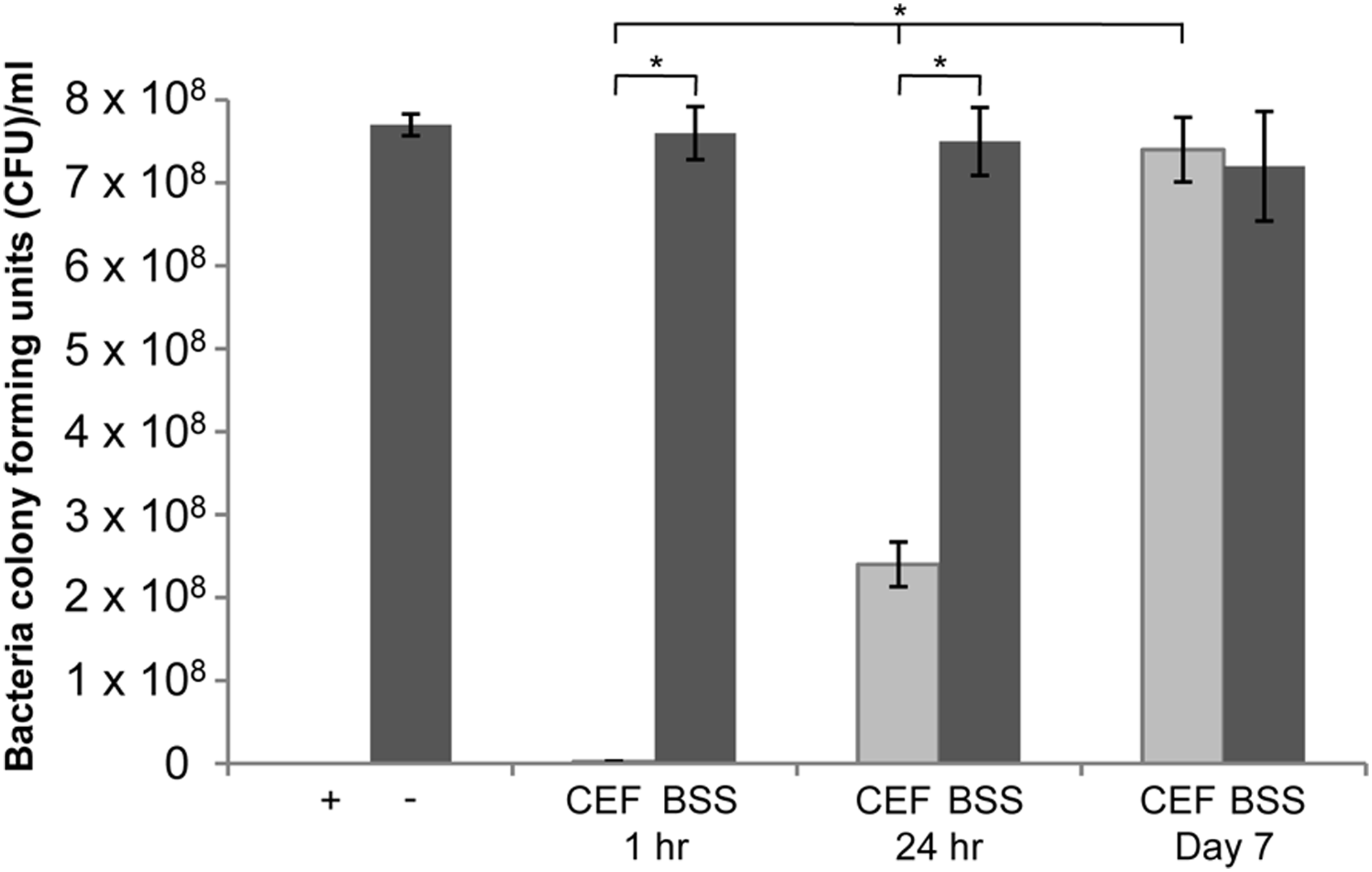
Graph to show the levels of bacteria (CFU/mL) following inoculation with cefuroxime stromally hydrated corneas (CEF) compared to BSS-hydrated corneas (BSS) at 1 h, 24 h, and day 7 postoperatively. Negative control (−) was nonoperated cornea and the positive control (+) was 5 μL of 10 mg/mL cefuroxime. CFU, colony-forming units.
Discussion
Stromal hydration of CCI with 10 mg/mL cefuroxime appears safe in mouse corneas with demonstrable levels up to 7 days postoperatively. This is consistent with a recent study, which found that stromal hydration is detectable for at least 1 week in patients undergoing cataract surgery performed through CCI, confirmed by 3D corneal and anterior segment optical coherence tomography (OCT). 13 Fine et al. used a Zeiss Visante anterior segment OCT to detect stromal swelling at 24 h postcataract surgery, but did not examine any later timepoints. 14 A reservoir of antibiotic at the wound could act as a barrier of defense against infection, with the potential to reduce the risk of postoperative endophthalmitis following cataract and associated ocular surgery.
Pharmacokinetic studies have shown that cefuroxime is excreted unchanged in the urine and has a half-life of 1–2 h. 15 A nonrandomized observer-masked trial was conducted to investigate the safety and kinetics of prophylactic intracameral cefuroxime in patients who underwent uneventful phacoemulsification. 16 Patients received a dose of 1 mg cefuroxime in 0.1 mL saline 0.9% into the anterior chamber at the end of surgery. One hour later, following aqueous sampling, a 4-fold reduction in the levels of cefuroxime was detected from 2.74 to 0.75 mg/mL. No further time points were measured and as there were no reports of aqueous turnover following cataract surgery, the true elimination rate could not be fully ascertained. From our study, the detection of cefuroxime-texas red conjugate and the corresponding bactericidal activity up to 24 h suggests that adequate concentrations of cefuroxime were present in the cornea following surgery. Bacterial colonies were detected at both time points, compared to the direct administration of cefuroxime to the gram-negative bacteria E. coli, but this is likely due to the dilution effect caused by using the whole cornea tissue homogenate. Nonetheless, presence of low levels of antibiotic had some inhibitory action on the growth of bacteria, and in practice, if concentrated around the wound edges will have a more potent protective effect. The main limitation of this study is the lack of serial drug level monitoring in the stroma, anterior chamber, and tears. Further studies are warranted to measure the release of cefuroxime from the stroma to the aqueous humour and into the tears over time to determine the true elimination rate from the cornea and whether its minimum inhibitory concentration levels could be achieved for S. epidermidis and other relevant bacteria associated with endophthalmitis.
A recent study investigated the penetration of bevacizumab administered to BALB/c mouse eyes topically with a denuded corneal epithelium or through subconjunctival injection with an intact cornea. 17 At 24 h postadministration, there was evidence of widespread intracorneal diffusion with even stromal distribution throughout the whole cornea using both methods. Bevacizumab remained present in the central cornea for up to 14 days, declining at 21 days from the periphery. Due to its large molecular weight, 149 kDa, it was hypothesized that bevacizumab was removed by diffusion from the corneal periphery in a centripetal pattern slowly over weeks. In contrast, cefuroxime is a small molecule, formula C16H16N4O8S, with a molecular mass of 424.386 Da, but this compound may act in a similar manner reducing in levels through diffusion secondary to its high concentration gradient in the stroma over time. Stromal hydration with cefuroxime would allow a known concentration of drug to be delivered to the cornea, which could act as a slow-release mechanism at the wound site and into the anterior chamber. In theory, stromal hydration may be useful for patients where compliance may be an issue, as a bolus may cover the patient over the first few days up to 1 week postoperatively.
There has been a reluctance to adopt the use of intracameral antibiotics, namely cefuroxime (0.1 mL of 10.0 mg/mL solution), over the past few years despite its result in a 5-fold reduction in the incidence of postoperative endophthalmitis. Fifty-five percent of surgeons surveyed in the United Kingdom in 2008 reported using intracameral cefuroxime, compared with 10% in 2005. 18 The unwillingness was mainly due to the concern of unintended dilution errors, endothelial toxicity, and possible bacterial contamination. Previously, there were no ready-to-use ocular formulations of cefuroxime available, hence the 10 mg/mL solution was prepared in hospital pharmacies and stored at 4°C for a limited time or reconstituted by the surgeon in the operating room, which risked mistakes during the dilution. A series of 6 cases was published by Delyfer et al. documenting the inadvertent administration of high-dose (100 mg/mL) intracameral cefuroxime at the end of an uneventful cataract surgery, secondary to misunderstanding of the dilution protocol. 19 Each case resulted in moderate anterior inflammation and fibrin formation consistent with a mild form of toxic anterior segment syndrome or toxic endophthalmitis, which had resolved by day 5. All patients developed extensive macular edema with an associated serous retinal detachment on day 1 postoperatively, which significantly improved in the first week. At 6 weeks CCT, endothelial cell density (ECD) and macular anatomy had returned to normal in all patients consistent with those observed after an uneventful phacoemulsification. Two-thirds of the surgeons not using intracameral cefuroxime stated that they would adopt this step if a commercial preparation was available. 18 A 1-step reconstitution of cefuroxime (Aprokam®) is now available and this may encourage the use of intracameral cefuroxime and its further application in stromal hydration of the cornea. 20 However, a prefilled single-use syringe containing 10 mg/mL cefuroxime would be ideal to eliminate any preparation and dosage errors.
Our experiments show that there were minimal levels of cell death in the cefuroxime and BSS stromal hydration groups, both comparable to nonoperated eyes. There have been many studies assessing the corneal endothelial changes after intracameral cefuroxime following cataract surgery. In a recent study, ECD, coefficient of variation (CoV), and hexagonality were evaluated at baseline and 1 week, 1 month, and 3 months following intracameral cefuroxime (1 mg/0.1 mL) or vancomycin (1 mg/0.1 mL) after cataract surgery. 21 The ECD was significantly reduced at 1 week postsurgery, after which it stabilized, but overall it decreased by a mean of 12.1% at 3 months. There was no significant difference in the CoV or hexagonality preoperatively and at 3 months postoperatively.
There has been little advance in perioperative techniques for the prevention of acute endophthalmitis over recent years. Before the 2007 ESCRS Endophthalmitis Study, which demonstrated the efficacy of using intracameral antibiotics for reducing endophthalmitis, only preoperative disinfection by povidone–iodine could reach the level II rating of scientific evidence.1,22 Other reported prophylactic interventions, such as antibiotic-containing irrigating solutions and the use of intraoperative heparin and postoperative subconjunctival antibiotic injection, received the lowest clinical recommendation based on weak evidence justifying their use. 22 This preclinical study shows proof-of-concept for developing a new perioperative prophylactic intervention, which uses the same concentration of intracameral cefuroxime for stromal hydration of the surgical wounds. Anectodotally, this technique is in use by some cataract surgeons, however, the method has not been previously published in the literature. There is contention about the transferability of mouse corneal data to humans, but this study does confirm the safety of cefuroxime intrastromal hydration in murine models. Clinical trials would be required to assess the safety in patients with a view to evaluating this procedure using large patient groups to compare rates of postoperative endophthalmitis following cataract surgery.
Footnotes
Acknowledgments
We would like to acknowledge the National Institute for Health Research UK (Moorfields Eye Hospital and UCL Institute of Ophthalmology Biomedical Research Centre) and the Eli Webster Ophthalmic Charity Fund, Charing Cross Hospital, London, United Kingdom.
Author Disclosure Statement
No competing financial interests exist.