
Abstract
Abstract
Purpose:
To evaluate the efficacy of switching from bevacizumab to ranibizumab in patients with diabetic macular edema (DME).
Methods:
Patients with DME who showed persistent fluid after at least 3 monthly bevacizumab injections were administered a single ranibizumab injection and were followed up after 1 month. Anatomic responders to ranibizumab were followed up monthly and administered ranibizumab injections on an as-needed basis for 3 months.
Results:
At the 1-month follow-up, mean central subfield foveal thickness (CSFT) decreased from 422 to 346 μm (P < 0.001) and mean best-corrected visual acuity (BCVA) improved from 20/49 to 20/46 (P = 0.063) in 62 enrolled eyes. Thirty-nine eyes (62.9%) were classified as anatomical responders and, after repeated ranibizumab injections (mean number: 2.6), mean CSFT improved (429–317 μm, P < 0.001) while BCVA was stabilized (20/52 to 20/48, P = 0.066) after 3 months, compared with baseline. The rate of patients who showed partial response to previous bevacizumab between anatomical responders and nonresponders to ranibizumab was compared. The results showed that the rate was significantly higher in the responder group than nonresponder group (76.9% vs. 43.5%, P = 0.008).
Conclusions:
Switching patients to ranibizumab may present a suitable option for the treatment of DME with persistent fluid after repeated bevacizumab injections. This treatment switch was more effective in eyes that showed partial response to previous bevacizumab therapy, compared with nonresponsive eyes.
Introduction
V
Three anti-VEGF agents are currently administered for the treatment of DME; ranibizumab, bevacizumab, and aflibercept. Although only ranibizumab and aflibercept are approved for this use, off-label use of bevacizumab by physicians exceeds that of the other 2 anti-VEGF agents because of its low cost and widespread availability. 6
A few studies have compared the effects of bevacizumab and ranibizumab on visual function and retinal thickness in patients with DME. Nepomuceno et al. concluded that bevacizumab and ranibizumab have similar effects on macular thickness in patients with DME 7 ; however, Ozturk et al. reported that ranibizumab resulted in a greater reduction in macular thickness. 8 Recently, a head-to-head trial was performed comparing the efficacy of intravitreal injections of aflibercept, ranibizumab, and bevacizumab for the treatment of center-involved DME. 9 When initial visual acuity loss was mild, there was no difference in the improvement of visual acuity among these 3 drugs. In cases of poorer initial visual acuity, aflibercept was superior to ranibizumab and bevacizumab in improving vision.
However, physicians should consider not only the efficacy of the drug but also several other factors such as economic burden, drug availability, and reimbursement policies in the selection of treatment options for DME. In addition, in a real clinical practice setting, it is not necessary for the treatment strategy to adhere to 1 specific drug, and switching to other drugs can achieve maximal benefit in patients with a suboptimal response to 1 agent. However, published data on the efficacy of ranibizumab for the treatment of patients with DME refractory to bevacizumab are limited. 10 Although both agents bind VEGF-A isoforms, the differences in the molecular size and pharmacokinetic parameters may produce a more effective therapeutic effect with ranibizumab in eyes that show a poor response to bevacizumab. 11
Therefore, in the current study, we evaluated the short-term efficacy of ranibizumab therapy in terms of visual function and retinal thickness in patients with DME who partially responded to or failed to respond to treatment with repeated bevacizumab injections. In addition, we aimed to identify any parameters associated with improved prognosis after this treatment switch.
Methods
We retrospectively reviewed the medical records of 50 DME patients (62 eyes) who showed persistent fluid after previous intravitreal bevacizumab injection (IVB) and who received 1–3 intravitreal ranibizumab injections (IVR), between April 2012 and August 2015, at the Seoul St. Mary's Hospital of the Catholic University of Korea. This study was approved by the Catholic Medical Center Institutional Review Board and was conducted in accordance with the tenets of the Declaration of Helsinki.
Included patients comprised those who had been diagnosed with persistent center-involved DME, defined as a central subfield foveal thickness (CSFT) >300 μm, after 3 or more consecutive 1.25 mg IVBs. All patients received their last IVB within 4–5 weeks before switching to IVR, and the changes in CSFT between the visits before and after the final IVB were below 10% in all eyes. Eyes that received intravitreal or periocular steroid therapy, focal laser, or panretinal photocoagulation in the 6 months before study enrollment were excluded. Other exclusion criteria included high myopia of >6 diopters, history of glaucoma, history of uveitis or other ocular inflammatory disease, presence of epiretinal membrane and/or vitreomacular traction, and a history of vitreoretinal surgery. In addition, eyes with active retinal neovascularization, which required panretinal photocoagulation, were excluded.
Each patient received a single IVR at a dose of 0.5 mg (0.05 mL) and was followed up after 1 month. We defined anatomic responders as patients exhibiting a dry macula and/or a reduction in CSFT of >50 μm after initial IVR. Anatomic responders were followed up at monthly intervals for 3 months and repeated injections were administered on an as-needed basis when spectral-domain optical coherence tomography (SD OCT) revealed any evidence of intraretinal and/or subretinal fluid or an increase in the CSFT of at least 50 μm from the previous visit.
All patients underwent complete ocular examination at baseline (defined as initial IVR visit) and at each visit. This included the Snellen best-corrected visual acuity (BCVA) test, dilated fundus examination with slit-lamp biomicroscopy, and SD OCT. Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany) was performed for all patients to determine the presence of fluid and automated CSFT measurements were generated using a 25-line raster scan pattern protocol. CSFT was defined as the mean retinal thickness in a 1-mm-diameter circular zone centered on the fovea. Enhanced depth imaging-OCT was conducted to determine the subfoveal choroidal thickness. The morphological patterns of DME on OCT were generally classified into diffuse retinal thickening, cystoid macular edema, or subretinal detachment by 2 independent masked observers. The level of hemoglobin A1c (HbA1c) was checked within 3–4 months before study enrollment. In comparison of CSFT values before and after the consecutive IVBs, the response to pre-enrollment IVB was divided into partial and nonresponse; a partial response was defined as a CSFT reduction of 10% or more with persistent fluid on SD OCT, and a nonresponse was defined as a CSFT reduction of <10%.
The main observed outcomes were mean BCVA and CSFT changes between baseline and monthly visits. For comparison of BCVA and CSFT with baseline values at each visit, the paired t-test with Bonferroni correction was utilized. BCVA was converted to the logarithm of the minimal angle of resolution (logMAR) values for statistical analysis. Improvement in CSFT was also assessed by the reduction ratio, calculated as follows: (initial CSFT–CSFT at 1 month)/initial CSFT × 100 (%). The differences between responders and nonresponders to ranibizumab were compared using the Mann–Whitney test for analysis of continuous variables and the chi-square test for categorical variables. A P value of <0.05 was considered to be statistically significant. Statistical analyses were performed using SPSS software v. 19.0 (SPSS, Inc., Chicago, IL).
Results
A total of 62 eyes from 50 patients with a mean age of 60.9 ± 8.8 years (range: 37–74 years) were enrolled in the study. The mean level of HbA1c was 6.7% ± 0.3% (range: 6.2%–7.5%). The mean duration of DME before receiving IVR was 20.8 ± 10.1 months (range: 6–52 months) and the patients received a mean number of 8.4 ± 2.3 IVBs (range: 6–16). Seventeen eyes had a history of intravitreal triamcinolone injection (IVTA) at least 6 months before study enrollment. A mean of 3.8 ± 0.8 (range: 3–6) consecutive IVBs were administered until the time point when the decision to change treatment from IVB to IVR was made. The baseline characteristics of the enrolled patients are shown in Table 1.
BCVA, best-corrected visual acuity; CME, cystoid macular edema; DME, diabetic macular edema; DRT, diffuse retinal thickening; F, female; HbA1c, glycated hemoglobin; IVB, intravitreal bevacizumab injection; IVR, intravitreal ranibizumab injection; IVTA, intravitreal triamcinolone injection; logMAR, logarithm of the minimal angle of resolution; M, male; OCT, optical coherence tomography.
At 1 month after initial IVR, the mean CSFT decreased from 422 ± 74 to 346 ± 67 μm compared with baseline (P < 0.001) and the mean CSFT reduction ratio was 17.6%. Mean BCVA improved from 0.39 ± 0.22 (Snellen equivalent of 20/49) to 0.36 ± 0.25 (Snellen equivalent of 20/46) compared with baseline, although statistical significance was not achieved (P = 0.063). Thirty-nine out of 62 eyes (62.9%) were classified as anatomic responders at 1 month and 8 eyes (12.9%) revealed complete fluid absorption on SD OCT (Fig. 1).

Representative OCT images of a 67-year-old woman who showed anatomic response to ranibizumab.
Figure 2 shows the CSFT and BCVA changes in 39 anatomic responders for a 3-month follow-up. The mean CSFT and BCVA of these responders were 429 ± 80 μm and 0.42 ± 0.24 (Snellen equivalent of 20/52) at baseline, respectively. Mean CSFT improved to 314 ± 49 μm at 1 month (P < 0.001) and was maintained at 2 and 3 months (325 ± 59 μm, P < 0.001; 317 ± 55 μm, P < 0.001, respectively). Mean BCVA improved to 0.38 ± 0.28 (Snellen equivalent of 20/48) at 1 month, 0.38 ± 0.27 (Snellen equivalent of 20/48) at 2 months, and 0.38 ± 0.27 (Snellen equivalent of 20/48) at 3 months, without statistical significance compared with baseline (P = 0.128, P = 0.058, and P = 0.066, respectively). Out of 39 eyes, additional IVR was administered in 31 (79.5%), 33 (84.6%), and 30 (76.9%) eyes at 1, 2, and 3 months, respectively, and the mean number of IVRs was 2.6 ± 0.6 during the 3-month follow-up period. Dry macula was achieved in 14 out of 39 eyes at least once during the follow-up period, and the required number of IVRs to achieve dry macula comprised 1 injection in 8 eyes, 2 injections in 4 eyes, and 3 injections in 2 eyes. Among these 14 eyes, recurrent intraretinal fluid accumulation was observed in 10 eyes 1 month after the visit in which the dry macula was observed.
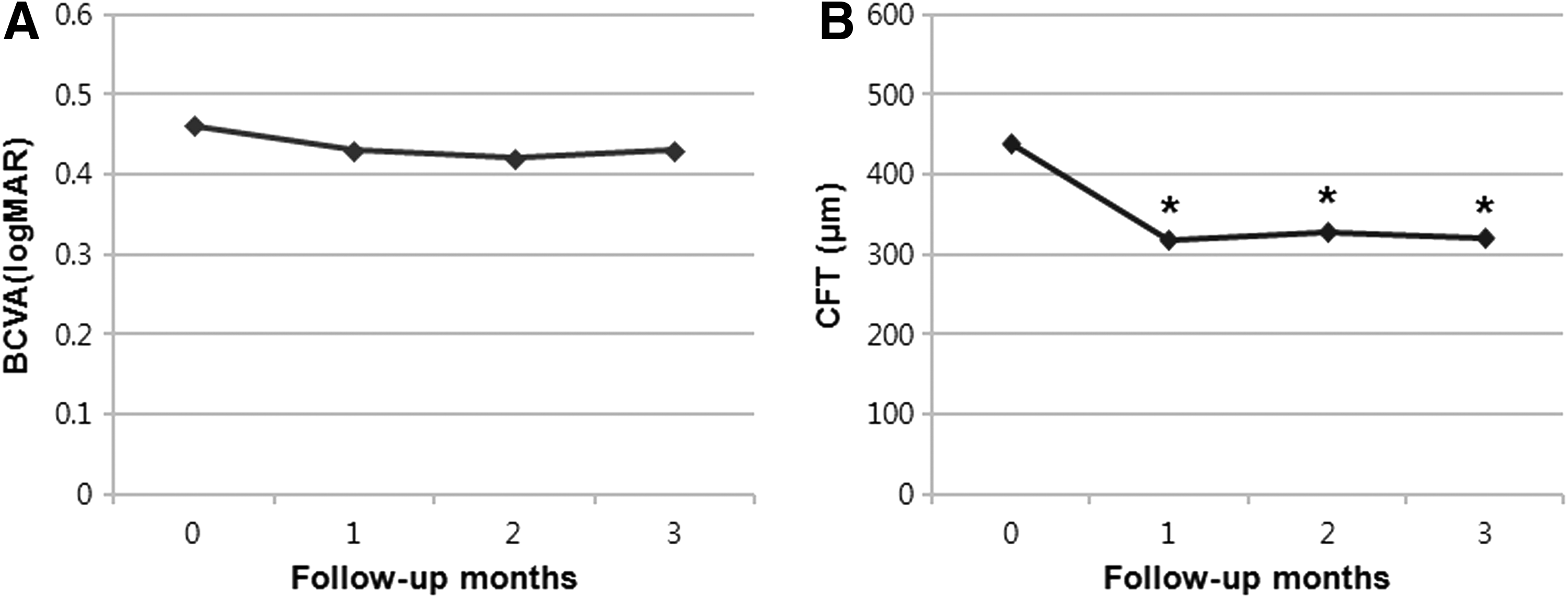
The changes in CSFT and BCVA of 39 anatomic responders during the 3-month follow-up period.
Intravitreal steroid injection was administered in 15 out of the 23 anatomic nonresponders to initial IVR (IVTA in 9 eyes, intravitreal dexamethasone implant in 6 eyes) and 11 eyes showed a reduction in CSFT of >50 μm 1 month after injection.
The effects of patient demographics and clinical characteristics on anatomic response were examined; only the response to previous IVB was related to anatomic response to IVR at 1 month (Table 2). Other factors such as presence of hypertension, level of HbA1c, history of previous treatment, duration of DME, and OCT type did not differ between the responders and nonresponders. The proportion of eyes that showed partial response to bevacizumab was significantly greater among the anatomic responders to ranibizumab compared with the nonresponders (76.9% versus 43.5%, P = 0.008). The mean CSFT reduction ratio after previous consecutive bevacizumab injections was 17.2% in the anatomic responders to ranibizumab and 7.7% in the nonresponders.
P ≤ 0.05 considered statistically significant (indicated by an asterisk).
Data are mean ± standard deviation (median, range) unless otherwise noted.
BCVA, best-corrected visual acuity; CME, cystoid macular edema; DME, diabetic macular edema; DRT, diffuse retinal thickening; HbA1c, glycated hemoglobin; IVB, intravitreal bevacizumab injection; IVR, intravitreal ranibizumab injection; IVTA, intravitreal triamcinolone injection; logMAR, logarithm of the minimal angle of resolution; OCT, optical coherence tomography.
Discussion
This retrospective observational case series investigated eyes that demonstrated persistent DME after repeated IVBs and that were subsequently switched to IVR. Mean CSFT significantly decreased after a single IVR and 62.9% of eyes were classified as anatomic responders. Anatomic improvement was maintained with repeated injections during a 3-month follow-up in these responders.
The observed anatomic benefit of switching to ranibizumab can be attributed to the pharmacokinetic/pharmacodynamic differences of the drugs and the potential of tachyphylaxis associated with prior bevacizumab treatment. Ranibizumab is an antigen-binding fragment derived from bevacizumab; it has a higher affinity for VEGF-A and a smaller size than bevacizumab. The latter is believed to enhance its diffusion from the vitreous into the retina and the choroid.11,12 These differences may translate into different clinical efficacy between the 2 medications. Similar benefits of switching from IVB to IVR have been reported in previous studies of patients with neovascular age-related macular degeneration (nAMD).13,14 However, the elevated VEGF levels in patients with DME relative to nAMD 15 provide further support to the reasoning that the continued suppression of VEGF from switching to a more potent drug may provide more benefit in DME than in nAMD. Tachyphylaxis, also well documented in previous studies on nAMD patients, 16 is another potential explanation for the results observed in the current study. Although the attenuated response occurs after repeated administration of a drug, little is known about the minimum time or number of treatments before the development of tachyphylaxis. 17 In a study by Forooghian et al., the median time to tachyphylaxis development was 100 weeks and the median number of IVBs before developing tachyphylaxis was 8 in wet AMD. 18 Therefore, due to the similar duration and number of previous treatments in the present study, tachyphylaxis may have developed in some cases. If tachyphylaxis is the reason for the effect of switching drugs, switching to bevacizumab in patients with suboptimal response to previous ranibizumab treatment might also bring further decrease in CSFT, although this has not been reported in the literature yet.
In this study, the response to previous IVB was found to be correlated with the response to IVR. Patients who showed partial response to IVB were more likely to benefit from the switch to IVR than patients with no response to IVB. This may imply that VEGF has more influence on the development of DME than other factors such as proinflammatory cytokines in patients with partial response, and vice versa in patients with no response to IVB. In addition, the mean CSFT value before IVB treatment was significantly higher in anatomic responders to IVR compared with nonresponders (530 ± 94 μm versus 454 ± 61 μm, P < 0.001, Mann–Whitney test). Reports from large randomized clinical trials have demonstrated that eyes with CSFT >400 μm at baseline showed more improvement in CSFT after ranibizumab treatment than those with CSFT of <400 μm.19,20 Several studies have found that VEGF concentrations in the vitreous and aqueous humor exhibit a strong correlation with the mean foveal thickness.21,22 Therefore, we may assume that a switch to IVR may be considered if the anatomic response to repeated IVBs is suboptimal in patients with higher baseline CSFT values. Switching to ranibizumab may lead to a further reduction in the VEGF level, which cannot be suppressed completely with bevacizumab. Hence, treatment with ranibizumab may provide anatomical and functional improvements in this subgroup of DME patients, who do not respond optimally to bevacizumab.
In the present study, the discrepancy between anatomic improvement and functional outcome may be due to the chronicity of DME (mean duration of DME: 21 months). Patients with chronic DME may already have significant photoreceptor damage and may not achieve visual improvement after anatomical improvement. 23 It is well established that delayed resolution of DME has a negative effect on the visual gains ultimately achieved. 4 In this view, an early switch to ranibizumab in IVB-resistant DME might lead to significant visual improvement. On the contrary, repeated IVBs might have achieved maximal vision improvement already, and dehydrating macular with IVR may not have additional benefit in visual outcomes in some patients.
In the present case series, 15 out of 23 nonresponders to IVR exhibited a reduction in CSFT by >50 μm after intravitreal steroid injection. Corticosteroids downregulate a variety of damaging chemokines and restore the integrity of the blood–retinal barrier, consequently decreasing DME. 24 Since anti-VEGF agents cannot change the concentration of the other proinflammatory molecules, intravitreal steroid injections have a specific role as a rescue and/or second-line therapy in patients with DME resistant to anti-VEGF treatment.
In the current study, patients received a mean number of 3.8 consecutive IVBs (a total mean of 8.4 IVBs), which may have been insufficient to evaluate the response to IVB, with more IVBs potentially resulting in further favorable responses in some cases. However, in the Ranibizumab for Edema of the Macula in Diabetes (READ-2) study, 4 ranibizumab injections over 6 months resulted in an ∼50% reduction in excess foveal thickness with a mean BCVA improvement of 7.4 letters. 25 A Diabetic Retinopathy Clinical Research Network study showed that most of the overall BCVA improvements after IVR occurred by the 8-week study visit. 20 The benefits of IVR were observed as early as 7 days after treatment initiation, signifying a very rapid effect of the anti-VEGF drugs in DME. 26 Therefore, in the present study, the limited response of the patients to a mean of 3.8 monthly IVBs may imply that they are “poor responder” to IVB candidates in real clinical practice; additional IVBs would not lead to further anatomic and functional improvement in these patients.
Other limitations of this study include a relatively small number of enrolled patients and a short follow-up period. The bevacizumab-resistant DME patients were not enrolled consecutively because of the high cost of ranibizumab. We also determined the response to ranibizumab after only a single injection and could not recommend additional IVR to nonresponders because of the economic burden. Although the effect of IVR is accepted to appear and reach its maximum value during the first month of treatment, 26 nonresponders might have had a chance to achieve a reduction in CSFT if 2 or 3 monthly IVRs had been administered consecutively. Therefore, treatment responses after switching medications should be assessed in further studies with longer follow-up periods involving repetitive injections. Also, a few reports recently demonstrated short-term efficacy of switching to aflibercept, which was not approved for the treatment of DME during the study period, in patients with incomplete response to other anti-VEGF drugs.27,28 Therefore, further studies are also warranted to identify the proper timing and candidates for switching to aflibercept in the treatment of DME. Finally, we hypothesized that the VEGF level and other inflammatory cytokine levels may differ between anatomic responders and nonresponders to IVR; this also requires evaluation in future studies.
In summary, a significant proportion of DME cases with persistent fluid on OCT, despite repeated IVBs, responded anatomically to a single IVR at 1 month, with the maintenance of benefits after 3 months among the responders. Due to a temporary therapeutic effect, repeated IVRs were required to maintain the anatomic improvement. Although significant visual improvement was not achieved in this study with chronic DME patients, minimizing the period with retinal fluid by switching to ranibizumab earlier might be advantageous in achieving maximal functional recovery in the long term. Although our results are preliminary and are based on a limited number of cases, the results of this study suggest that ranibizumab therapy can be considered as an alternative treatment on an individual basis for DME patients with persistent fluid after treatment with bevacizumab. Moreover, this study offers valuable insight in the selection of a cohort of DME patients who can benefit from switching from bevacizumab to ranibizumab. This switch is more likely to be effective in patients who showed a partial response to previous bevacizumab treatment than in nonresponders. Based on these findings, we suggest that the dynamics in CSFT during previous treatment with bevacizumab can be used to guide the decision to switch treatment to ranibizumab in the real clinic practice.
Footnotes
Author Disclosure Statement
W.K.L. has served on advisory boards for Novartis, Bayer, Allergan, Alcon, and Santen, and has received consultancy fees from these companies. He has received payments for lectures from Novartis, Bayer, Allergan, and Alcon. J.H.L. and S.E.K. have no financial disclosure to report. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria, educational grants, participation in speakers' bureaus, membership, employment, consultancies, stock ownership, or other equity interest, and expert testimony or patent-licensing arrangements) or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this article.