
Abstract
Abstract
Purpose:
To evaluate the long-term outcome of intravitreal bevacizumab treatment for idiopathic choroidal neovascularization (CNV) and to investigative the influence of CNV recurrence on visual prognosis.
Methods:
This retrospective study included 26 patients (26 eyes) who had been diagnosed with idiopathic CNV and followed up for at least 2 years. All the eyes included had been treated with intravitreal bevacizumab. The best-corrected visual acuity (BCVA) at diagnosis was compared with that at final follow-up. The final BCVA of patients who experienced CNV recurrence was compared with that of patients who did not.
Results:
The mean follow-up period after diagnosis was 33.9 ± 10.6 months. During this period, a mean of 2.5 ± 1.7 bevacizumab injections were administered. The mean logarithm of the minimal angle of resolution (logMAR) BCVAs at diagnosis, 6 months, 12 months, and final follow-up was 0.48 ± 0.38, 0.28 ± 0.36, 0.25 ± 0.35, and 0.20 ± 0.26, respectively. The final BCVA was significantly improved over the baseline value. CNV recurred in 8 patients (30.8%), 3 of whom experienced 2 recurrences; the mean timing of recurrence was 19.7 ± 15.5 months after diagnosis. The final BCVA in patients who experienced recurrence (mean 0.21 ± 0.19 logMAR) did not differ from that in patients who did not (mean 0.19 ± 0.29 logMAR).
Conclusions:
The long-term outcome of intravitreal bevacizumab treatment for idiopathic CNV was generally favorable. Although CNV recurrence was noted in 30.8% of patients, the recurrence may not significantly influence long-term visual prognosis.
Introduction
I
Intravitreal antivascular endothelial growth factor (VEGF) therapy is a widely used treatment for CNV. Although the therapy was originally developed to treat CNV secondary to AMD,3,4 it is also effective in idiopathic CNV. Anti-VEGF therapy for idiopathic CNV can significantly improve visual acuity and involves fewer injections than does anti-VEGF treatment for CNV secondary to AMD.5–11 In addition, anti-VEGF therapy is more efficacious than photodynamic therapy (PDT). 9 However, one limitation of previous studies is that the follow-up period has generally been limited to 1 year or less.5–8 Only few studies have investigated 2-year treatment outcome. 9 In addition, the long-term recurrence rate has not yet been fully elucidated, nor has the influence of recurrence on long-term visual prognosis.
The purpose of this study was to evaluate the long-term outcome of intravitreal bevacizumab treatment for idiopathic CNV. In addition, the timing and incidence of CNV recurrence, as well as its influence on long-term visual outcome were investigated.
Methods
This retrospective, observational case series was performed at a single center. The study was approved by the institutional review board (Kim's Eye Hospital IRB) and was conducted in accordance with the tenets of the Declaration of Helsinki.
This study included patients who had been diagnosed with treatment-naive idiopathic CNV between January 2010 and May 2013 and had been treated using intravitreal bevacizumab monotherapy. All subjects had undergone a comprehensive initial ophthalmological examination that included measurement of best-corrected visual acuity (BCVA), 90-diopter (D) lens slit-lamp biomicroscopy, fundus photography, fluorescein angiography, spectral domain optical coherence tomography (OCT, Spectral OCT/SLO®; OTI Ophthalmic Technologies, Inc.), and indocyanine green angiography (ICGA) performed using a confocal laser-scanning system (HRA-2; Heidelberg Engineering GmbH). Exclusion criteria were <2-year follow-up, ≥50 years of age, −6.0 D or greater myopia, axial length of 26.0 mm or greater, severe medial opacity, history of ocular trauma or refractive surgery, or concomitant retinal disorders (e.g., AMD, intraocular inflammation, chorioretinal scar, angioid streak, central serous chorioretinopathy, macroaneurysms, proliferative diabetic retinopathy, and central retinal vascular occlusion). Two examiners (Y.S.C. and J.H.K.) analyzed the ICGA results; polypoidal lesions, with or without branching vascular networks, were considered indicative of polypoidal choroidal vasculopathy. Such cases were also excluded from the study.
Central foveal thickness was defined as the distance at the fovea between the internal limiting membrane and Bruch's membrane, and was manually measured using the calipers tool in an OCT software program. The greatest linear dimension of the lesion was measured on the fluorescein angiography images.
All eyes had initially been treated with 1–3 monthly intravitreal bevacizumab (Avastin®; 1.25 mg/0.05 mL; Genentech) injections. The OCT was performed 1 month after the initial treatment, and additional injections were administered to patients in whom intraretinal/subretinal fluid remained. Once the fluid had completely subsided, patients were scheduled to visit the hospital once every 1–4 months, at the discretion of the treating physician. Recurred intraretinal/subretinal fluid exudate or retinal/subretinal hemorrhages, detected using OCT and fundus examination, were retreated using intravitreal bevacizumab.
The baseline BCVA was compared with that at 6 months, 12 months, and final follow-up. The BCVAs were converted to logarithm of the minimal angle of resolution (logMAR) values for analysis. Associations of final BCVA with the following factors were evaluated: age, greatest linear dimension, BCVA at diagnosis, central foveal thickness at diagnosis, duration of follow-up, and number of initial bevacizumab injections. In addition, eyes were classified into 2 groups on the basis of the CNV location: (1) subfoveal CNV and (2) juxtafoveal CNV. The final BCVA was compared between these 2 groups. Multivariate analysis was performed using the following variables to identify factors predictive of final visual outcome: age, greatest linear dimension, BCVA at diagnosis, central foveal thickness at diagnosis, duration of follow-up, proportion of patients receiving 3 loading injections, and location of lesion.
The eyes were classified into 2 groups: (1) eyes with CNV recurrence and (2) eyes without it. Various characteristics were compared between these 2 groups: age, location of the lesion, greatest linear dimension, BCVA at diagnosis, central foveal thickness at diagnosis, number of patients receiving 3 loading injections, and follow-up period. To evaluate the influence of CNV recurrence on the final visual outcome, BCVA at final follow-up and degree of change in BCVA during the follow-up period were compared between the 2 groups.
Statistical analyses were performed using a commercially available software package (SPSS ver. 12.0 for Windows; SPSS, Inc.). BCVA differences among the 4 time points were analyzed using repeated-measures analysis of variances. Differences between 2 groups were analyzed using either the Mann–Whitney U test or Fisher's exact test. Associations between factors were evaluated using Pearson's correlation analysis and multiple linear regression analysis. A P value of <0.05 was considered significant.
Results
Twenty-six consecutive patients (11 men, 15 women; 26 eyes) were included in the study (Table 1). The mean age was 40.9 ± 7.7 (range: 23–48) years. One patient had diabetes mellitus, and 3 had hypertension. Fourteen eyes had been diagnosed with subfoveal CNV and 12 with juxtafoveal CNV. The mean greatest linear dimension was 992.3 ± 239.9 μm. At diagnosis, the mean BCVA was 0.48 ± 0.38 logMAR and the mean central foveal thickness was 337.0 ± 105.4 μm.
BCVA, best-corrected visual acuity; F, female; M, male.
Four patients had received 2 monthly intravitreal bevacizumab loading injections and 7 patients had received 3 monthly injections. In all 11 of these eyes, the fluid had completely subsided after the injections. Fifteen eyes were initially treated with a single bevacizumab injection. In 13 of these eyes, the fluid had completely subsided after a single injection, whereas in 2 eyes, it had partially subsided. One additional injection was administered to these 2 eyes and the fluid had completely subsided 1 month after the second injection. Thus, 13, 6, and 7 eyes had initially been treated with 1, 2, and 3 monthly bevacizumab injections, respectively. The mean number of initial injections was 1.8 ± 0.9.
The mean follow-up period was 33.9 ± 10.6 months (range: 24–56) after diagnosis. During the follow-up period, CNV had recurred in 8 eyes (30.8%, Fig. 1), and 3 of these eyes had experienced 2 recurrences. CNV had recurred a mean of 19.7 ± 15.5 months (range: 7–49) after diagnosis. The 8 eyes with recurrence were additionally treated using 2.4 ± 1.4 bevacizumab injections, and the fluid had completely subsided after additional treatment. As a result, the mean number of injections administered throughout the entire follow-up period was 2.5 ± 1.7.
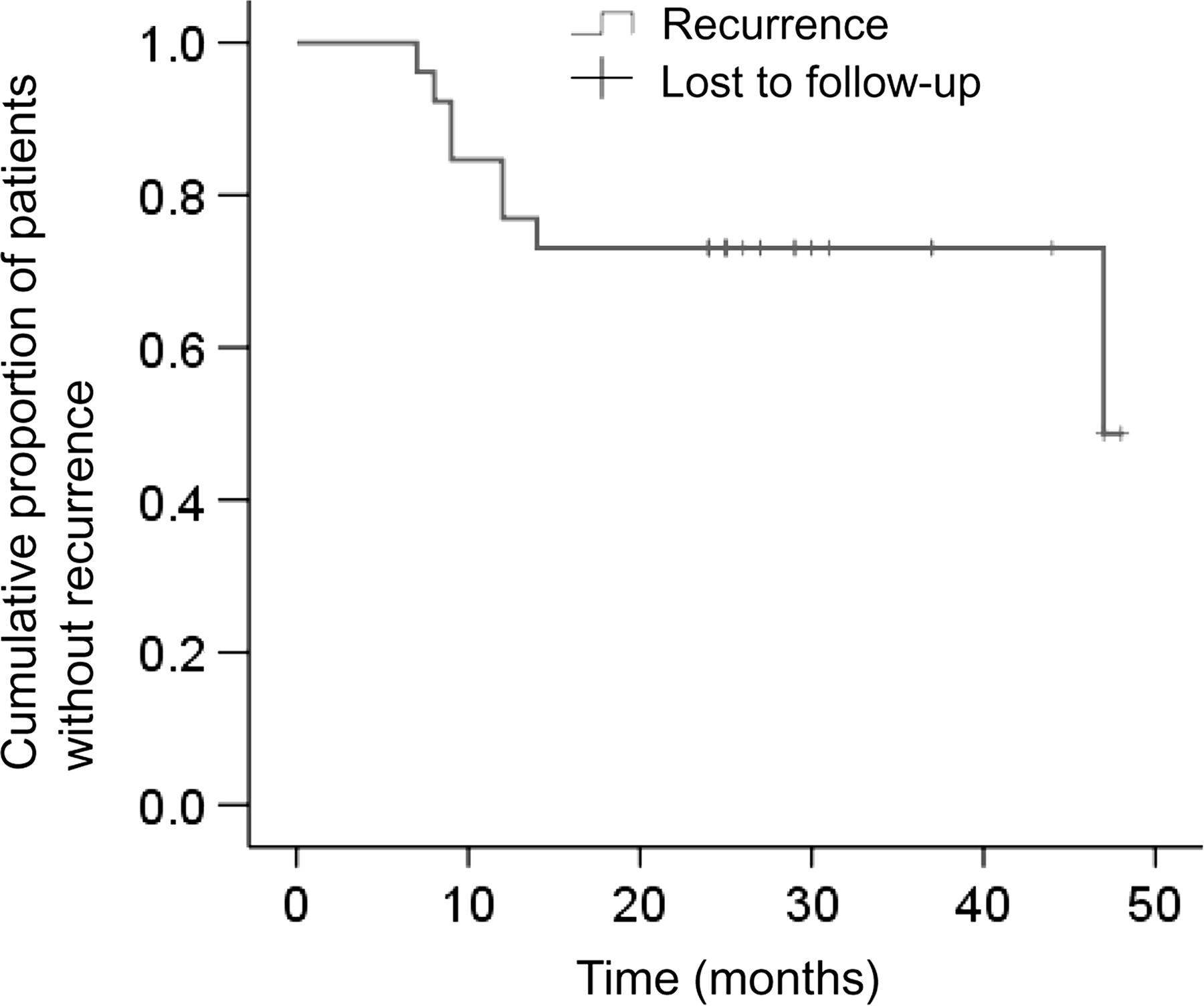
A Kaplan–Meier curve showing the cumulative proportion of patients who did not experience recurrence.
Table 2 summarizes the comparisons between patients with CNV recurrence and those without. The follow-up period in patients with recurrence (40.4 ± 13.0 months) was significantly longer than that in patients without recurrence (30.9 ± 8.1; P = 0.031). There was no difference between patients with recurrence and those without in terms of age (P = 0.605), lesion location (P = 0.202), greatest linear dimension (P = 0.495), BCVA at diagnosis (P = 0.449), central foveal thickness at diagnosis (P = 0.935), and proportion of patients receiving 3 loading injections (P = 0.375).
Statistical analysis performed using the Mann–Whitney U test.
Statistical analysis performed using Fisher's exact test.
BCVA, best-corrected visual acuity.
The mean BCVA at diagnosis, 6 months, 12 months, and final follow-up was 0.48 ± 0.38 logMAR, 0.28 ± 0.36 logMAR, 0.25 ± 0.35 logMAR, and 0.20 ± 0.26 logMAR, respectively (Fig. 2A). The BCVA at 6 months (P < 0.001), 12 months (P < 0.001), and at final follow-up (P < 0.001) had significantly improved over the baseline value. BCVA had improved by ≥0.2 logMAR in 16 eyes (61.5%), and was stable in the remaining 10 (38.5%); it had not deteriorated by ≥0.2 logMAR in any of the eyes. Figure 3 shows a representative case. BCVA at diagnosis was significantly correlated with final BCVA (P < 0.001, r = 0.785; Table 3). However, no other factors analyzed were significantly associated with final BCVA; age (P = 0.689), greatest linear dimension (P = 0.785), central foveal thickness at diagnosis (P = 0.748), duration of follow-up (P = 0.582), and number of initial bevacizumab injections (P = 0.076). When patients were divided into 2 groups on the basis of lesion location, the final BCVA was significantly better in eyes with juxtafoveal lesion (0.08 ± 0.08 logMAR) than in eyes with subfoveal lesion (0.29 ± 0.30 logMAR; P = 0.016). In multivariate analysis, the baseline BCVA was found to be predictive of final visual outcome (P < 0.001).
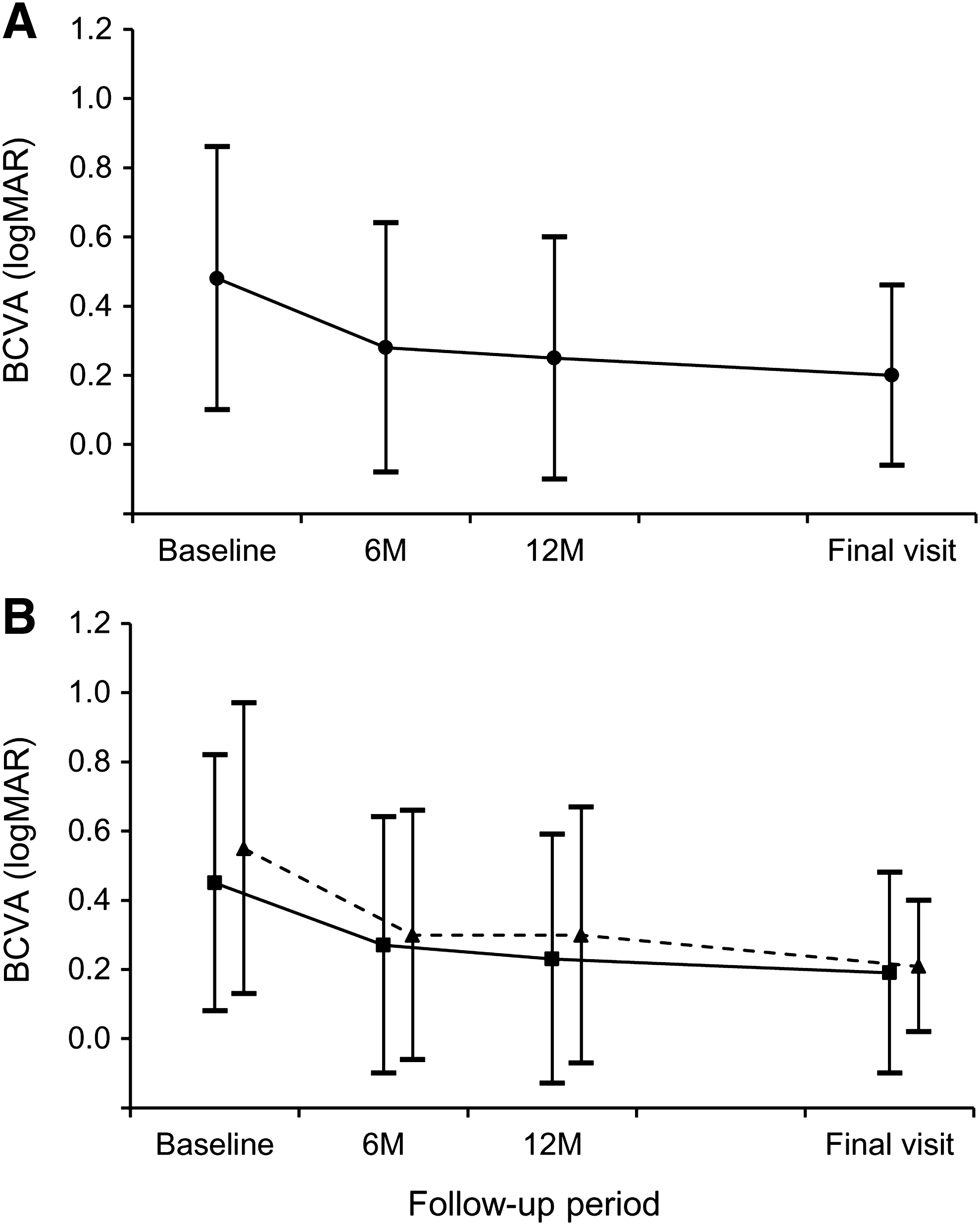
Changes in the logarithm of minimal angle of resolution BCVA during the follow-up period. The final visit occurred at mean 33.7 ± 10.8 months.
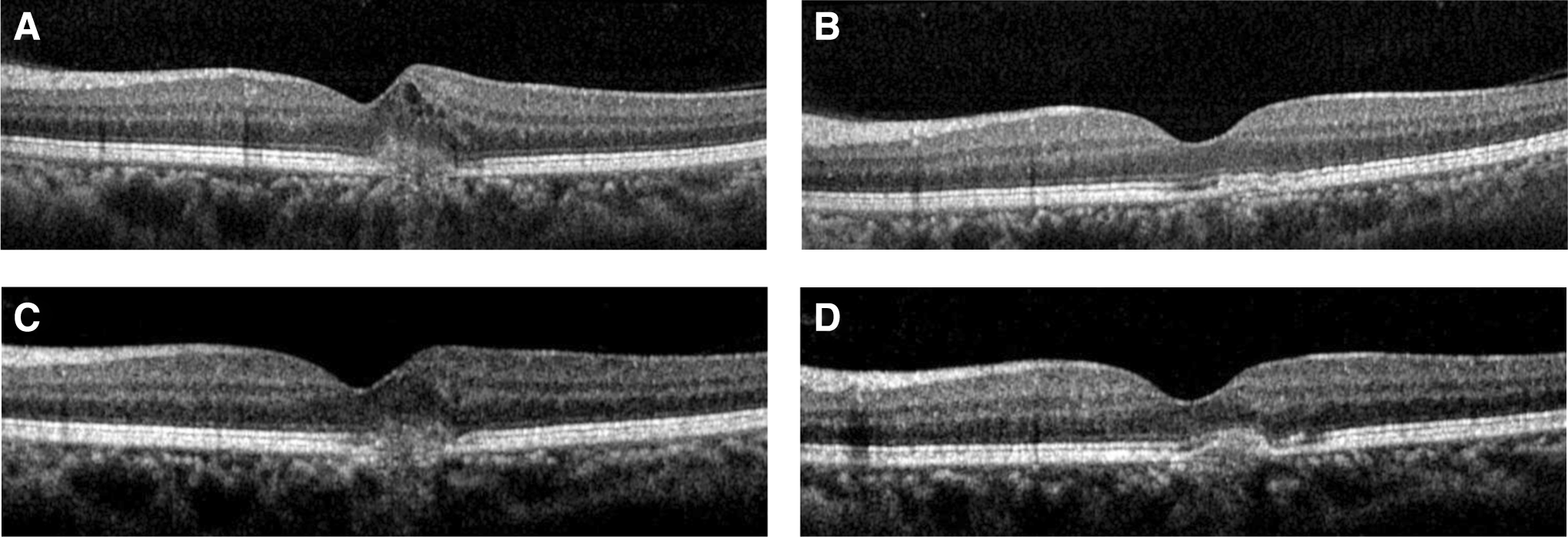
Optical coherence tomography images from a 46-year-old patient who had been diagnosed with idiopathic CNV. The BCVA had improved from 20/30 (logMAR value = 0.176) at diagnosis
Statistics analyzed using Pearson's correlation analysis.
BCVA, best-corrected visual acuity.
In the 18 eyes without CNV recurrence, the mean BCVA values at diagnosis, 6 months, 12 months, and final follow-up were 0.45 ± 0.37 logMAR, 0.27 ± 0.37 logMAR, 0.23 ± 0.36 logMAR, and 0.19 ± 0.29 logMAR, respectively (Fig. 2B). In the 8 eyes with CNV recurrence, the BCVAs were 0.55 ± 0.42 logMAR, 0.30 ± 0.36 logMAR, 0.30 ± 0.37 logMAR, and 0.21 ± 0.19 logMAR, respectively (Fig. 2B). The final BCVA did not differ between the 2 groups (P = 0.457), nor did the degree of change in BCVA (P = 0.467).
None of the patients had developed ocular complications related to the treatment, such as endophthalmitis, retinal detachment, and retinal pigment epithelial tear.
Discussion
In general, treatment outcomes of idiopathic CNV are known to be favorable. Visual acuity can be improved in the majority of eyes using either PDT12,13 or anti-VEGF therapy.5–11 In this study, we focused on the following 3 points: (1) long-term outcome of intravitreal bevacizumab treatment, as well as prognostic factors; (2) timing and incidence of CNV recurrence; and (3) the influence of recurrence on long-term visual prognosis.
In this study, the visual acuity of patients with idiopathic CNV had significantly improved after intravitreal bevacizumab. This improved visual acuity lasted throughout the mean follow-up period of 33.9 months. Consistent with the study of Sudhalkar et al., 8 subfoveal lesions and poor baseline BCVA were associated with poor visual outcome. Of these 2 factors, baseline BCVA was found to be the most significant predictor. In a 2-year follow-up study by Kang and Koh, 9 BCVA had improved during the follow-up period by a mean of 0.09 logMAR after a mean of 3.7 anti-VEGF injections. By comparison, the final visual acuity in this study was relatively poor, despite the fact that fewer injections were needed. We postulate that the CNV location influenced this difference. In the study of Kang and Koh, 9 40% of eyes were diagnosed with subfoveal CNV, whereas the proportion was 53.8% in our patients.
Previous studies have shown that multiple anti-VEGF injections are required during the follow-up period, suggesting that CNV recurs in some eyes. For instance, in a study by Kim et al., 7 a mean of 2.9 bevacizumab injections were administered during a mean follow-up period of 10.35 months. In 1-year follow-up studies, the mean number of injections has been between 2.0 and 3.2.6,8,11 In a 2-year follow-up study by Kang and Koh, 9 the mean number of anti-VEGF injections was 3.7. However, the exact timing and incidence of CNV recurrence, and its influence on long-term visual outcome, have not been reported. In this study, CNV had recurred in 30.8% of patients. The timing of the recurrence varied from 7 to 49 months after diagnosis. Although the majority of recurrences were noted within 14 months, 27% developed after 2 years. The follow-up period was significantly longer in patients who experienced recurrence than in those who did not. This study also showed that recurring CNV can be effectively treated using additional injections. In all cases, recurred fluid had completely subsided after additional bevacizumab injections, and the final visual outcome in patients with recurrence was not different from that in patients without recurrence.
Our results suggest a need for long-term follow-up of idiopathic CNV. In addition, it is helpful to warn the patients that a long-term exudation-free period does not guarantee complete cure of the disease. However, patients can also be encouraged that their visual acuity can be preserved by additional treatment after CNV recurrence.
The strength of this study was that treatment outcome was evaluated for a long term (mean 33.9 months). In addition, the timing and incidence of CNV recurrence, as well as its influence on long-term outcome, were investigated for the first time. Lastly, polypoidal choroidal vasculopathy cases, diagnosed using ICGA, were excluded from the study.
There were, however, limitations to this investigation. The study was retrospective, the sample size was small, and the initial treatment was performed at the discretion of the treating physician. Thus, 2 or 3 monthly loading injections were initially administered to some eyes, whereas only a single injection was administered to others. To date, there has been no evidence that multiple loading injections influence the treatment outcome in idiopathic CNV, including recurrence rate. Zhang et al. suggested that a single injection, followed by a wait-and-see approach, may be effective for idiopathic CNV. 6 The influence of initial number of injections on the treatment outcome requires further investigation involving more controlled study. Lastly, no strict monthly follow-up schedule, of the kind used in a previous prospective study, 6 was implemented; the follow-up schedule in our study varied between 1 and 4 months, depending on the discretion of the treating physician. Thus, detection and treatment of recurred CNV may have been delayed in some cases. Nevertheless, the final visual outcome in patients with CNV recurrence was comparable to that in patients without recurrence, thus highlighting the fact that the prognosis for idiopathic CNV is favorable, even in recurring cases.
In summary, the long-term (33.9 months) outcome of intravitreal bevacizumab treatment for idiopathic CNV was relatively favorable, with BCVA improving by ≥0.2 logMAR in 61.5% of patients. CNV had recurred in 30.8% of the patients, and the timing of recurrence varied from 7 to 49 months. Recurred fluid had completely subsided after additional bevacizumab injections, and the final visual outcome in these patients was not different from that in patients without recurrence.
Footnotes
Acknowledgment
Financial support: This study was supported by Kim's Eye Hospital Research Center.
Author Disclosure Statement
No competing financial interests exist.